

We report the case of a 14-year old girl who presented with a 3-week history of cough, exertional dyspnea and orthopnea, without B symptoms. On examination she had pulsus paradoxus, an elevated jugular venous pressure at 4 cm and displaced apex beat 1–2 cm, a precordial ejection systolic murmur and pericardial rub, and widespread hash wheeze with bibasal crepitations. Chest CT scan revealed a large anterior mediastinal mass distorting the superior mediastinum. PET showed a highly avid primary mass (SUV 13.9) measuring 140 mm × 74 mm (Figure 2A). Her initial blood count showed hypercalcemia 2.68 mmol/L (normal 2.1–2.6) and high LDH 3657 U/L (normal 313–618) but was otherwise unremarkable. Bone marrow aspirate and trephine and cerebrospinal fluid were clear of disease. Histopathology showed medium-sized nuclei with prominent nucleoli and pale cytoplasm, prominent mitosis and apoptosis. Immunostain was positive for CD20 and CD79a, and occasionally CD30. ALK, CD10, CD3, TdT and myogenin were negative, consistent with primary mediastinal large B-cell lymphoma (PMBCL).
Figure 2.
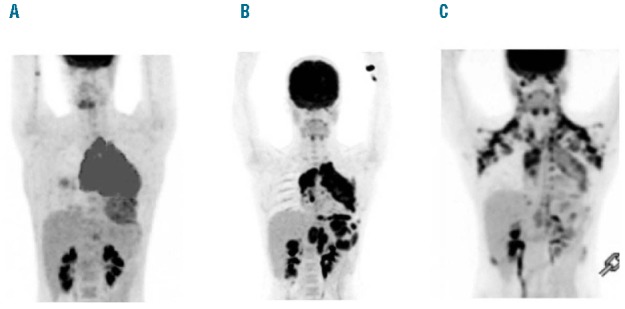
(A) Diagnostic PET scan. (B) PET scan post second-line therapy and lymphomectomy. (C) PET scan post third-line therapy with tofacitinib.
Figure 1.
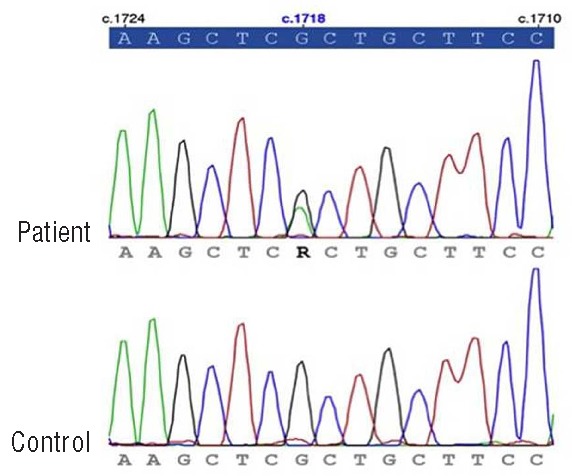
JAK3A573V variant confirmed by Sanger sequencing.
She was initially treated according to the Children’s Oncology Group protocol ANHL 1131 and received 6 cycles of dose-adapted DA-EPOCH-R (starting doses vincristine 0.4 mg/m2/day × 4 days, doxorubicin 10 mg/m2/day × 4 days, etoposide 50 mg/m2/day × 4 days, cyclophosphamide 750 mg/m2 Day 5, and prednisolone 120 mg/m2/day × 5 days, with rituximab 375 mg/m2 Day 1). Interim response assessment after 2 cycles revealed no significant metabolic or structural PET response (SUV 13.4, 127 mm × 60 mm) consistent with refractory disease. On completion of this therapy, her disease had progressed with increase of the mediastinal mass and diaphragmatic disease, as well as newly PET avid renal nodules.
Prior to second-line therapy, the mediastinal lymphoma was re-biopsied to confirm the histology and CD20 status, which were consistent. She then received 4 cycles of R/DHAP (rituximab 375 mg/m2, cisplatin 100 mg/m2, cytarabine 2 g/m2/dose for 2 doses, and dexamethasone 25 mg/m2/day for four days). On re-evaluation, her disease progressed substantially with new pericardial and para-esophageal nodal disease. At this stage, local control was planned with gross total resection of the mediastinal lymphoma with consideration for targeted re-sequencing of common cancer genes in a personalized therapeutic approach.1 In the interim, she presented with sepsis and required emergency tumor debulking due to caval compression.
DNA was isolated in five separate regions of the frozen tissue using DNeasy (Qiagen, Hilden) and subjected to amplicon-based next generation sequencing using the TruSeq Amplicon Cancer Panel (TSACP, Illumina, USA). Uniquely indexed samples were sequenced to average 3118× coverage on the Illumina MiSeq sequencer using 2× 150bp paired-end MiSeq v.2 chemistry (Illumina, San Diego, USA). TSACP comprises 212 amplicons from 48 genes covering mutation hotspots known to be frequently altered in various cancers. Probes covering the targeted region were hybridized to denatured DNA template, extended, ligated and PCR amplified incorporating bar-code sequences to facilitate multiplexing. All targets simultaneously amplified in a singletube reaction were purified manually using Agencourt AMPure XP beads (Beckman Coulter, USA). The resultant library was quantified on a Qubit Fluorometric system (Life Technologies, USA) for normalization and Tapestation 2200 (Agilent technologies, USA) for absolute quantification. Sequencing was performed on an Illumina MiSeq sequencer using 2× 150bp paired-end MiSeq v.2 chemistry. Raw reads were de-indexed, aligned and variant called using an in-house bio-informatic analysis pipeline. All tumor regions were positive for the JAK3A573V activating mutation, with variant reads ranging from 37–39% of total reads. The JAK3 mutation was confirmed by independent PCR and Sanger sequencing. JAK3A573V is a well-known activating mutation predicted to disrupt an important auto-regulatory interaction between JH2 and JH1 domains.2
Follow-up PET scan post mediastinal lymphoma resection showed gross disease progression (Figure 2B). The patient received third-line therapy with GEM-OX (gemcitabine 1.2 g/m2/day and oxaliplatin 120 mg/m2/day, both on Days 1 and 8) with a different CD20 antibody, namely ofatumumab (adult dosing; 300 mg at first dose followed by 1 gm thereafter on Days 1 and 8 of 14-day cycles). Ongoing studies have shown substitution of ofatumumab for rituximab in standard second-line regimens following failure of R-CHOP is a promising approach without additional significant toxicity.3
Given her refractory disease and proven JAK3 mutation, tofacitinib was included (adult dosing; 15 mg BD). Tofacitinib, a pan JAK inhibitor with primary effect against JAK3, has been safely used for the treatment of rheumatoid arthritis, psoriasis and other conditions.4,5 Its efficacy against lymphoma and its toxicity profile when used as combination therapy is still being evaluated.6 The PET scan at the completion of the third cycle of GEM-OX with ofatumumab and tofacitinib showed a partial metabolic response with reduction in both disease size and FDG avidity (Figure 2C). Confounding this result was adjunctive steroid use two days prior (dexamethasone 5 mg/m2/day in 2 doses) given for acute shoulder and back pain. She had a fourth cycle, followed by matched unrelated donor bone marrow transplant.
JAK/STAT signaling is aberrantly activated in lymphoma by multiple mechanisms, including inappropriate autocrine and paracrine cytokine stimulation.7 Recent studies highlight the importance of the JAK/STAT pathway for mechanisms of immune escape in lymphoma8 and it has been shown to be involved in regulating programmed cell death in a variety of tumor types, including Hodgkin lymphoma (HL), and PMBCL.9–11 JAK2-activating mutations are observed in lymphoma most commonly in PMBCL and HL.12 JAK3-activating mutations have been recently described in several lymphoproliferative disorders, including adult T-cell leukemia/lymphoma, natural killer T-cell lymphoma, cutaneous T-cell lymphoma, mantle-cell lymphoma, Burkitt lymphoma and anaplastic large cell lymphoma, but not PMBCL.13–15 To the best of our knowledge, this is the first case report of PMBCL with JAK3 mutation and the use of targeted therapy with tofacitinib.
Tofacitinib is a potent JAK inhibitor that shows nanomolar inhibitory potency against all JAK family kinases in enzyme studies, but it shows functional specificity for JAK1/3 over JAK2 in cell assays.2,14 It has been used as monotherapy in clinical trials for the treatment of rheumatoid arthritis and pre-clinical studies show promising results in sensitizing T/NK disorder cell lines to chemotherapy.6,14 There is, however, a paucity of literature for its use in PMBCL.
Whole exome sequencing has been used with success to discover somatic mutations in protein-coding genes of many hematologic malignancies, including lymphomas.14 These studies shed light on disease pathogenesis and uncover potential new therapeutic targets which are urgently needed for patients whose disease is refractory to conventional immuno-chemotherapy. In the clinic, however, a more focused approach is required to ensure that sequencing assays are delivered to clinically valid regions of cancer genes, and with an efficient turnaround time. We have used a commercial targeted cancer panel combined with a bench-top sequencing platform to promptly identify a targetable mutation in an otherwise refractory disease. Leveraging the accuracy of Illumina sequencing chemistry, the high specificity of TSACP, and the long paired-end read capability and speed of the MiSeq platform, allowed this analysis to be accomplished in days rather than months. This ability to detect actionable variants in tumor samples across a range of cancer-associated gene targets lies at the core of the revolution in personalized medicine. We have shown this in a young teenager with refractory PMBCL with an activating JAK3A573V mutation by using tofacitinib in combination with second-line immuno-chemotherapy, which resulted in partial disease response and allowed the patient to progress to allogeneic stem cell transplantation.
Acknowledgments
Dr. Fellowes is associated with the TruSeq Amplicon Cancer Panel on the Illumina website having previously performed a webinar endorsing the product.
Footnotes
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Harismendy O, Schwab RB, Bao L, Olson J, Rozenzhak S, Kotsopoulos SK, et al. Detection of low prevalence somatic mutations in solid tumors with ultra-deep targeted sequencing. Genome Biol. 2011;12(12):R124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cornejo MG, Kharas MG, Werneck MB, Le Bras S, Moore SA, Ball B, et al. Constitutive JAK3 activation induces lymphoproliferative syndromes in murine bone marrow transplantation models. Blood. 2009;113(12):2746–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Matasar MJ, Czuczman MS, Rodriguez MA, Fennessy M, Shea TC, Spitzer G, et al. Ofatumumab in combination with ICE or DHAP chemotherapy in relapsed or refractory intermediate grade B-cell lymphoma. Blood. 2013;122(4):499–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Vyas D, O’Dell KM, Bandy JL, Boyce EG. Tofacitinib: The First Janus Kinase (JAK) inhibitor for the treatment of rheumatoid arthritis. Ann Pharmacother. 2013;47(11):1524–31. [DOI] [PubMed] [Google Scholar]
- 5.Ortiz-Ibanez K, Alsina MM, Munoz-Santos C. Tofacitinib and other kinase inhibitors in the treatment of psoriasis. Actas Dermosifiliogr. 2013;104(4):304–10. [DOI] [PubMed] [Google Scholar]
- 6.Dymock BW, See CS. Inhibitors of JAK2 and JAK3: an update on the patent literature 2010 – 2012. Expert Opin Ther Pat. 2013;23(4): 449–501. [DOI] [PubMed] [Google Scholar]
- 7.Derenzini E, Younes A. Targeting the JAK-STAT pathway in lymphoma: a focus on pacritinib. Expert Opin Investig Drugs. 2013;22(6):775–85. [DOI] [PubMed] [Google Scholar]
- 8.Green MR, Monti S, Rodig SJ, Juszczynski P, Currie T, O’Donnell E, et al. Integrative analysis reveals selective 9p24.1 amplification, increased PD-1 ligand expression, and further induction via JAK2 in nodular sclerosing Hodgkin lymphoma and primary mediastinal large B-cell lymphoma. Blood. 2010;116(17):3268–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Marzec M, Zhang Q, Goradia A, Raghunath PN, Liu X, Paessler M, et al. Oncogenic kinase NPM/ALK induces through STAT3 expression of immunosuppressive protein CD274 (PD-L1, B7-H1). Proc Natl Acad Sci USA. 2008;105(52):20852–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yamamoto R, Nishikori M, Kitawaki T, Sakai T, Hishizawa M, Tashima M, et al. PD-1-PD-1 ligand interaction contributes to immunosuppressive microenvironment of Hodgkin lymphoma. Blood. 2008;111(6):3220–4. [DOI] [PubMed] [Google Scholar]
- 11.Holtick U, Vockerodt M, Pinkert D, Schoof N, Sturzenhofecker B, Kussebi N, et al. STAT3 is essential for Hodgkin lymphoma cell proliferation and is a target of tyrphostin AG17 which confers sensitization for apoptosis. Leukemia. 2005;19(6):936–44. [DOI] [PubMed] [Google Scholar]
- 12.Steidl C, Gascoyne RD. The molecular pathogenesis of primary mediastinal large B-cell lymphoma. Blood. 2011;118(10):2659–69. [DOI] [PubMed] [Google Scholar]
- 13.Elliott NE, Cleveland SM, Grann V, Janik J, Waldmann TA, Dave UP. FERM domain mutations induce gain of function in JAK3 in adult T-cell leukemia/lymphoma. Blood. 2011;118(14):3911–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Koo GC, Tan SY, Tang T, Poon SL, Allen GE, Tan L, et al. Janus kinase 3-activating mutations identified in natural killer/T-cell lymphoma. Cancer Discov. 2012;2(7):591–7. [DOI] [PubMed] [Google Scholar]
- 15.Cornejo MG, Boggon TJ, Mercher T. JAK3: a two-faced player in hematological disorders. Int J Biochem Cell Biol. 2009;41(12):2376–9. [DOI] [PMC free article] [PubMed] [Google Scholar]