

Abstract
AIM: To initially test for the content validity, comprehensibility, test-retest reliability and internal consistency reliability of the Yin-Yang Assessment Questionnaire (YY-AQ).
METHODS: The process of initial validity and reliability test covered: (1) content validation from the findings of 18 multiple-case studies, validated Yin- and Yang-deficiency assessment questionnaires, relevant literatures and registered Chinese medicine practitioners; (2) comprehension with the levels of comprehensibility for each item categorized on a 3-point scale (not comprehensible; moderately comprehensible; highly comprehensible). A minimum of three respondents selecting for each item of moderately or highly comprehensible were regarded as comprehensive; (3) test-retest reliability conducted with a 2-wk interval. The intraclass correlation coefficients (ICCs) and their 95%CIs were calculated using a two-way random effects model. Wilcoxon Signed Rank test for related samples was adopted to compare the medians of test-retest scores. An ICC value of 0.85 or higher together with P > 0.05, was considered acceptable; and (4) internal consistency of the total items was measured and evaluated by Cronbach’s coefficient alpha (α). A Cronbach’s α of 0.7 or higher was considered to represent good internal consistency.
RESULTS: Eighteen Yin-deficiency and 14 Yang-deficiency presentation items were finalized from content validation. Five participants with type 2 diabetes mellitus (T2DM) performed the comprehensibility and test-retest reliability tests. Comprehensibility score level of each presentation item was found to be moderate or high in three out of the five participants. Test-retest reliability showed that the single measure ICC of the total Yin-deficiency presentation items was 0.99 (95%CI: 0.89-0.99) and the median scores on the first and 14th days were 17 (IQR 6.5-27) and 21 (IQR 6-29) (P = 0.144) respectively. The single measure ICC of the total Yang-deficiency presentation items was 0.88 (95%CI: 0.79-0.99) and the median scores on the first and 14th days were 10 (IQR 6-18) and 14 (IQR 7-23) (P = 0.144) respectively. The results of a descriptive correlation study on 140 survey participants with T2DM using the YY-AQ showed that internal consistency of the total Yin-deficiency and Yang-deficiency presentation items was satisfactory, with Cronbach’s α of 0.79 and 0.78 respectively.
CONCLUSION: The YY-AQ will be tested further for comprehensibility, test-retest and internal consistency reliabilities, scoring system validity, construct validity, convergent and discriminant validities, responsiveness and predictive validity.
Keywords: Body constitution, Traditional Chinese medicine, Diabetes mellitus, Yin-deficiency, Yang-deficiency, Yin-Yang-deficiency, Yin-Yang assessment questionnaire, Initial validity and reliability
Core tip: Unregulated “unhealthy” body constitution (BC) with an imbalanced Yin and Yang can induce chronic diseases. Past research findings support that food has natures that can regulate the “unhealthy” BC by balancing Yin and Yang. Yin-, Yang- and Yin-Yang-deficiency are the common “unhealthy” BC types in diabetes mellitus (DM). In order to identify the “unhealthy” BC presentations, it was necessary for dieticians to develop the Yin-Yang Assessment Questionnaire for DM. It has passed the initial validation and will be tested further for construct validity, convergent and discriminant validities, responsiveness and predictive validity; scoring system validity, comprehensibility, test-retest and internal consistency reliabilities.
INTRODUCTION
From a perspective of traditional Chinese medicine (TCM), body constitution (BC) represents the health of an individual or a population in terms of the physical structure, physiological function, psychological reaction and metabolism[1,2]. BC can be classified as “healthy” and “unhealthy”. “Healthy” BC occurs in the person with a balance of Yin (cold) and Yang (hot) while an unbalanced Yin and Yang leads to “unhealthy” BC, such as Yin-deficiency and Yang-deficiency[3]. In accordance with the theory of Yin-Yang interaction in TCM, the weaker the Yin, the weaker the Yang it will be and vice versa. That is, unregulated Yin-deficiency will weaken the Yang to further change to Yin-Yang-deficiency or vice versa. Different “unhealthy” BC types, such as Yin-deficiency and Yang-deficiency can be found in association with a single disease. Likewise, the same “unhealthy” BC type can be found to be associated with different diseases[4]. Without a prompt and appropriate treatment, “unhealthy” BC will induce diseases. Studies showed that both Yin-deficiency and Yang-deficiency types of BC have a negative influence on nervous system[5], long-term memory[6], blood pressure[7], heart health[8], carcinoma[9] and sleep quality[10]. In addition, persons with Yang-deficiency are also found to have hormone abnormality[11], organ dysfunction and decreasing metabolic rate[12], accumulation of free radicals (destructive substances inside the body), declining immunity and sterility[13].
Yin-deficiency, Yang-deficiency and Yin-Yang-deficiency are commonly recognized BC types in the population of diabetes mellitus (DM)[14-17]. Empirical study found that persons with type 2 diabetes mellitus (T2DM) have the presentations of these “unhealthy” BC types (Table 1)[18]. A validated Yin/Yang-deficiency assessment questionnaire will help provide prompt assessment of “unhealthy” BC presentations so that earlier and appropriate dietary therapy can be provided to regulate the “unhealthy” BC presentations by a balance of Yin and Yang. The ultimate goal of this treatment strategy is to prevent the development of other chronic diseases.
Table 1.
Presentations of Yin-deficiency and Yang-deficiency in persons with type 2 diabetes mellitus
| 18 Yin-deficiency presentations | 14 Yang-deficiency presentations |
| I have felt excessively warm in all seasons1 | I have had an aversion to cold in all seasons1 |
| I have worn thin clothes due to feeling excessively warm | I have worn thick clothes due to my aversion to cold |
| I have intermittent hot and cold spells | I have had an aversion to strong wind |
| My face has been flushed with crimson red | I have experienced heavy sweating1 |
| I have been thin and slim1 | My body looks puffy1 |
| My palms or soles have felt hot | I have had pains on my knee, loin, shoulder, and back but feeling better with heat application1 |
| I have had tinnitus1 | I have running nose or and sneezing1 |
| I have dry cough1 | I have had clear sputum1 |
| I have experienced hot flush especially in the afternoon | I have felt comfortable with hot drink1 |
| I have experienced sweating at night1 | I needed to wake up because of my diarrhea |
| My stools have been dry and hard1 | My stools have been loose or watery1 |
| I have felt hungry even after big meals | I have had diarrhea, itchy throat or cough after intake of cold food |
| I have passed minimal volumes of urine that were yellow colored1 | I have passed large volumes of colorless urine1 |
| I have always drunk water to quench my thirst | I have experienced bland taste in my mouth1 |
| My thirst could not be relieved by frequent water intake1 | |
| My skin has been very dry1 | |
| My eyes have felt very dry | |
| My lips have felt very dry |
Presentations found in multiple-case studies[18].
There are a few validated Yin-deficiency and Yang-deficiency assessment questionnaires available in the field of TCM, such as the Traditional Chinese Medical Yang-Xu Constitutional Questionnaire (TCMYCQ)[19], the Yin-Deficiency Questionnaire 1 (Yin-DQ1)[20] and the Cold-Heat Pattern Questionnaire[21]. However, these questionnaires do not target those with DM. The TCMYCQ is applied for pregnant women while the Yin-DQ1 was developed for general patients and the Cold-Heat Pattern Questionnaire is mainly adopted in clinical trials only. In view of the unavailability of a Yin- and Yang-deficiency assessment questionnaire for persons with DM, it was necessary to develop one such instrument for three reasons. First, DM prevalence has been increasing worldwide[22]. Second, research findings showed that Yin-deficiency, Yang-deficiency and Yin-Yang-deficiency are the common types of “unhealthy” BC in DM population[14-17]. Third, if BC assessment is to be integrated into the current dietary practice in future, this specific assessment instrument would be helpful to healthcare professionals, such as dieticians, in the assessment of Yin-deficiency, Yang-deficiency or Yin-Yang-deficiency presentations for persons with DM before a Yin/Yang enhancing dietary therapy would be provided for regulating the “unhealthy” BC presentations.
MATERIALS AND METHODS
The initial validation of the Yin-Yang Assessment Questionnaire (YY-AQ) for DM is summarized in four steps (Figure 1). They are content validation, comprehension, test-retest reliability and internal consistency reliability. Scoring system was set up in between the steps of content validation and comprehension.
Figure 1.
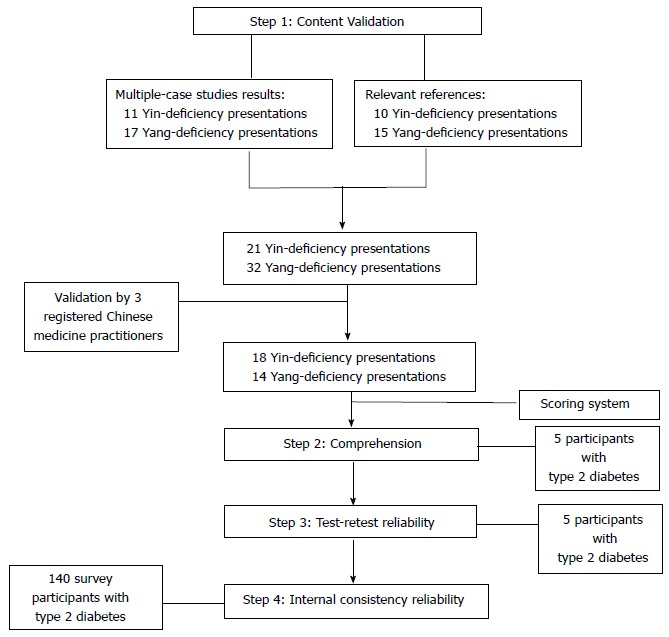
The process of developing the Yin-Yang Assessment Questionnaire.
Content validation
Content validation focuses on whether the full content of a conceptual definition is represented in the measure[23]. The YY-AQ was performed using the findings from the multiple-case studies conducted by Wong et al[18], validated Yin-deficiency and Yang-deficiency assessment questionnaires and relevant literatures.
The multiple-case studies
Between May 2013 and June 2013, 18 persons with T2DM were recruited in the multiple-case studies[18]. They were members of a non-profit organization for persons with DM. A specific characteristic of this participant group was that they all showed interests and faith in Chinese dietary therapy when asked why they liked to participate in this study. Apart from DM, all of them did not have other chronic diseases, non-diabetic medications and other medical treatments, such as kidney dialysis, chemotherapy, radiotherapy or Chinese medicine tonification. About three quarters of the 18 cases was female. The majority was aged less than 60 years. Most of the participants had more than three years of known diagnosis and were overweight. Nearly all of them were taking oral diabetic medications and their blood glucose levels were within normal range.
Each participant was assessed for BC type and presentations by a registered Chinese medicine practitioner (RCMP), who has 25 years of clinical experience in TCM, performed the TCM diagnostic technique using “Four Examinations” to collect the data with an application of the “Eight Principles of Syndrome Differentiation” to diagnose the BC type. Inter-rater reliability test was performed by two other RCMPs on five cases with a consistency rate of 80%. Eleven Yin-deficiency presentations and 17 Yang-deficiency presentations were identified from the multiple-case studies.
Procedure of content validation
First, Yin-deficiency presentation items were compiled from the multiple-case studies findings, validated Yin-DQ1[20] and two related studies[10,24]. Twenty Yin-deficiency presentation items were compiled, of which 11 items were made reference to the findings of the 18 multiple-case studies[18]. Apart from the Yin-deficiency presentations, Yang-deficiency presentations were compiled from the multiple-case studies findings, validated TCMYCQ[19] and Wang[10]’s study. Thirty-three Yang-deficiency presentation items were compiled, of which 17 items were found from the multiple-case studies findings[18]. A total of 53 presentation items were finally compiled, of which 28 (52.8%) belonged to the findings of the multiple-case studies[18]. Second, three RCMPs validated the contents of the 53 Yin-deficiency and Yang-deficiency presentation items. One of them has clinical experience for more than 25 years. The other two RCMPs, who are at PhD level in Chinese medicine, have been practising TCM for eight and 18 years respectively. The 53 presentation items were validated further into 32 items, of which 18 were Yin-deficiency type and 14 were Yang-deficiency type (Table 1). Of these 32 presentation items, 19 (53%) belonged to the findings of the multiple-case studies[18].
Scoring system
With reference to the validated TCMYCQ[19], the presentation items of Yin-deficiency and Yang-deficiency were categorized into frequency scoring system including “never”, “rare”, “occasional”, “often” and “always”. Each score was set for the respondent on a scale from 0 score (never) to 1 score (rare), 2 scores (occasional), 3 scores (often) and 4 (always) (Table 2). The higher the presentation score level, the more severe the “unhealthy” BC presentations the person has experienced. For statistical purpose, the score levels of the Yin-deficiency, Yang-deficiency and Yin-Yang-deficiency presentations were defined into low, moderate, high and very high levels using median as the cut-off point.
Table 2.
The Yin-Yang Assessment Questionnaire
| Your feelings (presentations) |
Put a "tick" if applicable |
||||
|
No |
Rare |
Occasional |
Often |
Always |
|
| 0 | (1 score) | (2 scores) | (3 scores) | (4 scores) | |
| I have felt excessively warm in all seasons1 | |||||
| I have worn thin clothes due to feeling excessively warm1 | |||||
| I have had an aversion to cold in all seasons2 | |||||
| I have worn thick clothes due to my aversion to cold2 | |||||
| I have intermittent hot and cold spells1 | |||||
| I have had an aversion to strong wind2 | |||||
| My face has been flushed with crimson red1 | |||||
| I have experienced hot flush especially in the afternoon1 | |||||
| I have experienced sweating at night1 | |||||
| My skin has been very dry1 | |||||
| My eyes have felt very dry1 | |||||
| My lips have felt very dry1 | |||||
| I have been thin and slim1 | |||||
| My body looks puffy2 | |||||
| My palms or soles have felt hot1 | |||||
| I have had pains on my knee, loin, shoulder, and back but feeling better with heat application1 | |||||
| I have running nose or and sneezing1 | |||||
| I have had tinnitus2 | |||||
| I have always drunk water to quench my thirst1 | |||||
| I have experienced heavy sweating2 | |||||
| My thirst could not be relieved by frequent water intake1 | |||||
| I have felt comfortable with hot drink2 | |||||
| I have dry cough1 | |||||
| I have had clear sputum2 | |||||
| My stools have been dry and hard1 | |||||
| My stools have been loose or watery2 | |||||
| I needed to wake up because of my diarrhea2 | |||||
| I have experienced bland taste in my mouth2 | |||||
| I have felt hungry even after big meals1 | |||||
| I have had diarrhea, itchy throat or cough after intake of cold food2 | |||||
| I have passed minimal volumes of urine that were yellow colored1 | |||||
| I have passed large volumes of colorless urine2 | |||||
Yin-deficiency presentation;
Yang-deficiency presentation.
Comprehension
Comprehension is an important procedure in the development of an instrument. It requires respondent to be able to understand the contents presented and to have the opportunity to read, evaluate and consider the content presented[25]. Five participants with T2DM were recruited and asked whether they understood the 32 presentation items from the YY-AQ. The levels of comprehensibility for each item were categorized on a 3-point scale (not comprehensible; moderately comprehensible; highly comprehensible). A minimum of three respondents selecting for each item of moderately or highly comprehensible was regarded as comprehensive.
Test-retest reliability
In order to ensure the reliability of the YY-AQ, it was necessary to ensure same score would be obtained when it would be given to the same person, under the same circumferences, but at a different time[23]. The test-retest reliability requires two administrations of the measuring instrument so as to assure stability of measurement over time. The YY-AQ was administered by five participants with T2DM with a 2-wk interval. This interval was used because the participants considered this length of time to be reasonable for time convenience. The participants completed the first YY-AQ at the recruitment. The second YY-AQ was sent to them by mail. They were requested to complete this second questionnaire on the 14th day since the completion of the first YY-AQ.
Internal consistency reliability
A measurement with a high degree of internal consistency is able to ensure all items are consistent with each other, or all working in the same direction[23]. Internal consistency estimation requires only one administration of the instrument. The YY-AQ was evaluated by a value of Cronbach’s α[26] from a descriptive correlation study on BC presentations in a sample of persons with T2DM[18].
The descriptive correlation study
One hundred and forty participants with T2DM were recruited to take part in the structured questionnaire survey between October 2013 and December 2013 after they had met the inclusion criteria: aged over 18 years; not on insulin injection and other medical treatments, such as kidney dialysis, chemotherapy or radiotherapy. Of the 140 survey participants, majority was the female. The mean age was about 65 years. Nearly half of the survey participants had more than 10 years of known diagnosis, taking either oral diabetic medications or non-diabetic medications. More than half of them had other chronic diseases, such as hypertension, heart disease, gout, cancer or liver disease. More than three quarters of the survey participants reported satisfactory blood glucose control. At the survey, each of them self-administered the YY-AQ. Completed questionnaires were then collected for data analysis of internal consistency reliability after data check by the researcher or trained helpers.
Statistical analysis
The Statistical Package for Social Sciences (SPSS, version 20, SPSS Inc., United States) was used to analyze the questionnaire data. Intraclass correlation coefficient (ICC) was used to analyze the test-retest reliability of the YY-AQ. Wilcoxon Signed Rank test for related samples was adopted to compare the median of test-retest scores. If the ICC value of 0.85 or higher together with P > 0.05 for the related samples test, the test-retest reliability of the YY-AQ was considered acceptable[27]. A Cronbach’s α of 0.7 or higher was considered to represent good internal consistency[23].
RESULTS
A total of 32 presentation items (18 Yin-deficiency items and 14 Yang-deficiency items) were validated for the YY-AQ (Table 2). Based on the cut-off point (median = 18), the score levels of the Yin-deficiency presentations questionnaire are categorized into low score (0-11 scores), moderate score (12-18 scores), high score (19-27 scores) and very high score (> 27 scores). The Yang-deficiency presentation score levels (median = 15) were set as: low score (0-10 scores), moderate score (11-15 scores), high score (16-20 scores) and very high score (> 20 scores). The Yin-Yang-deficiency scores were obtained by adding up the totals from the Yin- and Yang-deficiency scores. The Yin-Yang-deficiency score levels (median = 35) were classified as low score (0-23 scores), moderate score (24-35 scores), high score (36-48 scores) and very high score (> 48 scores) (Table 3). The results showed that more than three out of the five participants had selected each items of the YY-AQ as moderately or highly comprehensible (Table 4). Test-retest reliability showed that the single measure ICC of the total Yin-deficiency presentation items was 0.99 (95%CI: 0.89-0.99) and the median scores on the first and 14th days were 17 (IQR 6.5-27) and 21 (IQR 6-29) (P = 0.144) respectively. The single measure ICC of the total Yang-deficiency presentation items was 0.88 (95%CI: 0.79-0.99) and the median scores on the first and 14th days were 10 (IQR 6-18) and 14 (IQR 7-23) (P = 0.144) respectively. Internal consistency of the total Yin-deficiency and Yang-deficiency presentation items showed Cronbach’s α of 0.79 and 0.78 respectively.
Table 3.
Categorization of the Yin-Yang Assessment Questionnaire score levels in research setting
| Presentation |
Presentation score levels |
|||
| Low score | Moderate score | High score | Very high score | |
| Yin-deficiency (median = 18) | 0-11 | 12-18 | 19-27 | > 27 |
| Yang-deficiency (median = 15) | 0-10 | 11-15 | 16-20 | > 20 |
| Yin-Yang-deficiency (median = 35) | 0-23 | 24-35 | 36-48 | > 48 |
Table 4.
Comprehensibility of Yin-Yang Assessment Questionnaire (n = 5)
| Your feelings (presentations) | Frequency of comprehensibility | ||
| Not | Moderately | Highly | |
| I have felt excessively warm in all seasons | 0 | 4 | 1 |
| I have worn thin clothes due to feeling excessively warm | 0 | 4 | 1 |
| I have had an aversion to cold in all seasons | 0 | 3 | 2 |
| I have worn thick clothes due to my aversion to cold | 0 | 3 | 2 |
| I have intermittent hot and cold spells | 1 | 4 | 0 |
| I have had an aversion to strong wind | 1 | 4 | 0 |
| My face has been flushed with crimson red | 0 | 5 | 0 |
| I have experienced hot flush especially in the afternoon | 1 | 4 | 0 |
| I have experienced sweating at night | 0 | 5 | 0 |
| My skin has been very dry | 0 | 5 | 0 |
| My eyes have felt very dry | 0 | 5 | 0 |
| My lips have felt very dry | 1 | 4 | 1 |
| I have been thin and slim | 0 | 0 | 5 |
| My body looks puffy | 1 | 4 | 0 |
| My palms or soles have felt hot | 0 | 5 | 0 |
| I have had pains on my knee, loin, shoulder, and back but feeling better with heat application | 0 | 4 | 1 |
| I have running nose or and sneezing | 0 | 5 | 0 |
| I have had tinnitus | 0 | 0 | 5 |
| I have always drunk water to quench my thirst | 0 | 0 | 5 |
| I have experienced heavy sweating | 0 | 5 | 0 |
| My thirst could not be relieved by frequent water intake | 0 | 3 | 2 |
| I have felt comfortable with hot drink | 0 | 0 | 5 |
| I have dry cough | 1 | 4 | 0 |
| I have had clear sputum | 0 | 5 | 0 |
| My stools have been dry and hard | 0 | 0 | 5 |
| My stools have been loose or watery | 0 | 0 | 5 |
| I needed to wake up because of my diarrhea | 1 | 4 | 0 |
| I have experienced bland taste in my mouth | 1 | 4 | 0 |
| I have felt hungry even after big meals | 0 | 0 | 5 |
| I have had diarrhea, itchy throat or cough after intake of cold food | 0 | 0 | 5 |
| I have passed minimal volumes of urine that were yellow colored | 0 | 4 | 1 |
| I have passed large volumes of colorless urine | 0 | 5 | 0 |
DISCUSSION
Although the initial validation of the YY-AQ was performed in a sample of persons with T2DM, this questionnaire can also be applied to those with type 1 diabetes mellitus (T1DM) or impaired glucose tolerance (IGT). It is because DM in TCM is not treated like those in the Western medicine. Similar to other diseases, treatment variation for persons with DM is based on the syndrome differentiation and then treated accordingly with the consideration of BC[28]. As such, the YY-AQ is not an instrument for diagnosing DM but serves to assess the presentations of Yin-deficiency, Yang-deficiency and Yin-Yang-deficiency in persons with DM. It is rather an assessment instrument that can help dieticians to make early identification of “unhealthy” BC presentations in people with DM so that an appropriate Yin/Yang enhancing dietary therapy could be provided to prevent them from development of other diseases.
In applying the YY-AQ to dietetic settings including clinical and community dietetics, it may be necessary to categorize the presentation scores into low, moderate and high levels (Table 5) because it is a common practice for dieticians to set an assessment instrument into three levels. A moderate score is the basic requirement for referral to a clinical dietician. For those who get low scores, protocols for providing dietetic service can be set, such as issue of relevant information leaflet without referring to a clinical dietician. The YY-AQ is designed for self-administration or by in-person interview. This is because some respondents might possibly be unable to understand all of the question contents for two reasons. First, some of them have poor vision due to the disease. Second, older age is a key factor in understanding, so there might be difficulties for those aged above 70 years or even 60 years. Assessment of the Yin- and Yang-deficiency presentations can be incorporated into conventional dietary therapy for DM care as well as community dietetic program so that Yin-deficiency and Yang-deficiency presentations can be identified, and persons thus identified can benefit from a Yin/Yang enhancing dietary program as early as possible.
Table 5.
Categorization of the Yin-Yang Assessment Questionnaire score levels in clinical setting
| Presentation | Presentation score levels | ||
| Low score | Moderate score | High score | |
| Yin-deficiency (median = 18) | 0-11 | 12-18 | > 18 |
| Yang-deficiency (median = 15) | 0-10 | 11-15 | > 15 |
| Yin-Yang-deficiency (median = 35) | 0-23 | 24-35 | > 35 |
We have found one limitation in the initial validation study. Some presentation items are similar in the meaning. First, “I have felt excessively warm in all seasons” and “I have worn thin clothes due to feeling excessively warm” mean persistent feelings of “burning hot” even though the temperatures were generally low. It was found from crosstabs statistics and Spearman’s correlation coefficient (rho) that 55% of the 140 survey participants responded to both of these items (rho = 0.62, P = 0.000). Second, “I have had an aversion to cold in all seasons” and “I have worn thick clothes due to my aversion to cold” suggest that the respondents had experienced persistent feelings of “chilling cold” although the temperatures were general high. Of the 140 survey participants, 62% reported having both of these complaints (rho = 0.63, P = 0.000). Third, “My face has been flushed with crimson red” and “I have experienced hot flush especially in the afternoon” also mean the same thing. The results showed that 72.9% of the survey sample responded to both of the two items (rho = 0.63, P = 0.000). Fourth, “My stools have been loose or watery” also has the similar meaning to “I needed to wake up because of my diarrhea”. Of the 140 survey participants, 50% responded to both of the complaints (rho = 0.35, P = 0.008). Finally, the results showed that only 39% of the survey participants responded to both “I have always drunk water to quench my thirst” and “My thirst could not be relieved by frequent water intake” (rho = 0.4, P = 0.000). In view of the above statistical findings, the first three pairs of items could be tentatively considered for integration respectively due to being responded by over 50% of the survey participants. However, there is no “gold standard” of percentage requirement in considering the integration of items for measuring instruments. A larger sample size would be considered in the future validity and reliability study for the YY-AQ to find more substantial evidence.
In conclusion, the YY-AQ has initially passed the content validity, comprehensibility, test-retest and internal consistency reliabilities. Due to the small sample size in the tests for comprehensibility and test and retest reliability, need of a larger sample size for substantiating the need of items integration and other important validity and reliability for the YY-AQ, it is necessary to test it further for establishing its validity and reliability: comprehension if the contents are user friendly and easily understood by respondents; test-retest reliability for testing if the YY-AQ can give the same measurement to the same people with DM on different occasions; internal consistency reliability for testing the degree to which the items of the questionnaire are all measuring the same for DM; determination of the scoring system for its clinical significance; construct validity with factor analysis for testing if each item of the YY-AQ corresponds to one of the factors to be derived in the questionnaire; convergent and discriminant validities for testing the degree of the positive and negative correlation respectively between the total items and total factors to be derived in the YY-AQ; responsiveness and predictive validity; and the need of items integration.
This questionnaire is intended for use by dieticians in clinical or community settings. It will help them to early identify the Yin-deficiency or Yang-deficiency presentations in persons with DM so that a Yin/Yang enhancing dietary therapy or education program with a TCM approach can be provided for regulating the “unhealthy” BC presentations, apart from blood glucose stabilization using the nutrition approach in conventional dietary therapy. The goal of the integrated dietetic practice is to prevent the disease advancement by slowing down or preventing the development of other diseases in persons with DM, apart from stabilization of blood glucose level. Ultimately, the disease burden, such as reduced DM-related quality of life, stress of healthcare professionals and the rising healthcare cost would probably be reduced.
ACKNOWLEDGMENTS
The authors want to thank the following person and organizations for their contributions in the study: (1) Mr. Lam Chun Ho, Jaden, Statistical Officer, Quality and Safety Division, Tuen Mun Hospital, New Territories West Cluster, Hospital Authority, Hong Kong, China, for his sincere and unfailing support in the review and advice of statistical methods; and (2) the organization committee of The World Diabetes Day 2013 (venue: The Hong Kong Polytechnic University), The Society for Wong Tai Sin Diabetes Mutual Help, The Hong Kong Society for Rehabilitation New Territories West Tai Hing Centre, The Hong Kong Society for Rehabilitation New Territories Prince of Wales Centre, and The Angel of Diabetic, for their supports in the recruitments.
COMMENTS
Background
Conventional dietary therapy has its limitations in dealing with the “unhealthy” body constitution (BC) presentations by balancing one’s Yin and Yang in persons with diabetes mellitus (DM). It is because it controls blood glucose level with nutrition component only. An integration of current dietary practice and Chinese dietary approach may enhance the effectiveness on DM control as well as prevention of other diseases occurrence. In order to identify the “unhealthy” BC presentations, a validated Yin-Yang assessment questionnaire is required.
Research frontiers
The development of the Yin-Yang Assessment Questionnaire (YY-AQ) has completed its initial validation. However, it requires further test for validity and reliability.
Innovations and breakthroughs
It is comprehended that conventional dietary therapy has its limitations of regulating BC from a perspective of traditional Chinese medicine (TCM) while Chinese dietary therapy does not deal with nutrition component in the control of blood glucose. An integration of conventional dietary therapy and Chinese dietary therapy for DM care might be a future direction. The development of the YY-AQ has started a new page to the conventional dietary therapy for persons with DM.
Applications
The YY-AQ can be applied to persons with different types of DM in either clinical or community dietetic settings. In the future, this instrument could be further developed to be applied in different chronic diseases, such as hypertension.
Terminology
Yin-deficiency and Yang-deficiency are two common types of “unhealthy” BC in TCM. People with Yin-deficiency type of BC have the feelings of a “heat-dryness” due to an abnormally low level of humidity but extremely high level of temperature inside the body. Yang-deficiency is an indication of a “cold-dampness” nature of BC as a result of body humidity being at an extremely high above normal level but the body temperature is, however, extremely subnormal.
Peer-review
This study aimed to develop a Yin/Yang assessment questionnaire for persons with type 2 diabetes from a Traditional Chinese Medicine perspective. This questionnaire is intended for use by dieticians in clinical and community settings. It will help them to early make identification of the Yin- or Yang-deficiency presentations in persons with T2DM so that a Yin/Yang enhancing dietary therapy or program can be provided for regulating the unhealthy body constitution presentations.
Footnotes
Author contributions: Wong YCP performed the research, contributed to the preparation, recruited the participants, analyzed the data, wrote the manuscript and approved the manuscript; Pang MCS provided supervision on the research design, analyzed the data and contributed to editing, and finally approved the manuscript.
Conflict-of-interest statement: There is not any conflict-of-interest in conducting this study. It is because funding was not required for carrying out the initial validation test.
Data sharing statement: No additional data are available.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: January 19, 2015
First decision: April 10, 2015
Article in press: August 17, 2015
P- Reviewer: Hssan M, Panchu P, Tamemoto H S- Editor: Gong XM L- Editor: A E- Editor: Wu HL
References
- 1.Kuang DY. New version of human body constitution. Zhongyi Xuebao. 2003;21:487–488. [Google Scholar]
- 2.Wang Q. Classification of the nine body constitution types and diagnosis. Beijing Zhongyiyao. 2005;28:1–8. [Google Scholar]
- 3.Chan YP, Chien WT. Concepts of body constitution, health and sub-health from traditional Chinese medicine perspective. World J Transl Med. 2013;2:56–64. [Google Scholar]
- 4.Wang Q, Li YQ. Understanding and assessment of syndrome in Chinese medicine. Zhejiang Zhongyi Zazhi. 2006;41:623–625. [Google Scholar]
- 5.Bao HY, Yang T, Wu CY. Study of correlation between Yin-deficiency constitution and five systems of TDS. Liaoning Zhongyi Zazhi. 2012;39:598–600. [Google Scholar]
- 6.Wu BJ, Wang Y, Liu YX, Wang P. Characteristics of memory functional impairment in women with menopausal syndrome of kidney Yang-deficiency. Zhongguo Linchuang Kangfu. 2006;10:18–20. [Google Scholar]
- 7.Qiao HZ, Xing HS, Xu H, Zhang LH, Ning Q, Quang WT, Gui YZ, Cai YF. An investigation on the traditional Chinese medicine constitution of 1232 patients with slight or moderate primary hypertension in Lianyungang area. Zhongguo Zhongyi Jichu Yixue Zazhi. 2012;17:1378–1380. [Google Scholar]
- 8.Liu LL, Fan JP. Renal function of cerebral infarction patients of different ages and its relationship with Yin-deficiency. Xiandai Shengwu Yixue Jinzhan. 2010;10:3858–3861. [Google Scholar]
- 9.You J, Li TF, Wang X, Tan XW, Shan MJ. Chinese medicine syndrome classification in 303 elderly patients with primary lung cancer. Zhongyi Zazhi. 2012;53:1404–1426. [Google Scholar]
- 10.Wang Q. Understanding Your Constitution for Fitness and Health. New Taipei City: Yuen Wah; 2013. [Google Scholar]
- 11.Xu Y, Ruan XF, Jin T, Zhen HS. Preliminary study on essence of heart-kidney Yang-deficiency of chronic heart failure. Shanghai Zhongyiyao Daxue Xuebao. 2007;21:45–46. [Google Scholar]
- 12.Ye Z, Ou G, Li YZ, Yang Z. Analysis of Yang-deficiency constitution in health assessment. Guangzhou Zhongyiyao Daxue Xuebao. 2010;27:411–413. [Google Scholar]
- 13.Yan SL, Shen HC, Wang HZ, Tao Y. Research on the transportation features of kidney Yang-deficiency syndrome. Huaxi Yixue. 2012;27:537. [Google Scholar]
- 14.Si FC, Li YN. Chinese constitution distributions in diabetes mellitus and drug regulation distributions. Zhongyiyao Yanjiu. 2009:22. [Google Scholar]
- 15.Chen S, Suen W, Suen HY, Jim S. Study of 157 clinical cases of Yang-deficiency in diabetes mellitus. Zhejiang Zhongyi Zazhi. 2007;42:100–101. [Google Scholar]
- 16.Yu CW, Zhang TF, Yang LF, Wang YC. Survey of symptoms and research on body constitution in diabetes mellitus. Shandong Zhongyiyao Daxue Xuebao. 2001;25:185–188. [Google Scholar]
- 17.Zhou TH, Wang HF, To CH, Suen KM, To KL, Lee Y, Muk SK, Lo S, Wang Y, Wang YN. 217 diabetes cases in Chinese body constitutions and related causes. Beijing Zhongyiyao. 2009;28:39–40. [Google Scholar]
- 18.Wong YC, Pang WC, Chan YP. Empirical analysis of body constitution and food intake in persons with type 2 diabetes from a TCM perspective. Journal of Nutritional Therapeutics. 2014;3:67–80 [10.6000/1929-5634.2014.03.02.5]. [Google Scholar]
- 19.Wang HL, Kuo SH, Chou F, Chen LM, Chen LL, Lin WT. Reliability and validity evaluation of the traditional Chinese medicine Yang-Xu constitutional questionnaire on pregnant women. Huli Ji Jiankang Zhaogu Yanjiu. 2012;91:3–11. [Google Scholar]
- 20.Lee S, Park J, Lee H, Kim K. Development and validation of Yin-Deficiency Questionnaire. Am J Chin Med. 2007;35:11–20. doi: 10.1142/S0192415X07004576. [DOI] [PubMed] [Google Scholar]
- 21.Ryu H, Lee H, Kim H, Kim J. Reliability and validity of a cold-heat pattern questionnaire for traditional Chinese medicine. J Altern Complement Med. 2010;16:663–667. doi: 10.1089/acm.2009.0331. [DOI] [PubMed] [Google Scholar]
- 22.WHO. Country and regional data on diabetes. [Accessed. New Taipei City: Yuen Wah; 2014. p. Apr 27]. Available from: http://www.who.int/diabetes/facts/world_figures/en/ [Google Scholar]
- 23.Punch KF. Introduction to Social Research Quantitative and Qualitative Approaches. 2nd ed. London: SAGE Publications Ltd; 2007. [Google Scholar]
- 24.Shen CZ. The effect of Chinese food therapy on community dwelling middle-aged hypertensive patients with Yin-deficiency in Hangzhou. Hong Kong: The Hong Kong Polytechnic University; 2009. pp. 38–41. [Google Scholar]
- 25.Pandiya A. Readability and comprehensibility of informed consent forms for clinical trials. Perspect Clin Res. 2010;1:98–100. [PMC free article] [PubMed] [Google Scholar]
- 26.Cronbach LJ. Coefficient α and the internal structure of tests. Psychometrika. 1951;16:297–334. [Google Scholar]
- 27.Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to Their Development and Use. 3rd ed. New York: Oxford University Press; 2005. [Google Scholar]
- 28.Suen N, Lieu WK, Tsui KM, Wu SK, Ma SZ. Syndrome differentiation in diabetes. Zhongyi Xuebao. 2014;29:4. [Google Scholar]