

Abstract
Background:
Diabetes is the most prevalent metabolic disease with a growing spread rate in word wide. Short message service (SMS) is of the most common public communication networks, which have brought about a broad spectrum of applications like social, cultural and service products in the late decade. The objective of this research is, the investigate of using SMS on diabetes patients self-caring.
Methods:
In an interventional study, 228 diabetes patients have been selected from a community charity. With using of random sampling method, they were divided into two groups of 114 subjects as the control and case. The case group was sent messages reminding them about sports, caring foot, taking insulin and oral tablet for 4 weeks via mobile phone. After 4 weeks, a posttest questionnaire was completed. The data analysis was performed using a descriptive statistic, Chi-square, independent t-test, and paired t-test.
Results:
There are not significant differences between case and control groups before intervention by studied dependent variables (P > 0.05). Performance score mean of taking care of foot, sport and taking oral tablet and insulin in case group before intervention were 29.90, 10, 11.16 and 3.75 respectively and after intervention were 20.11, 41.36, 13.09 and 4.90, respectively. Furthermore, the performance scores mean difference after intervention, taking care of foot (P < 0.001), sport (P < 0.001), taking oral tablet (P = 0.020) was meaningful in case and control groups.
Conclusions:
Regarding the study results on using cell phone, to utilize virtual training methods is recommended as an appropriate procedure for different health care, self-caring and follow-up training plans for various groups in society, especially diabetic and chronic patients.
Keywords: Cell phone, diabetes, experimental, intervention, mobile phone, short message service
INTRODUCTION
Diabetes is the most prevalent metabolic disease with a growing spread rate in word wide.[1] Diabetes comes along with diverse disorders in glucose protein and lipid metabolism, and chronic blood sugar increase results in different organisms’ breakdown, malfunction, and insufficiencies.[1]
Diabetes is the cause of ¼ all new advanced kidney malfunction disability and responsible for ½ all organ am potation cases. Statistics shows that 10% hospital special care beds are devoted to diabetic patients.[2] According to World Health Organization estimation, diabetes prevalence will rise from 4% in 1995 to 5.4% in 2035.[3] The number of patients in developing countries with 170% increase will go up from 84 million to 228 million ones.[4]
To control diabetes appropriately requires the patients’ capability to take care of him/her and his/her commitment to maintaining health.[5] One of the biggest challenges diabetic patients face is how to learn living with diabetes and to control blood sugar daily. Thus, training the patients to make them capable of self-care and controlling blood sugar optimally and finally to promote life quality level is considered a meaningful part in treating diabetes.[6,7] One of the educational technologies is E-training.[8] E-training refers to an educational system in which the trainer and trainee are separated due to physical distance, but they are connected with the aid of means and tools available to them because of technology.[8] In other words, the training course content is presented using transmitted sound, image, and text.[9] One of the information and communication tools in E-health is a cell phone.[10] Short message service (SMS) is of the most common public communication networks, which have brought about a broad spectrum of applications like social, cultural and service products in the late decade.[11,12]
This study aiming to promote diabetic patients self-care through SMS gives the chance to patients to experience a new kind of communication, care, training and procedure and regarding the disease being chronic and imposing enormous costs on health and treatment system, its hoped to reduce the imposed huge burden on health and treatment system by doing research and to decrease patients suffering from diabetes lost years of life and to provide a high-quality life for the patients and their family.
METHODS
The present research is an interventional study. The study community includes diabetic patients referring to a community charity institution in Sari. Sample size has been chosen 114 in both case and control groups. Oof 114 individuals in case group, 37 persons were excluded (12 due to giving wrong telephone number, 10 due to being reluctant to continue intervention, 5 as a result of their line getting closed and 10 for lack of referring to fill in posttest questionnaire), which reached to 77 in case group on the whole and out of 114 persons in control group, 37 were excluded of the study; 27 due to not referring to complete posttest questionnaire, 10 because of giving wrong telephone number which reached to 74 in control group on the whole. Sampling was the simple random method. In this way, samples were chosen randomly using patients file number and were divided into 2 case and control groups equally.
Data collection was based on a questionnaire. This questionnaire is of diabetic patients’ self-care type. It includes two sections: Patients’ demographic information and their performance in three areas as sports, caring foot and medicine (insulin and tablet).
To measure its validity, the questionnaire was completed by 15 diabetic patients and after 7 days, it was filled in by the same patients. Intraclass correlation coefficient (ICC) was used in performance and attitude to measure reliability using ICC statistical value. ICC for attitude was 0.973 and for performance, it was 0.81 indicating the mentioned questionnaires reliability. Furthermore, data collection was carried out in 2013. Before intervention, the necessary explanations about the method were given to the selected samples and their consent was taken for intervention. The questionnaire was filled in by the case and control groups separately as a pretest. First, a training plan was held for the intervention group, and they were handed pamphlets about diabetes-intervention lasted 4 weeks. Intervention group received 3 reminding messages every 48 h (exercise, taking care of foot and medicine) through cell phone (by manually). Besides, medicine reminding messages (oral tablet and insulin) were sent to them daily. At the end of every week, telephone-based follow-up was done and the patients were asked about their satisfaction from intervention approach and also the tips sent to them through SMS and in case of being reluctant to continue intervention, they were put aside. Six weeks after the intervention, posttest questionnaire was distributed among case and control groups. Data analysis was performed by descriptive statistics, Chi-square test, independent t-test, paired t-test and using SPSS version 16 software (SPSS Inc., Chicago IL).
Ethical issues (including plagiarism, informed consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors.
RESULTS
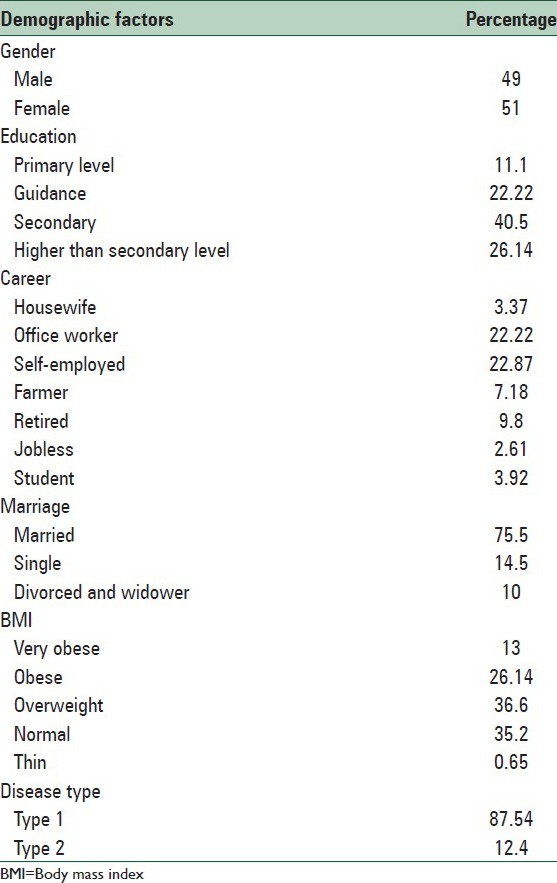
The study findings indicate that 49% of samples were women and age mean was 44.26 ± 11.2. About education, 11.1% were in primary level, 22.2% guidance and 40.5% secondary and 26.1% higher. In terms of career, 31.4% were housewives, 22.2% office workers, 22.9% self-employed, 7.2% farmers, 9.8% retired, 2.6% jobless and 3.9% students. Samples marital status, 75% were married, 14.5% single, 2.5% divorced and 7.5% widow/widower. About kind disease, 12.4% were in type 1 and 81.5% in type 2. Study samples body mass index condition, 0.13% were very obese, 26.1 obese, 36.6% overweight, 35.2% normal weight, 0.65% thin. To analyze diabetic patients’ type 1 or 2 ratio difference, data was analyzed through Chi-square test, and a significant difference was not observed [Table 1].
Table 1.
Study samples demographic characteristics
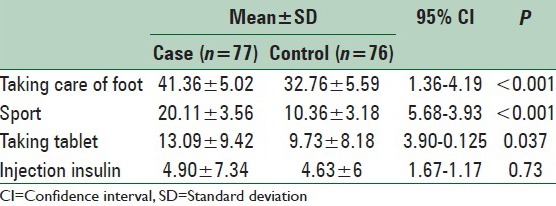
The mean and standard deviation of taking care of foot performance score before intervention in case and control groups were 22.90 ± 7.95 and 32.94 ± 6.14 and after intervention in case and control groups, they changed to 41.36 ± 5.0 and 32.76 ± 5.59. The difference of taking care of foot performance score in case and control groups with confidence interval 95% is (4.19–1.36) and the mean difference is 2.78 with P = 0.8 that this mean difference is significant. The mean and standard deviation of performance scores related to sport before intervention is case and control groups were 11.16 ± 5.04 and 11.30 ± 3.47, respectively which changed to 20.11 ± 3.56 and 1.36 ± 3.8 for case and control groups after intervention. Sport performance score difference in case and control groups with confidence interval 95% is (5.68–3.93) and mean difference is 4.8 with P < 0.001. This mean difference is significant that is sport performance level in case group is 4.8 times than that of the control group. Performance score mean and standard deviation of taking oral tablet before intervention in case and control groups was 10.68 ± 7.66 and 10.01 ± 8.21 respectively and after intervention in case and control groups, they got to 13.9 ± 9.42 and 9.37 ± 8.18 respectively. Taking oral tablet performance score difference in case and control groups with confidence interval 95% is 0.12–3.9 and mean difference is significant (P < 0.04). Taking insulin performance score mean and standard deviation in case and control groups before intervention were 3.75 ± 5.78 and 4.52 ± 6.0 respectively that changed to 4.90 ± 7.34 and 4.63 ± 6 after intervention in case and control groups, respectively. Injecting insulin performance score difference in case and control groups with confidence interval 95% is 1.67–1.17 and mean difference is 0.2 with P = 0.73 that this mean difference is not significant [Table 2].
Table 2.
Comparing mean and SD (after intervention) of diabetic patients’ self-care performance
DISCUSSION
This study was conducted to analyze the effect using SMS service has on diabetic patient's self-care referring to sari-based tabarestan diabetes charity institution. Regarding the research findings, using SMS has been effective on boosting diabetic patients’ self-care so that diabetic patients performance on taking care of foot, exercise, taking medicine and their attitude before and after intervention has been significant different.
This study results are in congruent with other similar research results. In Zolfaghari et al. comparative study on mobile message and telephone-based follow-up in diabetic (type 2) patients in both groups, median HbA1c has changed meaningfully.[13] Also in the study by Ollivier et al., SMS has been a very useful reminder and there was a significant difference between the two groups to recovery from malaria and adapting after returning to malaria indigenous region.[14] In the research by Anhøj and Møldrup on asthmatic patients through cell phone and SMS, at the end, they were all satisfied from controlling their disease using SMS.[15] The study by Gerber et al. showed that the primary feasibility and acceptability of a message text as an approach to develop healthy behaviors to maintain weight has been very influential.[16] Therefore, this study result proposing various studies reports verifies that reminding messages for diabetic patients self-care can play a positive role on patients’ self-care behaviors.
In the research by Fatehi et al. that the true answers mean in intervention group has improved meaningfully and the mean change was significant before and after intervention[17] matched with this study results. In addition, Baradaran et al., Heidari et al., in their studies obtained findings similar to the present study about attitude.[18,19] Of course, it should be noted that attitude change is one of the difficult stages of training interventions and all studies are not necessarily successful in attitude change; in the research by Shabbidar and Fathi on diabetic (type 2) patients, there was no marked difference in attitude between intervention group and control one after 3-month intervention and 3-month follow-up.[20] Of the other main variables under study in this research was patients’ performance (in exercise, taking care of foot, taking insulin and oral tablet). Based on the study results, there was a meaningful difference in studied individuals exercise performance scores mean before and after intervention. This increase implies training and applied methods effect on patients’ performance alteration. In mean and standard deviation of taking care of foot performance in case group, a meaningful difference was found before and after intervention.
According to the above mentioned findings, this study regarding diabetic people's performance change has been successful relatively. Mean difference of taking oral tablet performance had a meaningful difference in case group before and after intervention. This finding is congruent with that of the other studies such as the ones done by Nouhi, Zolfaghari, Kim, Wan Berg, Fathi and Baradaran et al. In these studies on case group performance before and after training, a meaningful statistical difference was observed in case group.[7,13,17,18] Also using SMS and high speed internet services caused an increase in taking diabetic medicine, 30-min physical exercise and persevering in diabetic patients’ care.[16] SMS is an effective tool to transfer information to diabetic people who have a cell phone. Sending educational text message through cell phone has a positive effect on patients’ knowledge.[17]
Of the limitation the present study was the large number of participants leaving the study.
CONCLUSIONS
The study results indicated that a regular and planned training program can result in promoting performance improvement in diabetic patients’ self-care. Although using virtual trainings, especially SMS is not so wide spread in health care educational programs, regarding growing increase of communication and digital gadgets and people easily accessing them, to utilize virtual educational methods is recommended as an appropriate approach for various health and self-care and follow-up training programs for diverse groups in society, particularly chronic and diabetic patients.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Backholer K, Peeters A, Herman WH, Shaw JE, Liew D, Ademi Z, et al. Diabetes prevention and treatment strategies: Are we doing enough? Diabetes Care. 2013;36:2714–9. doi: 10.2337/dc12-2501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Baan CA, van Baal PH, Jacobs-van der Bruggen MA, Verkley H, Poos MJ, Hoogenveen RT, et al. Diabetes mellitus in the Netherlands: Estimate of the current disease burden and prognosis for 2025. Ned Tijdschr Geneeskd. 2009;153:A580. [PubMed] [Google Scholar]
- 3.Bakhshian AA, Zamanzade V, Bakhshin MA, Rasouli AS, Virani F. Self-care needs of diabetic (type 2) patients referring to Tabriz-based Sina hospital diabetes clinic. Nurs Midwifery J. 2008;3:45–50. [Google Scholar]
- 4.Baghaei P, Zandi M, Vares Z, Masoudi Alavi N, Adib-Hajbaghery M. Self care situation in diabetic patients referring to Kashan Diabetes Center, in 2005. KAUMS J (FEYZ) 2008;12:88–93. [Google Scholar]
- 5.Masoudi Alavi N, Ghofranipour FA, Larijani B, Ahmadi FA, Rajab AA, Babaei GH. Analyzing the effect of community oriented care interventions implementation on Tehran diabetes control in 2003. Iran J Diabetes Lipid Disord. 2004;3:186. [Google Scholar]
- 6.Peimani M, Malazi AT, Pazhohi M. Nurses role in caring diabetes. Iran J Diabetes Lipid Disord. 2009;9:107–15. [Google Scholar]
- 7.Nouhi E, Khandan M, Mirzadeh A. Effective of electronic education on knowledge attitude and self-care in patient's diabetic type 2 refer to diabetic center of Kerman University of Medical Science. Int J Neurol Res. 2011;6:73–80. [Google Scholar]
- 8.Zolfaghari M, Mehrdad N, Parsa yekta Z, Borough NS, Bohrani N. The effect of lecture and E-learning methods on learning mother and child health course in nursing students. Iran J Med Educ. 2007;7:32. [Google Scholar]
- 9.Dargahi H, Ghazi Saeedi M. E-training position in medical science universities. Payavard Salamat. 2007;10:21. [Google Scholar]
- 10.Zandi B, Rabbani F. Congruence between SMS language and the standard Persian. Iran J Cult Res. 2009;2:48–51. [Google Scholar]
- 11.Déglise C, Suggs LS, Odermatt P. Short message service (SMS) applications for disease prevention in developing countries. J Med Internet Res. 2012;14:e3. doi: 10.2196/jmir.1823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mayor S. International Diabetes Federation consensus on prevention of type 2 diabetes. Int J Clin Pract. 2007;61:1773–5. doi: 10.1111/j.1742-1241.2007.01547.x. [DOI] [PubMed] [Google Scholar]
- 13.Zolfaghari M, Mousavifar SA, Haghani H. Mobile phone text messaging and telephone follow-up in type 2 diabetic patients for 3 months: A comparative study. J Diabetes Metab Disord. 2012;11:7. doi: 10.1186/2251-6581-11-7. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 14.Ollivier L, Romand O, Marimoutou C, Michel R, Pognant C, Todesco A, et al. Use of short message service (SMS) to improve malaria chemoprophylaxis compliance after returning from a malaria endemic area. Malar J. 2009;8:236. doi: 10.1186/1475-2875-8-236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Anhøj J, Møldrup C. Feasibility of collecting diary data from asthma patients through mobile phones and SMS (short message service): Response rate analysis and focus group evaluation from a pilot study. J Med Internet Res. 2004;6:e42. doi: 10.2196/jmir.6.4.e42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gerber BS, Stolley MR, Thompson AL, Sharp LK, Fitzgibbon ML. Mobile phone text messaging to promote healthy behaviors and weight loss maintenance: A feasibility study. Health Informatics J. 2009;15:17–25. doi: 10.1177/1460458208099865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fatehi F, Malekzadeh G, Akhavimirab A, Rashidi M, Afkhami-Ardekani M. The effect of short message service on knowledge of patients with diabetes in Yazd, Iran. Iran J Diabetes Obes. 2010;2:27–31. [Google Scholar]
- 18.Baradaran HR, Shams-Hosseini N, Noori-Hekmat S, Tehrani-Banihashemi A, Khamseh ME. Effectiveness of diabetes educational interventions in Iran: A systematic review. Diabetes Technol Ther. 2010;12:317–31. doi: 10.1089/dia.2009.0118. [DOI] [PubMed] [Google Scholar]
- 19.Heidari S, Shirazi F, Sanjari M, Salimi S, Baljani E, Tizfahm T. Analyzing effective factors on blood sugar control of diabetic (type 2) patients referring to metabolism and endocrine glands institute associated with Iran medical science university. Iran J Diabetes Lipid Disord. 2010;9:365–75. [Google Scholar]
- 20.Shabbidar S, Fathi B. Effects of nutrition education on knowledge and attitudes of type 2 diabetic patients. J Birjand Univ Med Sci. 2007;14:9–15. [Google Scholar]