

Abstract
The trial was to explore the effects of Chinese medicinal plants (CMP) treatment on the advanced endometriosis (stage III-IV) after conservative surgery. A prospective, multi-center and controlled trial was conducted from June 2012 to September 2013. Sixty-five post-operative women with advanced endometriosis (stage III-IV) after conservative surgery were included in the trial. They had undergone laparoscopic surgical excision of the endometriosis lesions and the diagnosis of endometriosis was confirmed by pathological examination. The patients received either CMP treatment or goserelin acetate sustained-release depot treatment (as comparison) according to the willingness of the patients. In the post-treatment follow-up visit at 6 and 12 months, the patients were respectively undergone ultrasonic and gynecological examinations. The serum levels of cancer antigen 125 (CA-125) and interleukin 18 (IL-18) were also detected in the post-treatment follow-up visit at 12 months. We found that in the post-treatment follow-up visit at 6 months, the recurrence rate of CMP group and comparison group was 1/31 (3.23%) and 1/34 (2.94%), respectively. In the post-treatment follow-up visit at 12 months, the recurrence rate of CMP group and comparison group was 5/31 (16.13%) and 6/34 (17.65%), respectively. There were no significant differences between the two groups (P>0.05). The serum levels of CA-125 and IL-18 significantly decreased in both of the two groups (P<0.05) and no marked differences existed between them on the serum levels of IL-18 (P>0.05). The serum CA-125 levels of CMP group were significantly lower than those of the comparison group (P<0.05). No adverse effect was reported in both of the two groups during the research and the follow-up period. It concluded that CMP showed promise in preventing the recurrence of stage III-IV endometriosis after conservative surgery, although the conclusion is somewhat limited due to the small size of the trial.
Keywords: Chinese medicinal plants (CMP), endometriosis, cancer antigen 125 (CA-125), interleukin 18 (IL-18)
Introduction
Endometriosis, firstly described in 1860 [1], is a common gynecological disease, which affects approximately 10% of reproductive-aged women and 20% to 50% of infertile women [2]. It is the third leading cause of gynecologic hospitalization in the United States [3]. Surgery is the conventional medical treatment for endometriosis with the significant short-term relief effects, however, the post-operative recurrence is common, especially for those women with advanced endometriosis (stage III-IV) [4-6].
Chinese medicinal plants (CMP) have eminent advantages in treating endometriosis [7-10]. CMP provides an alternative option that reduces the incidence rate of surgery in endometriosis patients [11]. A holistic approach of CMP and hypnotherapy was found to reduce the pain and increase birth rates of the patients with therapy-refractory endometriosis [8]. Delphi, a method defined as a series of sequential questionnaires or rounds, that seeks to gain the most reliable consensus of opinion from a group of experts [12], was applied to establish good practice guidelines for a feasibility study exploring the role of CMP in the treatment of endometriosis [13]. The Delphi process identified Qi (vital energy) and Blood stasis as the two diagnostic categories most commonly found in endometriosis, whereas Blood deficiency and Kidney Yang deficiency were also considered relatively common [13], which has provided a scientific basis to further explore the effects of CMP in treating endometriosis. However, few researches have been exclusively conducted on the effects of CMP in the post-operational treatment of endometriosis. Whether CMP has positive effects in preventing the recurrence of advanced endometriosis after conservative surgery? The prospective, multi-center and controlled trial was designed to address it.
Subjects and methods
Subjects
The prospective, multi-center and controlled trial was conducted from June 2012 to September 2013 in Women’s Hospital, School of Medicine, Zhejiang University (Hangzhou, China), the 2nd Hospital, Heilongjiang University of Chinese Medicine (Harbin, China) and the First People’s Hospital of Yuhang District (Hangzhou, China). A total of 65 post-operative women with stage III-IV endometriosis after conservative surgery were included in the trial. They had undergone laparoscopic surgical excision of the endometriosis lesions 4-6 weeks before they were recruited in the trial and the diagnosis of endometriosis was confirmed by pathological examination. All of the 65 women had no history of hypertension, heart diseases and diabetes mellitus, none of them took any hormones in the past six months before the laparoscopic surgical operation. All the patients did not suffer from any other diseases through gynecologic examinations and laboratory tests.
Group and administration
The post-operative patients with endometriosis of stage III-IV were divided into either CMP group or goserelin acetate sustained-release depot group (comparison group) according to the willingness of the patients. Having been divided, the CMP group had 31 cases and the comparison group 34 cases. Ethical approval and permission to conduct the study were obtained from the Local Ethical Committee. The aim and methodology of the study were explained to the patients. Voluntary participation was requested and informed consent was obtained. Each participant of the two groups received a physical examination, a routine blood examination, a routine uronoscopy, a liver function test and a renal function test respectively one day before the treatment started and one day after the treatment ended. In the statistical analysis, all of the women were included without missing cases during the research and the post-treatment follow-up visits at 6 and 12 months (Figure 1).
Figure 1.
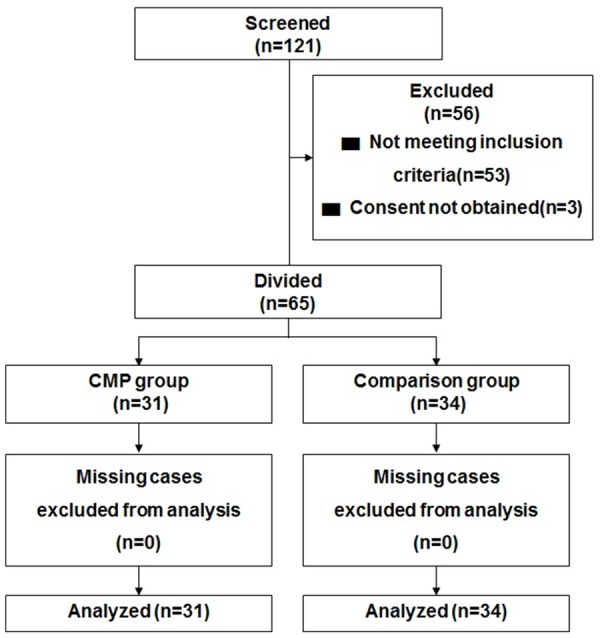
The flow chart of the progress of participants through the trial.
The formula of CMP is as follows: 30 g of Common Lophatherum, 20 g of Radix Paeoniae Rubra, 20 g of Rhizoma Curcumae and 20 g of Radix Bupleuri. All the herbs were administered within the standard dosage levels. The herbs were provided by the pharmacy departments of individual centers with a national CMP standard. The patients were instructed to orally take one dosage a day for twelve consecutive weeks. A two-week supply was dispensed at each treatment visit. Subjects were asked not to modify their dietary pattern during the research period.
The patients in the comparison group received anterior abdominal subcutaneous injection with goserelin acetate sustained-release depot (made by AstraZeneca China Pharmaceutical Co., Ltd, Wuxi, China), in the dosage of 3.6 mg once every 28 days for 12 consecutive weeks.
Index and method
All the patients completed the 12-weeks treatment. In the post-treatment follow-up visits at 6 and 12 months, the patients were respectively undergone ultrasonic and gynecological examinations. One day before the treatment and in the post-treatment follow-up visit at 12 months, the blood samples were taken and the serum levels of cancer antigen 125 (CA-125) were respectively detected by chemiluminescent assays (Abbott laboratories, PA, USA). The serum levels of interleukin 18 (IL-18) were measured by enzyme-linked immune-sorbent assay (ELISA, provided by Santa Cruz Biotechnology, Santa Cruz, CA, USA).
Data analysis
Results were analyzed by an independent university statistician using Statistical Package for Social Sciences (SPSS 16.0 for Windows), a computer software. Non-parametric Mann-Whitney tests and Analysis of variance (ANOVA) were used to analyze the data. A 5% significance level (P<0.05) and two-tailed tests were used for all hypothesis tests.
Results
The baseline characteristics
There were no significant differences between the two groups on all the baseline characteristics (P>0.05) (Table 1).
Table 1.
The baseline characteristics
| Item | Comparison group (n=34) | CMP group (n=31) |
|---|---|---|
| Age (years) | 34.79±5.24 | 32.58±4.92 |
| BMI (kg/m2) | 23.01±4.98 | 24.44±5.87 |
| Artificial abortion (cases) | 14 (41.18%) | 13 (41.94%) |
| Married/cohabitation (cases) | 19 (79.41%) | 24 (77.42%) |
| Never married (cases) | 4 (11.76%) | 3 (9.68%) |
| Women with children (cases) | 17 (50.00%) | 18 (58.06%) |
| Duration of endometriosis before operation (month) | 24.90±8.14 | 26.01±7.15 |
Notes: Data were shown as mean ± SD; * P<0.05, compared with the comparison group; CMP: Chinese medicinal plants; BMI: body mass index.
The recurrence rates of endometriosis
In post-treatment follow-up visit at 6 months, the recurrence rate of CMP group and comparison group was 1/31 (3.23%) and 1/34 (2.94%), respectively. In post-treatment follow-up visit at 12 months, the recurrence rate of CMP group and comparison group was 5/31 (16.13%) and 6/34 (17.65%), respectively. There were no significant differences between the two groups (P>0.05).
Serum levels of CA-125 and IL-18
As shown in Table 2, there were no significant differences between the two groups on the serum levels of CA-125 and IL-18 before treatment (P>0.05). In the post-treatment follow-up visit at 12 months, the serum levels of CA-125 and IL-18 were significantly decreased in both of the two groups (P<0.05) and no marked differences existed between them on the serum levels of IL-18 (P>0.05). However, the serum CA-125 levels of CMP group were significantly lower than those of the comparison group (P<0.05).
Table 2.
The serum levels of CA-125 and IL-18 before and after treatment
| Item | Comparison group (n=34) | CMP group (n=31) | ||
|---|---|---|---|---|
|
| ||||
| Pre-treatment | Post-treatment follow-up visit at 12 months | Pre-treatment | Post-treatment follow-up visit at 12 months | |
| CA-125 (U/ml) | 94.21±20.11 | 35.47±7.19# | 91.23±18.76 | 25.12±6.17*,# |
| IL-18 (pg/ml) | 103.22±24.55 | 67.11±9.13# | 109.51±23.98 | 70.01±10.98# |
Note: Data were shown as mean ± SD; CA-125: cancer antigen 125; IL-18: interleukin 18;
P<0.05, compared with the comparison group;
P<0.05, compared with pre-treatment in the same group.
Adverse result
No side-effect was reported in either of the two groups during the research and the follow-up period.
Discussion
As we know, the laparoscopic ovarian cystectomy offered the lowest risk of recurrence and the highest chance of spontaneous pregnancy rate, however, it definitely risked marked injury to the ovarian functions [14,15]. Although the surgical excision of endometriosis lesions significantly alleviated pain symptoms [16], they may recur after surgery and most of the patients were unwilling to accept a second operation [17]. Medical treatment can be used as a first line therapy to treat recurrent symptoms after surgery or prevent recurrence of the disease [18]. We found in the trial that CMP showed promise in preventing the recurrence of stage III-IV endometriosis after conservative surgery, and no side-effect was reported in either of the two groups during the research and the follow-up period.
As the most consistently studied glycoprotein in endometriosis, CA125 is more accurate in diagnosing advanced endometriosis [19-21], and a correlation existed between the CA-125 levels and the stage of endometriosis [22,23]. The serum CA-125 levels were significantly increased in the patients with ovarian and mixed endometriosis lesions compared with those who had exclusively extraovarian foci [24]. The correlation between CA-125 and the surgical as well as pathologic finding of ovarian and deep endometriosis was found to be statistically significant [24]. IL-18 is among the cytokines responsible for immune-mediated pathologies [25], which may favor the progression of endometriosis [26]. IL-18-607 A homozygote and A allele were positively correlated with the risk of developing endometriosis or the stage of endometriosis [27]. In this trial, we found that the serum levels of CA-125 and IL-18 significantly decreased in both of the two groups and no marked differences existed between them on the serum levels of IL-18, however, the serum CA-125 levels of CMP group were significantly lower than those of the comparison group. We found in the trial that CMP showed promise in preventing the recurrence of stage III-IV endometriosis after conservative surgery. However, the conclusion may be somewhat limited due to the limited patients. A large-size, randomized, multi-centre, double-blinded and placebo-controlled trials are supposed to be conducted in the future, and the involved mechanism underlying CMP preventing the recurrence of advanced endometriosis should be addressed.
Acknowledgements
This work was supported China Scholarship Council (No. 201308330139), National Natural Science Foundation of China (No. 81373674), and Zhejiang TCM Foundation (No. 2014ZA072).
Disclosure of conflict of interest
None.
References
- 1.Von Rokitansky C. Ueber uterusdrusen-neubildung in uterus and ovarilsarcomen. Z Ges Aerzte Wein. 1860;37:577–593. [Google Scholar]
- 2.Taylor RN, Lebovic DI, Mueller MD. Angiogenic factors in endometriosis. Ann N Y Acad Sci. 2002;955:89–100. doi: 10.1111/j.1749-6632.2002.tb02769.x. discussion 118, 396-406. [DOI] [PubMed] [Google Scholar]
- 3.McLeod BS, Retzloff MG. Epidemiology of endometriosis: an assessment of risk factors. Clin Obstet Gynecol. 2010;53:389–396. doi: 10.1097/GRF.0b013e3181db7bde. [DOI] [PubMed] [Google Scholar]
- 4.Sutton CJ, Pooley AS, Ewen SP, Haines P. Follow-up report on a randomized controlled trial of laser laparoscopy in the treatment of pelvic pain associated with minimal to moderate endometriosis. Fertil Steril. 1997;68:1070–1074. doi: 10.1016/s0015-0282(97)00403-2. [DOI] [PubMed] [Google Scholar]
- 5.Abbott J, Hawe J, Hunter D, Holmes M, Finn P, Garry R. Laparoscopic excision of endometriosis: a randomized, placebo-controlled trial. Fertil Steril. 2004;82:878–884. doi: 10.1016/j.fertnstert.2004.03.046. [DOI] [PubMed] [Google Scholar]
- 6.Baldi A, Campioni M, Signorile PG. Endometriosis: pathogenesis, diagnosis, therapy and association with cancer (review) Oncol Rep. 2008;19:843–846. [PubMed] [Google Scholar]
- 7.Flower A, Liu JP, Chen S, Lewith G, Little P. Chinese herbal medicine for endometriosis. Cochrane Database Syst Rev. 2009:CD006568. doi: 10.1002/14651858.CD006568.pub2. [DOI] [PubMed] [Google Scholar]
- 8.Meissner K, Bohling B, Schweizer-Arau A. Long-term effects of traditional Chinese medicine and hypnotherapy in patients with severe endometriosis--a retrospective evaluation. Forsch Komplementmed. 2010;17:314–320. doi: 10.1159/000322890. [DOI] [PubMed] [Google Scholar]
- 9.Wang DZ. [Diagnosis and treatment of endometriosis with traditional Chinese medicine] . Zhongguo Zhong Xi Yi Jie He Za Zhi. 1994;14:112–114. [PubMed] [Google Scholar]
- 10.Flower A, Liu JP, Lewith G, Little P, Li Q. Chinese herbal medicine for endometriosis. Cochrane Database Syst Rev. 2012;5:CD006568. doi: 10.1002/14651858.CD006568.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Su SY, Muo CH, Sung FC, Morisky DE. Reduction of surgery rate in endometriosis patients who take Chinese medicine: a population-based retrospective cohort study. Complement Ther Med. 2014;22:632–639. doi: 10.1016/j.ctim.2014.06.010. [DOI] [PubMed] [Google Scholar]
- 12.Powell C. The Delphi technique: myths and realities. J Adv Nurs. 2003;41:376–382. doi: 10.1046/j.1365-2648.2003.02537.x. [DOI] [PubMed] [Google Scholar]
- 13.Flower A, Lewith GT, Little P. Seeking an oracle: using the Delphi process to develop practice guidelines for the treatment of endometriosis with Chinese herbal medicine. J Altern Complement Med. 2007;13:969–976. doi: 10.1089/acm.2006.6283. [DOI] [PubMed] [Google Scholar]
- 14.Psaroudakis D, Hirsch M, Davis C. Review of the management of ovarian endometriosis: paradigm shift towards conservative approaches. Curr Opin Obstet Gynecol. 2014;26:266–274. doi: 10.1097/GCO.0000000000000078. [DOI] [PubMed] [Google Scholar]
- 15.Pergialiotis V, Vlachos D, Protopapas A, Chatzipapas I, Vlachos G. Review of the various laparoscopic techniques used in the treatment of bowel endometriosis. Minerva Ginecol. 2014;67:353–63. [PubMed] [Google Scholar]
- 16.Ford J, English J, Miles WA, Giannopoulos T. Pain, quality of life and complications following the radical resection of rectovaginal endometriosis. BJOG. 2004;111:353–356. doi: 10.1111/j.1471-0528.2004.00093.x. [DOI] [PubMed] [Google Scholar]
- 17.Borghese B, Santulli P, Streuli I, Lafay-Pillet MC, de Ziegler D, Chapron C. [Recurrence of pain after surgery for deeply infiltrating endometriosis: How does it happen? How to manage?] . J Gynecol Obstet Biol Reprod (Paris) 2014;43:12–18. doi: 10.1016/j.jgyn.2012.11.009. [DOI] [PubMed] [Google Scholar]
- 18.Hughes E, Brown J, Collins JJ, Farquhar C, Fedorkow DM, Vandekerckhove P. Ovulation suppression for endometriosis. Cochrane Database Syst Rev. 2007:CD000155. doi: 10.1002/14651858.CD000155.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Barbieri RL. CA-125 and endometriosis. Contrib Gynecol Obstet. 1987;16:103–108. [PubMed] [Google Scholar]
- 20.Patton PE, Field CS, Harms RW, Coulam CB. CA-125 levels in endometriosis. Fertil Steril. 1986;45:770–773. doi: 10.1016/s0015-0282(16)49390-8. [DOI] [PubMed] [Google Scholar]
- 21.Maiorana A, Cicerone C, Niceta M, Alio L. Evaluation of serum CA 125 levels in patients with pelvic pain related to endometriosis. Int J Biol Markers. 2007;22:200–202. doi: 10.1177/172460080702200306. [DOI] [PubMed] [Google Scholar]
- 22.Chen FP, Soong YK, Lee N, Lo SK. The use of serum CA-125 as a marker for endometriosis in patients with dysmenorrhea for monitoring therapy and for recurrence of endometriosis. Acta Obstet Gynecol Scand. 1998;77:665–670. doi: 10.1034/j.1600-0412.1998.770615.x. [DOI] [PubMed] [Google Scholar]
- 23.Rosa ESAC, Rosa ESJC, Ferriani RA. Serum CA-125 in the diagnosis of endometriosis. Int J Gynaecol Obstet. 2007;96:206–207. doi: 10.1016/j.ijgo.2006.11.016. [DOI] [PubMed] [Google Scholar]
- 24.Patrelli TS, Berretta R, Gizzo S, Pezzuto A, Franchi L, Lukanovic A, Nardelli GB, Modena AB. CA 125 serum values in surgically treated endometriosis patients and its relationships with anatomic sites of endometriosis and pregnancy rate. Fertil Steril. 2011;95:393–396. doi: 10.1016/j.fertnstert.2010.08.043. [DOI] [PubMed] [Google Scholar]
- 25.Boraschi D, Dinarello CA. IL-18 in autoimmunity: review. Eur Cytokine Netw. 2006;17:224–252. [PubMed] [Google Scholar]
- 26.Glitz C, Souza CA, Rodini GP, Genro V, Bilibio JP, Senger M, Cunha-Filho JS. Peritoneal and serum interleukin-18 levels are not increased in women with minimum or mild endometriosis. Braz J Med Biol Res. 2009;42:1039–1043. doi: 10.1590/S0100-879X2009001100007. [DOI] [PubMed] [Google Scholar]
- 27.Ayaz L, Celik SK, Cayan F, Aras-Ates N, Tamer L. Functional association of interleukin-18 gene -607 C/A promoter polymorphisms with endometriosis. Fertil Steril. 2011;95:298–300. doi: 10.1016/j.fertnstert.2010.07.1046. [DOI] [PubMed] [Google Scholar]