

Abstract
There is rare studies with regard to sesamoid bone variations of the hand in addition to its prevalence and distribution. This study aims to assess both the prevalence and variation of sesamoid bones of the hand. A retrospective review of posteroanterior (PA) and oblique radiographs of 436 left and 414 right hands of 850 adult patients obtained from four hospitals was performed. All X-ray films were examined independently for existing sesamoid bones. The presence of sesamoid bones was confirmed if oblique views revealed a small oval bone volar to the metacarpophalangeal (MCP) joint or interphalangeal (IP) joint of the thumb or finger. The X-ray films consistently revealed two sesamoid bones at the MCP joint of the thumb, and 30.4% were identified with variation, which can be classified into three distinct types based upon the number of ossification centers and the shape of fusion lines seen on standard PA and oblique films. The prevalence of sesamoid bones was 60.8% for index finger MCP joint and 59.1% for small finger MCP joint. At the thumb IP joints, sesamoid bones were only seen in 15.9% hands. Two sesamoid bones were rarely seen in other joints of the hand except thumb MCP joints.
Keywords: Sesamoid bone, variation, prevalence, hand, radiography
Introduction
Sesamoid bones are usually small ovoid shaped bones and can vary in shape and size [1]. These bones were first defined by Galen who compared them to sesame seeds [2]. Sesamoid bones are found on the palmar and plantar articular surfaces where tendons run in close proximity to bones and joints. Sesamoid bones can be embedded in tendons through dense fibrous tissue. It is thought that they play an important function as part of the lubricating mechanism, which protects the tendon and decreases friction [3].
The incidence of sesamoid bones in hands was first reported in 1892, then Bizarro systematically studied the distribution of sesamoid bones of the whole body [1], followed by several reports on sesamoid bones in the hand and feet reporting variable data especially in the hand in different populations and ethnic groups [2,4-9]. The variation of sesamoid bones has not been reported in detail, and neither similar data exist for China. This study aims to assess the prevalence and variation of sesamoid bones of the hand obtained from a multi-center population of China.
Patients and methods
A retrospective review of posteroanterior (PA) and oblique radiographic views of the hand of adult patients following hand trauma was performed. This study has been approved by the Institutional Review Board of the Third Hospital of Hebei Medical University. Informed consent was not required for this retrospective radiographic study. The original data were obtained from trauma and emergency centers of four hospitals with the use of Picture Archiving and Communication System, in four large central cities located in northern, central, eastern and southern China with high population density. Patient records or information was anonymized and re-identified prior to analysis. The data comprised all patients discharged from July 2010 to June 2011. The inclusion criteria were: patients aged 16 years and older, availability of high quality PA and oblique radiographs that demonstrate all the metacarpal and phalangeal bones of the hands including the carpus. All patients with hand pathologies, such as fractures, osteolysis, severe arthritis and calcification were excluded, as were cases with inferior radiographs and patients with clinical symptoms around the sesamoid bones.
Per protocol sesamoid bone presence had to be independently confirmed by all members of the research team which consisted of an orthopedic chief surgeon, an attending surgeon, and two radiologists. All X-rays were examined independently for existing sesamoid bones. The presence of sesamoid bones was confirmed if oblique view X-rays revealed a small oval bone volar to the MCP joint or IP joint of the thumb or finger. A consensus between all four members of the team was necessary prior to the calculation of prevalence. The sesamoid bone variation was classified based upon the number of sesamoid ossification centers and the shape of fusion lines seen on standard PA and oblique films.
The collected data included patient’s gender, age, hand laterality (right/left), location, the number of sesamoid bones, and variations of sesamoid bones. All data were recorded in spreadsheet format using Microsoft Excel 2007™.
Results
Radiographic views of 850 adult patients (679 men and 171 women) with 436 left hands and 414 right hands were included in our study. The mean age (± standard deviation) was 38.5 ± 13.5 years, with a range of 16-85 years. The distribution of sesamoid bones and prevalence in percent is shown in Table 1.
Table 1.
Distribution and incidence of sesamoid bones in 850 adult hands
| Site | Incidence (n, (%)) | Left Hand (n, (%)) | Right Hand (n, (%)) |
|---|---|---|---|
| MCP joint; I | 850 (100) | 436 (100) | 414 (100) |
| MCP joint; II | 517 (60.8) | 261 (59.9) | 256 (61.8) |
| MCP joint; III | 33 (3.9) | 18 (4.1) | 15 (3.6) |
| MCP joint; IV | 11 (1.3) | 7 (1.6) | 4 (0.9) |
| MCP joint; V | 502 (59.1) | 255 (58.5) | 247 (59.7) |
| IP joint; I | 135 (15.9) | 57 (13.1) | 78 (18.8) |
MCP: metacarpophalangeal joint; IP: interphalangeal joint; I: Thumb; II: Index Finger; III: Long finger; IV: Ring Finger; V: Small finger.
Sesamoid bones palmar to the thumb MCP joint were found in all hands. Two sesamoid bones were seen in all thumb MCP joints. Sesamoid bones were also found palmar to the index finger MCP joint in 517 hands (261 left and 256 right hands). One sesamoid bone was seen at the index MCP joint in 511 hands (257 left and 254 right hands, 511/850, 60.1%) and two were seen in 6 hands (2 left and 4 right hands, 6/850, 0.7%) (Figure 1A). Small finger sesamoid bones were seen palmar to the MCP joint in 502 hands (255 left and 247 right hands). Here one sesamoid bone was seen palmar to the MCP joint in 498 hands (252 left and 246 right hands, 498/850, 58.6%) and two were found in 4 hands (3 left and 1 right hands, 4/850, 0.5%) (Figure 1B). Sesamoid bones palmar to the middle and ring finger MCP joints were rare: the prevalence for the two locations was only 3.9% and 1.1%, respectively.
Figure 1.

The posteroanterior X-ray films of the index (A) and little fingers (B) both demonstrate two sesamoid bones (arrows) at the metacarpophalangeal (MCP) joints.
One sesamoid bone was found palmar to the thumb IP joint in 135 hands (57 left and 78 right hands) with a rate of 15.9%. None of the hands showed sesamoid bones on the palmar surface of the proximal or distal IP joints of all other fingers. Additionally, 17 sesamoid bones were found around the carpus at the following sites: 13 (1.5%) at the ulnar styloid, 2 (0.2%) volar to the scaphoid, and 2 (0.2%) at the base of the first metacarpal (Figure 2).
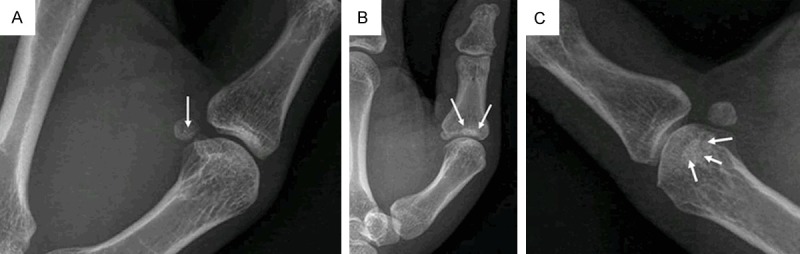
Figure 2.

The posteroanterior X-ray films show the sesamoid bones at the ulnar styloid (A), the scaphoid (B) and the base of the first metacarpal (C).
The variation of sesamoid bones palmar to the thumb MCP was detected in 30.4% (258 of 850) patients. The variations can be classified into three distinct types (Figure 3) according to the number of sesamoid ossification centers and the shape of fusion lines seen in the standard PA and oblique X-ray films (Table 2). For Type I, there were two ossification centers with one straight fusion line seen on the sesamoid bones; for Type II, there were two ossification centers with one curve fusion line; and for Type III, there were more than two ossification centers.
Figure 3.
Three types of congenital variation of sesamoid bones in the metacarpophalangeal joint of the thumb. For Type I, there were two ossification centers with one straight fusion line seen on the sesamoid bones (A); for type II, there were two ossification centers with one curve fusion line (B); and for Type III, there were more than two ossification centers (C).
Table 2.
Classification of sesamoid bone variation at the thumb MCP joint
| Type | Description | Cases | Percent (%) |
|---|---|---|---|
| I | Two ossification centers with one straight fusion line | 137 | 53.1 |
| II | Two ossification centers with one curve fusion line | 90 | 34.9 |
| III | More than two ossification centers | 31 | 12.0 |
Discussion
For this investigation, adult patients were enrolled from four regionally separated cities in China. Given the vast population size and ethnic diversity of the Chinese population, this study cannot claim to comprehensively represent the prevalence of sesamoid bones in the greater Chinese population. That said, this study demonstrates features and variations of sesamoid bone distribution in this ethnic group. This data can increase our diagnostic skills in detecting sesamoid bones. There has been no similar study to date looking at the Chinese population. Previous international studies reporting on sesamoid bones in the hand were mostly focused on the thumb MCP joint. However, there exists scarce literature on the details of distribution and variation of sesamoid bones in the whole hand.
Both prevalence and distribution of sesamoid bones at the MCP joints in the current study did not differ much from data in previous publications (Table 3). We are firmly convinced that the palmar sesamoid bones at the thumb MCP have always existed in the adult hand. They are often the source of chronic and degenerative pathologies such as trigger thumb [10], clicking thumb [11] and arthritis and can be injured during hyperextension trauma. Both sesamoid fractures as well as dislocations are well described [6,12,13]. Exact knowledge of sesamoid distribution will allow for better diagnostics and refined therapeutic approaches to pain and functional hand dysfunction. When comparing our results to published material, the prevalence of sesamoid bones in the middle and ring finger MCP joints in our collective was 3.9% and 1.3%, respectively, which were similar to findings of Dharap’s study [8], but lower than data reported by Bizzaro [1].
Table 3.
Distribution & prevalence (%) of sesamoid bones in the hand: historical comparison
| Previous study | Bizarro | Jones | Joseph | Bannister | Msamati | Dharap | Amar | Seki | Current Study |
|---|---|---|---|---|---|---|---|---|---|
| sites | 1921 | 1941 | 1951 | 1995 | 2001 | 2007 | 2011 | 2012 | 2014 |
| MCP joint; I | 98.2 | 100 | 100 | 100 | 100 | 100 | 99.5 | - | 100 |
| MCP joint; II | 64 | 45.9 | 35 | 35 | 4.8 | 40.4 | 42.3 | - | 60.8 |
| MCP joint; III | 5.3 | Rare | - | Less frequent | 0 | 2.3 | 1.4 | - | 3.9 |
| MCP joint; IV | 7.1 | Rare | - | Less frequent | 0 | 1.5 | 0.2 | - | 1.3 |
| MCP joint; V | 44.6 | 76.5 | 70 | 73 | 0 | 45.3 | 41.1 | - | 59.1 |
| IP joint; I | 22.3 | Frequent | 100 | - | 100 | 28.6 | 26.2 | 66.7 | 15.9 |
| IP joint; II | - | - | - | - | - | 0 | - | 0 | 0 |
| IP joint; III | - | - | - | - | - | 0 | - | 0.4 | 0 |
| IP joint; IV | - | - | - | - | - | 0 | - | 0.5 | 0 |
| IP joint; V | - | - | - | - | - | 0 | - | 1.1 | 0 |
MCP: metacarpophalangeal joint; IP: interphalangeal joint; I: Thumb; II: Index; Finger; III: Long finger; IV: Ring Finger; V: Small finger.
Interestingly, in our study the prevalence of sesamoid bones in the thumb IP joint was 15.9% and quite different from most reported articles. Msamati and Igbigbi [7] reported 100% incidence of a sesamoid bone at the thumb IP joint, and they confirmed the occurrence in the thumb of one sesamoid bone palmar to the IP joint. Wood and Joseph [2,5] also found similar percentages of sesamoid bones in the thumb IP joint. Amar [4], however, noted a prevalence of 26.2% in thumb IP joints, which was close to the findings by Bizzaro [1] and Dharap [8], as well as the current study. In the IP joints of all other fingers we found no sesamoid bones, which is similar to Dharap et al’s [8] data but differed with Seki et al [9] who found an incidence of 0, 0.4%, 0.5% and 1.1% in index, long, ring and small finger IP joints. The large differences in reported prevalence of sesamoid bones in the hand might be attributed to racial and genetic differences, functional necessities, or overuse of hand and fingers [4,5,7,14].
We found that sesamoid bones palmar to the thumb MCP joint commonly have variations, which may be caused by multiple ossification centers that did not unite during development resulting in a bipartite appearance [15]. We classified the variations of sesamoid bones into three types according to the number of ossification centers and the shape of fusion lines seen in standard PA and oblique view plain films. Type I is defined as two ossification centers with one straight fusion line which was found in 137 cases (53.0% of 258 cases); type II is defined by two ossification centers with one curvilinear line, present in 90 cases (34.9% of 258 cases); type III defines more than two ossification centers which was found in 31 cases (12.0% of 258 cases). The radial thumb MCP sesamoid seems to be more commonly the site of anatomical alterations. This is important in dealing with traumatic conditions. There was neither evidence nor history of fracture in any of these cases.
Fractures of the thumb sesamoid bones are a rare entity. Few reports exist on radial sided thumb sesamoid fractures. In our study, we found 8 cases of radial sided sesamoid fractures of the thumb. These must be differentiated from divided sesamoids [16]. Bipartite sesamoid bones usually present with smooth edges on radiographic images and similar contralateral findings. In contrast fractured sesamoids often demonstrate irregular bone margins. These rare traumatic pathologies are described after either direct trauma, and more commonly seen in hyperextension of the MCP joint in a young and active patient [17]. A detailed history of the initial trauma and thorough clinical examination can identify most of the sesamoid fractures. As there are usually two sesamoids of the thumb as well as bipartite sesamoids [16], radiologists must distinguish fracture fragments from normal variants.
As far as we know, only Bizzaro [1] and Amar [4] have described sesamoid bones in the carpus. In our study population we found three distinct sites in the carpus with higher prevalence of sesamoid bones: at the ulnar styloid, the scaphoid and around the base of the first metacarpal, with a respective prevalence of 1.5%, 0.2% and 0.2%, respectively. Our results were comparable to findings by Bizzaro [1], but differed with data from Amar [4]. On standard radiographs sesamoid bones can resemble ovoid nodules in carpal bones, a fact that can impede detection of additional sesamoid bones. This may be the reason for the low incidence of carpal sesamoid bones reported in literature.
There are several limitations in our study. Aside from the relatively small cohort size, for a retrospective study, there is a large heterogeneity in the distribution and variation pattern of different regions. Additionally, the description of sesamoid variation and fracture patterns in our study relied on the radiographic features seen in the standard PA and oblique radiographs, and the subjective assessment by the observers. An improved study design looking into sesamoid bone variation would be a prospective evaluation of all abnormal sesamoid bones with no history of trauma and no local symptoms using CT or MRI techniques.
Conclusions
This study reports the prevalence of sesamoid bones in the hand of Chinese adults. Two sesamoid bones are seen at all thumb MCP joints, with variation of the number of sesamoid ossification centers and the shape of fusion lines identified in 30.4% patients. The sesamoid bone variation can be classified into three distinct types based upon the number of sesamoid ossification centers and the shape of fusion lines seen in the standard PA and oblique radiographs. Two sesamoid bones can be rarely found in other joints of the hand except the thumb MCP joints.
Acknowledgements
The authors wish to thank Dr. Tao Sun and Dr. Haitao Zhao, Orthopedic surgeons, Dr. Wenjuan Wu and Xuesong Zhang, radiologists, for their assistance and cooperation in this study.
Disclosure of conflict of interest
None.
References
- 1.Bizarro AH. On Sesamoid and Supernumerary Bones of the Limbs. J Anat. 1921;55:256–268. [PMC free article] [PubMed] [Google Scholar]
- 2.Wood VE. The sesamoid bones of the hand and their pathology. J Hand Surg Br. 1984;9:261–264. doi: 10.1016/0266-7681(84)90038-x. [DOI] [PubMed] [Google Scholar]
- 3.Goldberg I, Nathan H. Anatomy and pathology of the sesamoid bones. The hand compared to the foot. Int Orthop. 1987;11:141–147. doi: 10.1007/BF00266700. [DOI] [PubMed] [Google Scholar]
- 4.Amar E, Rozenblat Y, Chechik O. Sesamoid and accessory bones of the hand--an epidemiologic survey in a Mediterranean population. Clin Anat. 2011;24:183–187. doi: 10.1002/ca.21077. [DOI] [PubMed] [Google Scholar]
- 5.Joseph J. The sesamoid bones of the hand and the time of fusion of the epiphyses of the thumb. J Anat. 1951;85:230–241. [PMC free article] [PubMed] [Google Scholar]
- 6.Mohler LR, Trumble TE. Disorders of the thumb sesamoids. Hand Clin. 2001;17:291–301. x. [PubMed] [Google Scholar]
- 7.Msamati BC, Igbigbi PS. Radiographic appearance of sesamoid bones in the hands and feet of Malawian subjects. Clin Anat. 2001;14:248–253. doi: 10.1002/ca.1042. [DOI] [PubMed] [Google Scholar]
- 8.Dharap AS, Al-Hashimi H, Kassab S, Abu-Hijleh MF. Incidence and ossification of sesamoid bones in the hands and feet: a radiographic study in an Arab population. Clin Anat. 2007;20:416–423. doi: 10.1002/ca.20378. [DOI] [PubMed] [Google Scholar]
- 9.Seki Y, Hoshino Y, Kuroda H. Prevalence of sesamoid bones in the interphalangeal joint of the thumb and fingers: a radiographic study. Clin Anat. 2013;26:823–826. doi: 10.1002/ca.22201. [DOI] [PubMed] [Google Scholar]
- 10.Seybold EA, Warhold LG. Impingement of the flexor pollicis longus tendon by an enlarged radial sesamoid causing trigger thumb: a case report. J Hand Surg Am. 1996;21:619–620. doi: 10.1016/s0363-5023(96)80013-x. [DOI] [PubMed] [Google Scholar]
- 11.Deshmukh NV, Saikia AN, Norton ER, Sonanis SV. Sesamoid displacement: a rare cause of ‘clicking thumb’. Injury. 1999;30:141–143. doi: 10.1016/s0020-1383(98)00216-2. [DOI] [PubMed] [Google Scholar]
- 12.Resnick D, Niwayama G, Feingold ML. The sesamoid bones of the hands and feet: participators in arthritis. Radiology. 1977;123:57–62. doi: 10.1148/123.1.57. [DOI] [PubMed] [Google Scholar]
- 13.Shaw M, Lyburn ID, Torreggiani WC, Watura R. Comminuted fracture of the ulnar sesamoid of the metacarpophalangeal joint of the thumb: an uncommon injury. J Emerg Med. 2003;24:437–439. doi: 10.1016/s0736-4679(03)00043-x. [DOI] [PubMed] [Google Scholar]
- 14.Sarin VK, Carter DR. Mechanobiology and joint conformity regulate endochondral ossification of sesamoids. J Orthop Res. 2000;18:706–712. doi: 10.1002/jor.1100180505. [DOI] [PubMed] [Google Scholar]
- 15.Hansen CA, Peterson TH. Fracture of the thumb sesamoid bones. J Hand Surg Am. 1987;12:269–270. doi: 10.1016/s0363-5023(87)80286-1. [DOI] [PubMed] [Google Scholar]
- 16.Hubay CA. Sesamoid bones of the hands and feet. Am J Roentgenol Radium Ther. 1949;61:493–505. [PubMed] [Google Scholar]
- 17.Patel MR, Pearlman HS, Bassini L, Ravich S. Fractures of the sesamoid bones of the thumb. J Hand Surg Am. 1990;15:776–781. doi: 10.1016/0363-5023(90)90155-k. [DOI] [PubMed] [Google Scholar]