

Abstract
Purpose
To assess the potential of dual-energy computed tomography (DECT) to identify urinary stone components, particularly uric acid and calcium oxalate monohydrate, which are unsuitable for extracorporeal shock wave lithotripsy (ESWL).
Materials and Methods
This clinical study included 246 patients who underwent removal of urinary stones and an analysis of stone components between November 2009 and August 2013. All patients received preoperative DECT using two energy values (80 kVp and 140 kVp). Hounsfield units (HU) were measured and matched to the stone component.
Results
Significant differences in HU values were observed between uric acid and nonuric acid stones at the 80 and 140 kVp energy values (p<0.001). All uric acid stones were red on color-coded DECT images, whereas 96.3% of the nonuric acid stones were blue. Patients with calcium oxalate stones were divided into two groups according to the amount of monohydrate (calcium oxalate monohydrate group: monohydrate≥90%, calcium oxalate dihydrate group: monohydrate<90%). Significant differences in HU values were detected between the two groups at both energy values (p<0.001).
Conclusions
DECT improved the characterization of urinary stone components and was a useful method for identifying uric acid and calcium oxalate monohydrate stones, which are unsuitable for ESWL.
Keywords: Calcium oxalate, Uric acid, Urinary calculi, X-ray computed tomography
INTRODUCTION
Urinary stones are composed of various components, such as calcium, uric acid, carbonate, and cystine. In the past, plain x-rays and intravenous pyelography (IVP) were the standard diagnostic tests. Since computed tomography (CT) has become widely used, noncontrast CT has become the standard test for diagnosing urinary stones owing to its higher sensitivity (94%-100% vs. 52%-87%) and specificity (92%-100% vs. 92%-100%) compared with IVP [1,2,3,4,5].
Most patients will undergo extracorporeal shock wave lithotripsy (ESWL) or endoscopic surgery if a stone is not expected to pass by medical expulsive therapy. ESWL is a minimally invasive treatment method that does not require hospitalization. More than 90% of urinary stones in adult patients are treatable with ESWL, but the success rate is affected by stone size, location, component, patient condition, and the surgeon's skill [6,7,8]. If a stone is resistant to ESWL, secondary surgical options are needed. However, this can be economically burdensome to the patient and results in a longer treatment time. Among several stone components, uric acid stones are difficult to find on ESWL x-ray images, because they are radiolucent [9]. Calcium oxalate monohydrate (COM) stones are compact and resistant to shock wave lithotripsy [10]
Many studies have been done with the aim of predicting stone components to reduce the ESWL failure rate [11,12]. However, most of these studies used conventional CT at a single energy value, which is limited for determining the details of stone composition. In this study, we predicted stone components by use of dual-energy computed tomography (DECT). We focused on uric acid stones and COM stones, because they are unsuitable for ESWL.
MATERIALS AND METHODS
A total of 246 patients with urinary stones were treated at our hospital between November 2009 and August 2013 and were included in this study. All patients who underwent surgical treatment (ureteroscopic surgery, percutaneous nephrolithotomy, retrograde intrarenal surgery) for urinary stones underwent preoperative DECT, and the components of their stones were analyzed postoperatively. Among the patients, 24 had bilateral stones. A total of 270 cases were included in this study.
Patient demographic data were collected, and the stones were collected for the component analysis. These samples were obtained via therapeutic modalities, such as percutaneous nephrolithotomy and ureteroscopic stone removal, and were analyzed by use of Fourier transform infrared spectrometry (Green Cross Corp., Yongin, Korea).
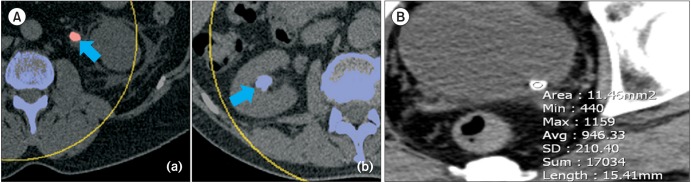
DECT (Somatom Definition Flash, Siemens Medical Solutions, Forchheim, Germany) was performed with two x-ray sources. Differences in attenuation are based on the material-dependent Compton and photo-electric effects. Stone materials can be distinguished and stone composition can be predicted by applying different x-ray spectra, because the absorption will differ depending on the stone material. Water is blue and red, and iodine is blue. We used a second-generation DECT instrument that had two energy sources. Tube A provided 140 kVp, and tube B provided 80 kVp of energy. Two readers analyzed the data with respect to stone attenuation at each energy level (x-ray diffraction analysis). Hounsfield unit (HU) values were measured by one radiology specialist using the region of interest method along the inner edge of the stones (Fig. 1). The largest diameter of the stones in the transverse plane image was defined as stone size.
Fig. 1. (A) Uric acid and nonuric acid stones in color-coded images. Dual-energy computed tomography had excellent sensitivity and accuracy for differentiating uric acid from nonuric acid stones. Uric acid stones are red in the color-coded image (a), and nonuric acid stones are blue (b) (arrow). (B) Measuring Hounsfield unit (HU) values using the region of interest (ROI) method. One radiological specialist drew a circular ROI along the inner edge of the stone to measure the HU value. An HU value of 946.33 was determined for the left uretero-vesical junction stone.
All statistical analyses were conducted with IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA) using the independent-sample t-test. A p-value <0.05 was considered significant.
RESULTS
1. Patient characteristics
The mean age of the patients was 55.6±14.2 years. A total of 179 men and 91 women were included. In total, 104 cases involved right-sided urinary tract stones, 118 cases were left-sided, and 24 cases involved both sides. Mean stone size was 8.35±5.72 mm. Stones were found in the kidney, upper ureter, mid ureter, and lower ureter in 24, 87, 41, and 118 cases, respectively (Table 1).
Table 1. Patient characteristics.
| Characteristic | Value |
|---|---|
| No. of cases | 270 |
| Age (y) | 55.6±14.2 |
| Sex | |
| Male | 179 (66.3) |
| Female | 91 (33.7) |
| Stone size (mm) | 8.35±5.72 |
| Laterality | |
| Right | 104 |
| Left | 118 |
| Both | 24 |
| Location | |
| Kidney | 24 (8.9) |
| Upper ureter | 87 (32.2) |
| Mid ureter | 41 (15.2) |
| Lower ureter | 118 (43.7) |
Values are presented as mean±standard deviation or number (%).
2. Stone components
Uric acid stones were found in 79 cases and nonuric acid stones were found in 191 cases. Mean age was not significantly different between these groups (uric acid: 61.6±14.3 years vs. nonuric acid: 53.5±13.6 years). Sixty-eight cases were men and 11 were women in the uric acid stone group and 111 cases were men and 80 were women in the nonuric acid stone group. Mean uric acid stone size was 9.03±4.51 mm and that of nonuric acid stones was 8.10±6.09 mm (p>0.05).
A total of 135 cases had calcium stones. We excluded calcium stones mixed with other components, such as uric acid and carbonate. The COM stone group (n=92) had >90% monohydrate content (group 1), whereas the calcium oxalate dehydrate stone group (n=43) had <90% monohydrate content (group 2). No significant difference in mean age was detected between these two groups (54.4±11.9 years vs. 49.1±13.2 years, respectively). Mean stone size was 7.04±3.47 mm in group 1 and 6.81±6.33 mm in group 2 (p>0.05).
3. DECT findings
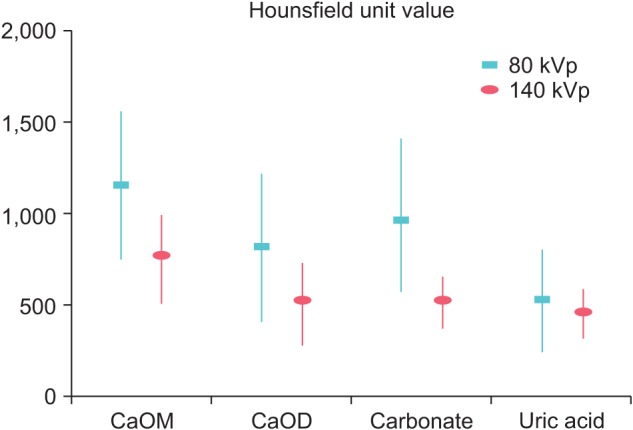
The HU values of the stones differed by their main component in the 80- and 140-kVp images. The mean HU values of the COM, COM+dihydrate, carbonate apatite, and uric acid stones were 1,190.20, 793.69, 961.73, and 511.47 on the 80-kVp images and 753.21, 510.82, 508.35, and 481.98 on the 140-kVp images, respectively (Fig. 2).
Fig. 2. Mean Hounsfield unit (HU) values for stones based on the energy used. Different HU values were measured on 80 and 140 kVp images of each stone. CaOM, calcium oxalate monohydrate; CaOD, calcium oxalate monohydrate+dihydrate; Carbonate, carbonate apatite.
Mean HU values of the uric acid stone group were 511.47 on the 80-kVp image and 481.98 on the 140-kVp image, whereas those in the nonuric acid stone group were 1,099.27 on the 80-kVp image and 706.10 on the 140-kVp image. The HU values were significantly different at each energy value (p<0.001) (Table 2). In addition, all uric acid stones were red on dual-energy color-coded images, whereas 184 nonuric acid stones (96.3%) were blue (Fig. 1A).
Table 2. Characteristics of uric acid stones vs nonuric acid stones.
| Variable | Total | Uric acid | Nonuric acid | p-value |
|---|---|---|---|---|
| No. of cases | 270 | 79 | 191 | |
| Age (y) | 55.6±14.2 | 61.6±14.3 | 53.5±13.6 | <0.001 |
| Sex | <0.001 | |||
| Male | 179 | 68 | 111 | |
| Female | 91 | 11 | 80 | |
| Stone size (mm) | 8.35±5.72 | 9.03±4.51 | 8.10±6.09 | 0.262 |
| HU value (kVp) | ||||
| 80 | 943.96±516.47 | 511.47±233.43 | 1,099.27±502.05 | <0.001 |
| 140 | 646.88±294.9 | 481.98±152.52 | 706.10±311.11 | <0.001 |
| Color-coded Image | Red (100%) | Blue (96.3%) |
Values are presented as mean±standard deviation unless otherwise indicated.
HU, Hounsfield units.
The mean HU values for the calcium oxalate stones in group 1 were 1,190.20 (±445.23) on the 80-kVp image and 753.21 (±239.33) on the 140-kVp image, whereas they were 793.69 (±413.55) on the 80-kVp image and 510.82 (±225.43) on the 140-kVp image in group 2. The HU values were significantly different for the two energy values according to monohydrate content (p<0.001) (Table 3).
Table 3. COM stones group (monohydrate≥90%) vs. COD stones group (monohydrate<90%).
| Variable | Total | COM group | COD group | p-value |
|---|---|---|---|---|
| No. of cases | 135 | 92 | 43 | |
| Age (y) | 52.6±12.5 | 54.4±11.9 | 49.1±13.2 | 0.026 |
| Sex | 0.849 | |||
| Male | 78 | 52 | 26 | |
| Female | 57 | 40 | 17 | |
| Laterality | ||||
| Right | 62 | 40 | 22 | 0.548 |
| Left | 63 | 43 | 20 | 0.403 |
| Both | 10 | 9 | 1 | 0.951 |
| Stone size (mm) | 6.96±4.60 | 7.04±3.47 | 6.81±6.33 | 0.796 |
| HU value (kVp) | ||||
| 80 | 1,059.07±472.10 | 1,190.20±445.23 | 793.69±413.55 | <0.001 |
| 140 | 673.05±260.44 | 753.21±239.33 | 510.82±225.43 | <0.001 |
Values are presented as mean±standard deviation unless otherwise indicated.
COM, calcium oxalate monohydrate; COD, calcium oxalate dehydrate; HU, Hounsfield units.
DISCUSSION
Urinary stones are one of the most common urological diseases but require active treatment owing to higher recurrence rates and various complications. Although the success rates of treatment have improved, additional treatments are frequently required. This can waste time and money and frustrate clinicians and patients. Although ESWL is the preferred treatment for urinary stones and has a high success rate, ESWL-resistant stones are not rare [13,14].
In particular, uric acid stones are radiolucent and difficult to find on ESWL x-ray images. The ESWL success rate of these stones is lower than average [15]. COM stones are a typical ESWL-resistant stone. The ESWL success rate for these stones is 36.4% [16].
Thus, it is very important to identify the stone components to determine the most effective treatment modality. Most studies that have predicted stone components have used single-energy 120-kVp CT, which reports one HU value. Some prospective CT studies have measured HU before treatment. Ouzaid et al. [13] reported that ESWL stone-free rates for stones <970 HU and ≥970 HU are 96% and 38%, respectively. Nakasato et al. [14] reported that ESWL treatment success rates are significantly higher for stones <815 HU than for stones >815 HU.
Single-energy CT has been used to detect uric acid stones in vivo and in vitro [17,18,19,20,21]. However, it may not be able to predict the exact stone components. For example, distinguishing between calcium and struvite stones is difficult because of the overlapping spectra of these stones [22]. The most important issue is that single-energy CT cannot differentiate COM stones, ESWL-resistant stones, from calcium oxalate dihydrate stones.
Recently, DECT has been performed for patients with urinary stones [18,19,20,23]. DECT uses two energy sources of 80 and 140 kVp. Some machines use 100 and 140 kVp. A contrast medium is not used for urinary stone imaging, and the spectrum of the stone itself is reflected. HU values are measured differently depending on the energy used [11,12]. CT shows a high diagnostic ability to differentiate uric acid stones from nonuric acid stones [18,20]. Although both DECT and single-energy CT are useful for diagnosing uric acid stones, the diagnostic rate of these stones is 40% with single-energy CT and 93% with DECT [24].
However, many clinicians worry about the radiation hazard of DECT. In DECT, a slightly increased radiation dose is delivered to the patient compared with the standard single-energy CT protocol [25,26]. To reduce the radiation hazard, Stolzmann et al. [27] used a tin filter to reduce the radiation dose. Jepperson et al. [28] reported that DECT using 80/140 and 100/140 kVp protocols provides information on the stone components and anatomic information provided by single-energy CT without increasing radiation exposure to the patient and with a minimal impact on image noise.
Another limitation of DECT is the small number of clinical studies. DECT can find ESWL-unsuitable stones, such as COM stones as well as uric acid stones, which improves its clinical usefulness. Unfortunately, most studies of DECT have reported methods for detecting uric acid stones. Few studies have been conducted for COM stones.
It is very important to predict stone components in an imaging study before treating a patient. We found that DECT was better able to distinguish uric acid stones and those with COM, which have relatively high treatment failure rates among ESWL-resistant stones. DECT can be used to predict stone components before treatment and reduce ESWL treatment failure, resulting in lower cost and time for re-treatment and increasing patient satisfaction.
Some limitations of our study should be mentioned. A prospective study is useful for measuring HU values before treatment and to check the rates of stone removal after treatment but is limited to collecting stones and analyzing their components. Our retrospective study was useful for measuring the corresponding HU values of the calculus components but was limited for predicting ESWL results. All of our patients were treated surgically. ESWL is a relatively noninvasive procedure that is usually applied to treat radiopaque urinary stones. However, we do not conduct post-ESWL stone component analyses in our hospital. Some kind of prospective study and a study to define effective cutoff values that have a higher diagnostic rate for each energy level will be needed.
CONCLUSIONS
DECT was effective for predicting urinary stone components before treatment. In particular, it was more useful than single-energy CT for predicting uric acid stones and COM stones, which are often resistant to ESWL. Additional studies will be needed to address the limitations of this study.
Footnotes
CONFLICTS OF INTEREST: The authors have nothing to disclose.
References
- 1.Sourtzis S, Thibeau JF, Damry N, Raslan A, Vandendris M, Bellemans M. Radiologic investigation of renal colic: unenhanced helical CT compared with excretory urography. AJR Am J Roentgenol. 1999;172:1491–1494. doi: 10.2214/ajr.172.6.10350278. [DOI] [PubMed] [Google Scholar]
- 2.Miller OF, Rineer SK, Reichard SR, Buckley RG, Donovan MS, Graham IR, et al. Prospective comparison of unenhanced spiral computed tomography and intravenous urogram in the evaluation of acute flank pain. Urology. 1998;52:982–987. doi: 10.1016/s0090-4295(98)00368-9. [DOI] [PubMed] [Google Scholar]
- 3.Yilmaz S, Sindel T, Arslan G, Ozkaynak C, Karaali K, Kabaalioglu A, et al. Renal colic: comparison of spiral CT, US and IVU in the detection of ureteral calculi. Eur Radiol. 1998;8:212–217. doi: 10.1007/s003300050364. [DOI] [PubMed] [Google Scholar]
- 4.Niall O, Russell J, MacGregor R, Duncan H, Mullins J. A comparison of noncontrast computerized tomography with excretory urography in the assessment of acute flank pain. J Urol. 1999;161:534–537. [PubMed] [Google Scholar]
- 5.Wang JH, Shen SH, Huang SS, Chang CY. Prospective comparison of unenhanced spiral computed tomography and intravenous urography in the evaluation of acute renal colic. J Chin Med Assoc. 2008;71:30–36. doi: 10.1016/S1726-4901(08)70069-8. [DOI] [PubMed] [Google Scholar]
- 6.Wen CC, Nakada SY. Treatment selection and outcomes: renal calculi. Urol Clin North Am. 2007;34:409–419. doi: 10.1016/j.ucl.2007.04.005. [DOI] [PubMed] [Google Scholar]
- 7.Miller NL, Lingeman JE. Management of kidney stones. BMJ. 2007;334:468–472. doi: 10.1136/bmj.39113.480185.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Galvin DJ, Pearle MS. The contemporary management of renal and ureteric calculi. BJU Int. 2006;98:1283–1288. doi: 10.1111/j.1464-410X.2006.06514.x. [DOI] [PubMed] [Google Scholar]
- 9.Dussol B. Uric acid nephrolithiasis. Rev Prat. 2011;61:389–392. [PubMed] [Google Scholar]
- 10.Gonzalez Enguita C, Rodriguez Minon-Cifuentes JL, Cabrera Perez J, Garcia de la Pena E, Calahorra Fernandez FJ, Garcia Cardoso J, et al. ESWL-resistant lithiasis. Actas Urol Esp. 1999;23:247–255. [PubMed] [Google Scholar]
- 11.Karcaaltıncaba M, Aktas A. Dual-energy CT revisited with multidetector CT: review of principles and clinical applications. Diagn Interv Radiol. 2011;17:181–194. doi: 10.4261/1305-3825.DIR.3860-10.0. [DOI] [PubMed] [Google Scholar]
- 12.Primak AN, Vrtiska TJ, Qu M, McCollough CH. Abdominal imaging: kidney stone differentiation. In: Johnson TR, Fink C, Schonberg SO, Reiser MF, editors. Dual energy CT in clinical practice. Heidelberg: Springer; 2010. pp. 177–192. [Google Scholar]
- 13.Ouzaid I, Al-qahtani S, Dominique S, Hupertan V, Fernandez P, Hermieu JF, et al. A 970 Hounsfield units (HU) threshold of kidney stone density on non-contrast computed tomography (NCCT) improves patients' selection for extracorporeal shockwave lithotripsy (ESWL): evidence from a prospective study. BJU Int. 2012;110(11 Pt B):E438–E442. doi: 10.1111/j.1464-410X.2012.10964.x. [DOI] [PubMed] [Google Scholar]
- 14.Nakasato T, Morita J, Ogawa Y. Evaluation of Hounsfield units as a predictive factor for the outcome of extracorporeal shock wave lithotripsy and stone composition. Urolithiasis. 2015;43:69–75. doi: 10.1007/s00240-014-0712-x. [DOI] [PubMed] [Google Scholar]
- 15.Sun XZ, Zhang ZW. Shock wave lithotripsy for uric acid stones. Asian J Surg. 2006;29:36–39. doi: 10.1016/S1015-9584(09)60292-X. [DOI] [PubMed] [Google Scholar]
- 16.Tomescu P, Panuş A, Mitroi G, Dragoescu O, Stoica L, Dena S, et al. Assessment of Extracorporeal Shock Wave Lithotripsy (ESWL) Therapeutic Efficiency in Urolithiasis. Curr Health Sci J. 2009;35:40–43. [PMC free article] [PubMed] [Google Scholar]
- 17.Ferrandino MN, Pierre SA, Simmons WN, Paulson EK, Albala DM, Preminger GM. Dual-energy computed tomography with advanced postimage acquisition data processing: improved determination of urinary stone composition. J Endourol. 2010;24:347–354. doi: 10.1089/end.2009.0193. [DOI] [PubMed] [Google Scholar]
- 18.Stolzmann P, Scheffel H, Rentsch K, Schertler T, Frauenfelder T, Leschka S, et al. Dual-energy computed tomography for the differentiation of uric acid stones: ex vivo performance evaluation. Urol Res. 2008;36:133–138. doi: 10.1007/s00240-008-0140-x. [DOI] [PubMed] [Google Scholar]
- 19.Graser A, Johnson TR, Bader M, Staehler M, Haseke N, Nikolaou K, et al. Dual energy CT characterization of urinary calculi: initial in vitro and clinical experience. Invest Radiol. 2008;43:112–119. doi: 10.1097/RLI.0b013e318157a144. [DOI] [PubMed] [Google Scholar]
- 20.Primak AN, Fletcher JG, Vrtiska TJ, Dzyubak OP, Lieske JC, Jackson ME, et al. Noninvasive differentiation of uric acid versus non-uric acid kidney stones using dual-energy CT. Acad Radiol. 2007;14:1441–1447. doi: 10.1016/j.acra.2007.09.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Eliahou R, Hidas G, Duvdevani M, Sosna J. Determination of renal stone composition with dual-energy computed tomography: an emerging application. Semin Ultrasound CT MR. 2010;31:315–320. doi: 10.1053/j.sult.2010.05.002. [DOI] [PubMed] [Google Scholar]
- 22.Thomas C, Krauss B, Ketelsen D, Tsiflikas I, Reimann A, Werner M, et al. Differentiation of urinary calculi with dual energy CT: effect of spectral shaping by high energy tin filtration. Invest Radiol. 2010;45:393–398. doi: 10.1097/RLI.0b013e3181df9d28. [DOI] [PubMed] [Google Scholar]
- 23.Matlaga BR, Kawamoto S, Fishman E. Dual source computed tomography: a novel technique to determine stone composition. Urology. 2008;72:1164–1168. doi: 10.1016/j.urology.2008.03.051. [DOI] [PubMed] [Google Scholar]
- 24.Wisenbaugh ES, Paden RG, Silva AC, Humphreys MR. Dual-energy vs conventional computed tomography in determining stone composition. Urology. 2014;83:1243–1247. doi: 10.1016/j.urology.2013.12.023. [DOI] [PubMed] [Google Scholar]
- 25.Stolzmann P, Frauenfelder T, Pfammatter T, Peter N, Scheffel H, Lachat M, et al. Endoleaks after endovascular abdominal aortic aneurysm repair: detection with dual-energy dual-source CT. Radiology. 2008;249:682–691. doi: 10.1148/radiol.2483080193. [DOI] [PubMed] [Google Scholar]
- 26.Thomas C, Patschan O, Ketelsen D, Tsiflikas I, Reimann A, Brodoefel H, et al. Dual-energy CT for the characterization of urinary calculi: In vitro and in vivo evaluation of a low-dose scanning protocol. Eur Radiol. 2009;19:1553–1559. doi: 10.1007/s00330-009-1300-2. [DOI] [PubMed] [Google Scholar]
- 27.Stolzmann P, Leschka S, Scheffel H, Rentsch K, Baumuller S, Desbiolles L, et al. Characterization of urinary stones with dual-energy CT: improved differentiation using a tin filter. Invest Radiol. 2010;45:1–6. doi: 10.1097/RLI.0b013e3181b9dbed. [DOI] [PubMed] [Google Scholar]
- 28.Jepperson MA, Cernigliaro JG, Ibrahim el-SH, Morin RL, Haley WE, Thiel DD. In vivo comparison of radiation exposure of dual-energy CT versus low-dose CT versus standard CT for imaging urinary calculi. J Endourol. 2015;29:141–146. doi: 10.1089/end.2014.0026. [DOI] [PMC free article] [PubMed] [Google Scholar]