

Abstract
Background:
Hand-sewn gastrointestinal anastomoses has been the traditional approach to gastrointestinal anastomosis in Nigeria while stapled anastomoses are infrequently performed in few centers.
Objectives:
To describe the outcome of our initial experience with stapled gastrointestinal anastomoses in a semi-urban patient population.
Patients and Methods:
Consecutive patients who had stapled gastrointestinal anastomoses between January 2011 and June 2014 in a Nigerian tertiary hospital were prospectively evaluated. Indications for operation, procedures performed and anastomoses constructed and postoperative outcome of each patient were documented.
Results:
Nineteen patients including seven males and 12 females had stapled anastomoses within the period. Their ages ranged between 41 and 68 (mean 52.5) years. Six (31.6%) Roux-en-Y gastrojejunostomies, 6 (31.6%) ileo-colic, 3 (15.8%) ileo-ileal, 2 (10.5%) colo-colic, and 2 (10.5%) colo-anal anastomoses were performed. Indications include antral gastric cancer in 4 (21.1%), right colon cancer 4 (21.1%), ileal perforations in 3 (15.8%) while 2 (10.5%) each had left colon cancer, common bile duct obstruction, rectal cancer and ruptured appendix. Mean duration of operation was 108 ± 46 min and mean duration of postoperative stay was 5 ± 2.6 days. No intraoperative complications were recorded and no anastomotic leakage occurred. At a median follow-up of 5 months no staple related stricture had occurred.
Conclusions:
Stapled gastrointestinal anastomoses are associated with a good outcome in our center. We propose a prospective, large-population randomized comparison of the technique with hand-sewn anastomoses.
KEYWORDS: Anastomoses, gastrointestinal, Nigeria, stapled
INTRODUCTION
Gastrointestinal anastomoses are commonly performed in general surgical practice. The conventional hand-sowing technique was practiced for several years until the introduction of mechanical stapling devices. After several years of modifications to the procedures and the devices, mechanical stapling is now an established alternative to the conventional hand-sowing technique. Several randomized controlled trials have compared with stapled and hand-sewn anastomoses in terms of technique and surgical outcomes.[1,2,3,4,5] A systematic review of randomized clinical trials concluded that stapled functional end to end anastomosis is associated with fewer leaks than hand-sewn anastomosis,[6] but a recent review of similar trials in colorectal anastomosis found insufficient evidence of any superiority of one technique over the other.[7]
Mechanical gastrointestinal stapling is not routinely deployed in many Nigerian hospitals for many reasons. In our institution for instance, nonavailability of the device as well as the prohibitive cost when it first became available in the country limited its application in general surgical practice. Until recently, local training on the technique was also not widely available with attendant limitation in the local expertise required to perform the technique. This situation improved recently with the training and retraining of our general surgeons on mechanical stapling and the receipt of a consignment of donated GI staplers with which an initial set of procedures were performed.
This study describes the outcome of initial experience with mechanical gastrointestinal stapling in a general surgery unit of a tertiary hospital in Nigeria.
PATIENTS AND METHODS
Consecutive patients who had stapled gastrointestinal anastomoses between January 2011 and June 2014 in one of two general surgery units of the Ife Hospital Unit of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria, were prospectively evaluated. Throughout the study, all patients requiring gastric and or intestinal anastomoses were offered options of hand-sewn and stapled techniques and those who could afford to procure staplers were recruited into this study. A cohort of six patients in 2013 who benefitted from the procedures at no personal costs using a consignment of donated staplers was also included.
All procedures were carried out by consultant general surgeons who had been trained on the use of gastrointestinal staplers. Stapling techniques were performed using the linear staplers, transverse linear cutters and circular staplers of Ethicon Endo-Surgery (Ethicon, Johnson and Johnson Limited). We documented the indications for operation, procedures performed and anastomoses constructed. The duration of operation and anastomosis related intraoperative complications were noted. Postoperatively, patients were clinically evaluated for anastomotic bleeding and obstruction. Time to commencement of oral intake and total duration of postoperative hospital stay were recorded. Features of anastomotic strictures were sought for on follow-up clinic visits.
RESULTS
Nineteen patients including seven males and 12 females had stapled gastrointestinal anastomoses within the period. Their ages ranged between 41 and 68 with a mean of 52.5 years. Indications for operations include antral gastric cancer in 4 (21.1%), right colon cancer in 4 (21.1%), ileal perforations in 3 (15.8%) while 2 (10.5%) each had left colon cancer, common bile duct obstruction, rectal cancer, and ruptured appendix with paracaecal abscesses. Six (31.6%) stapled ileo-colic anastomoses were constructed, with 6 (31.6%) Roux-en-Y gastro-jejunostomies, 3 (15.8%) ileo-ileal, 2 (10.5%) colo-colic, and 2 (10.5%) colo-anal anastomoses were performed as depicted in Table 1. Duration of operation ranged between 55 and 132 min with a mean duration of 108 ± 22 min while duration of postoperative stay ranged between 4 and 11 days with a mean 5 ± 2.6 days.
Table 1.
Procedures performed
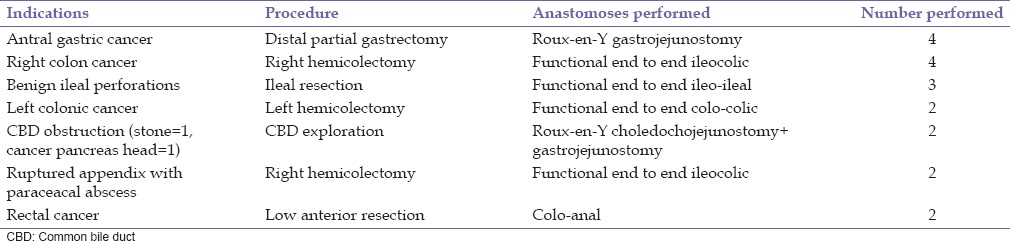
No intraoperative complications related to mechanical stapling occurred. Postoperatively, no anastomotic leakage occurred. Duration of follow-up ranged from 3 to 19 months. Two patients with advanced antral gastric malignancies developed malignant bowel obstructions while on chemotherapy 4 and 6 months respectively after surgery. Both of them succumbed to the disease progression. No staple related stricture occurred in any patient.
DISCUSSION
Within the period of this study, mechanical gastrointestinal stapling devices became more readily available in South-West Nigeria. This is partly because of the efforts of the marketers as well as the increasing interests of general surgeons in mechanical stapling. The high cost of the devices and the fact that healthcare financing is still largely sourced out-of-pocket by individuals in the country has limited its wide adoption in our practice. An additional N80,000-150,000 (approximately 400–800 US dollars) to the regular cost of laparotomy is required for mechanical stapling procedures and this may be unaffordable to a number of patients particularly in our hospital's semi-urban location.
Mechanical stapling has been established for the construction of various types of gastrointestinal anastomoses.[1,3,8,9,10] In this initial series, we have deployed mechanical stapling for a wide range of indications including benign and malignant conditions requiring various types of anastomoses. We have equally utilized the technique for both elective and emergency procedures. Gastro-jejunostomies and functional end-to-end ileo-colic anastomoses are however the most common procedures in our series with both accounting for about two-thirds of all procedures performed.
The outcome of the procedures we performed is generally comparable to that of hand-sewn technique in our center. Mechanical stapling is generally associated with a reduction in the duration of operation in many series.[11,12] We have not specifically timed the construction of anastomoses in this initial series but we have observed the entire duration of operation to be generally similar to that of hand-sewn procedures in our center. Mechanical stapling is also known to be associated with a reduction in the incidence of clinically significant anastomotic leakage particularly in ileo-transverse anastomoses.[6] In this series, no clinically detected anastomotic leakage was recorded and no anastomosis related peri-operative deaths were recorded. We recorded no anastomotic stricture at a mean follow-up duration of 1-year.
We are currently recruiting patients into a prospective randomized controlled study comparing hand-sewn and stapled technique for gastrointestinal anastomoses. We have also embarked on training of our surgical residents on the use of gastrointestinal staplers with the aim of improving their expertise and popularizing the technique among them. We are equally hopeful that wider coverage of the National Health Insurance Scheme in Nigeria and improvement of its scope will make routine deployment of stapled gastrointestinal anastomoses feasible among our patients.
CONCLUSIONS
Stapled gastrointestinal anastomoses are associated with a good outcome in our center even in the early stages of our experience. We propose a prospective, large-population randomized comparison of the technique with hand-sewn anastomoses.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
A consignment of gastrointestinal staplers among other items freely donated by MedWish Inc., Cleveland, Ohio, USA was used for a cohort of six patients in this study.
REFERENCES
- 1.Chandramohan SM, Gajbhiye RN, Agwarwal A, Creedon E, Schwiers ML, Waggoner JR, et al. A randomized study comparing outcomes of stapled and hand-sutured anastomoses in patients undergoing gastrointestinal surgery. Indian J Surg. 2013;75:311–6. doi: 10.1007/s12262-012-0496-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hasegawa H, Radley S, Morton DG, Keighley MR. Stapled versus sutured closure of loop ileostomy: A randomized controlled trial. Ann Surg. 2000;231:202–4. doi: 10.1097/00000658-200002000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Markar SR, Karthikesalingam A, Vyas S, Hashemi M, Winslet M. Hand-sewn versus stapled oesophago-gastric anastomosis: Systematic review and meta-analysis. J Gastrointest Surg. 2011;15:876–84. doi: 10.1007/s11605-011-1426-9. [DOI] [PubMed] [Google Scholar]
- 4.Leung TT, MacLean AR, Buie WD, Dixon E. Comparison of stapled versus handsewn loop ileostomy closure: A meta-analysis. J Gastrointest Surg. 2008;12:939–44. doi: 10.1007/s11605-007-0435-1. [DOI] [PubMed] [Google Scholar]
- 5.Kim T, Yu W, Chung H. Handsewn versus stapled gastroduodenostomy in patients with gastric cancer: Long-term follow-up of a randomized clinical trial. World J Surg. 2011;35:1026–9. doi: 10.1007/s00268-011-1038-2. [DOI] [PubMed] [Google Scholar]
- 6.Choy PY, Bissett IP, Docherty JG, Parry BR, Merrie A, Fitzgerald A. Stapled versus handsewn methods for ileocolic anastomoses. Cochrane Cochrane Database Syst Rev. 2011;3:CD004320. doi: 10.1002/14651858.CD004320.pub3. DOI: 10.1002/14651858. [DOI] [PubMed] [Google Scholar]
- 7.Neutzling CB, Lustosa SA, Proenca IM, da Silva EM, Matos D. Stapled versus handsewn methods for colorectal anastomosis surgery. Cochrane Database Syst Rev. 2012;2:CD003144. doi: 10.1002/14651858.CD003144.pub2. [DOI] [PubMed] [Google Scholar]
- 8.Kim RH, Takabe K. Methods of esophagogastric anastomoses following esophagectomy for cancer: A systematic review. J Surg Oncol. 2010;101:527–33. doi: 10.1002/jso.21510. [DOI] [PubMed] [Google Scholar]
- 9.Demetriades D, Murray JA, Chan LS, Ordoñez C, Bowley D, Nagy KK, et al. Handsewn versus stapled anastomosis in penetrating colon injuries requiring resection: A multicenter study. J Trauma. 2002;52:117–21. doi: 10.1097/00005373-200201000-00020. [DOI] [PubMed] [Google Scholar]
- 10.Resegotti A, Astegiano M, Farina EC, Ciccone G, Avagnina G, Giustetto A, et al. Side-to-side stapled anastomosis strongly reduces anastomotic leak rates in Crohn's disease surgery. Dis Colon Rectum. 2005;48:464–8. doi: 10.1007/s10350-004-0786-6. [DOI] [PubMed] [Google Scholar]
- 11.Farrah JP, Lauer CW, Bray MS, McCartt JM, Chang MC, Meredith JW, et al. Stapled versus hand-sewn anastomoses in emergency general surgery: A retrospective review of outcomes in a unique patient population. J Trauma Acute Care Surg. 2013;74:1187–92. doi: 10.1097/TA.0b013e31828cc9c4. [DOI] [PubMed] [Google Scholar]
- 12.Liu BW, Liu Y, Liu JR, Feng ZX. Comparison of hand-sewn and stapled anastomoses in surgeries of gastrointestinal tumors based on clinical practice of China. World J Surg Oncol. 2014;12:292. doi: 10.1186/1477-7819-12-292. [DOI] [PMC free article] [PubMed] [Google Scholar]