

Abstract
Introduction:
The prevalence of childhood obesity has increased over the last two decades. Obesity is a major risk factor for chronic diseases and plays a central role in insulin resistance or metabolic syndrome.
Methods:
The aim of the study was to assess the prevalence of obesity and abdominal obesity by means of body mass index (BMI) and waist-to-height ratio (WHtR) in adolescent girls in a district school in Bangladesh. Based on age and sex specific BMI percentiles, the students were classified as normal weight (5th–<85th percentile), overweight (85th–<95th percentiles), and obese (≥95th percentile). Central obesity was categorized as WHtR ≥ 0.5. Adolescent girls (aged 9–17 years) attending the sixth to twelfth grades (n = 501) in a Bengali medium school participated in the study.
Results:
The prevalence of obesity and overweight were 23% and 14% among the girls. The prevalence of central obesity was 26%. Around 14% of girls in the normal weight group were centrally obese. There was a significant relationship between WHtR and BMI status (P = 0.0001).
Conclusion:
Our study provides evidence showing a high prevalence of overall and central obesity in adolescent girls in our population. We emphasize the need for further large scale surveillance programs and preventive strategies in our population to reduce the incidence of obesity.
Keywords: Adolescent girls, central obesity, obesity, waist-height ratio
INTRODUCTION
The prevalence of childhood obesity has increased over the last two decades.[1] Obesity is a major risk factor for chronic diseases and plays a central role in insulin resistance or metabolic syndrome. In a recent study done in India, there was evidence of the presence of early cardiovascular risk factors in obese children and adolescents.[2] Body mass index (BMI) is widely used as a measure to evaluate the impact of obesity on cardiovascular and metabolic risk factors, both in children and adults. However, BMI does not always relate to central obesity[3] and it cannot differentiate muscle mass from bone and fat mass.[4] waist-to-height ratio (WHtR) has been proposed as an easily measurable anthropometric index for detection of central obesity and to assess associations between cardiometabolic risk factor variables and central intra-abdominal obesity.5,[6,7,8,9] The use of WHtR for detecting central obesity and its associated health risks was first proposed in the mid1990s.[10,11,12,13] Recently, many authors[14,15,16,17,18] have suggested the WHtR as a measure of excess central adiposity. The rationale underlying this index is that, for a given height, there is an acceptable degree of fat stored on the upper body. Since the WHtR takes into account children's height, a single cut-off point can likely be set for the ratio without age and gender difference bias.[18] In addition, it has been shown to be a simple, noninvasive, and practical tool that correlates well with visceral fat and is easier to use.[15,16,17,18] In the small number of studies that have examined this index in children, WHtR has been shown to be superior in its ability to predict cardiovascular disease risk factors compared with either BMI or percentage of body fat.[17] A WHtR cut-off-point of 0.5 has been proposed as a simple means of indicating whether the amount of central adiposity is excessive and represents a health risk in children.[14,15,16,17,18,19] In Bangladesh, studies have been done mostly in English medium schools focusing on overall obesity but no study has been done to assess central obesity in children and adolescents. In a recent study done among urban children, approximately a fivefold increase in overweight and obesity over the past two decades was reported.[20] In one study done in an adult population, the mean WHtR of 0.48 significantly correlated with sociodemographic variables and was markedly higher in females.[21]
Considering the scarcity of studies on WHtR in children and adolescents in our country the present study was done to assess the prevalence of obesity and central obesity by means of BMI and WHtR in a girls’ high school in a central district near the capital city of Bangladesh.
METHODS
Sample
All adolescent girls (aged 9–17 years) attending the sixth to 12 grades (n = 501) in a Bengali medium school participated in the study. This study was carried out as part of “Diabetes Awareness and screening program” a surveillance of changing diabetes in children (CDiC) program in Bangladesh Institute of Research and Rehabilitation of Diabetes, Endocrine and Metabolic Disorders, a tertiary hospital in Bangladesh. The survey was conducted with the cooperation of School teachers, CDiC staff, and some volunteers. They underwent 8 h of training before starting the survey. Students and their parents were informed about the study by means of written form. Informed written consent was obtained by means of a signed letter from the school authority. A self-designed structured questionnaire was used for the data collection.
Anthropometric measurements assessment
All the girls were examined by a trained team consisting of diabetes educators, dietician, and volunteers. The team had received 8 h of training and had been standardized in the measurement assessments. The assessment was carried out during school hours as time allocated by the school authority. Body weight was measured by a bathroom scale wearing light clothes to the nearest 100 g. Standing height was measured with stadiometer and measurement was done to the nearest 0.1 cm. Waist circumference (WC) measured to the nearest 0.5 cm in duplicate according to standard conditions by placing a flexible tape midway between the lowest rib and the iliac crest. The tape did not squeeze or compress the skin and was parallel to the floor. The measurement was taken on unclothed, relaxed subjects after gentle expiration. BMI was calculated as the ratio between weight (in kilograms) and the square of height (in meters). WHtR was calculated as the ratio between waist and height both measured in centimeters.
Cut-off values
Based on age and sex specific BMI percentiles,[22] the girls were classified as normal weight (5th–<85th percentiles), overweight (85th–<95 h percentiles), and obese (≥95th percentile). A cut-off of 0.5 was used to differentiate low WHtR from high W/HtR.[14,15,19,23]
Data analysis
Data were processed using the Statistical Package for the Social Sciences (SPSS) (SPSS Inc, Chicago, IL, USA). Descriptive statistics was presented as mean ± standard deviation score for normally distributed data and median with interquartile range (IQR) for skewed data. Chi-Square test was used to evaluate the relationship between WHtR and age group with BMI.
RESULTS
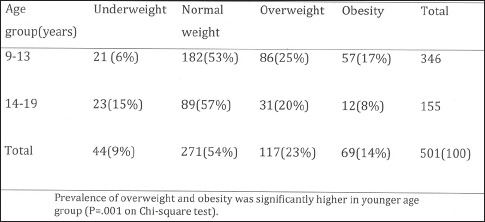
Median age of the students was 13.0 (IQR: 11.0–14.0). Median BMI was 20.3 (17.8–23.4) and median WHtR was 0.44 (0.38–0.50). The prevalence of overweight and obesity were 23% and 14% among the girls. The prevalence of central obesity was 26%. Around 14% of girls in the normal weight group were centrally obese. In overweight girls, 46% and in the obese group, 54% had central obesity [Figure 1]. There was significant relationship between WHtR and BMI status (P = 0.00001) [Figure 1]. We have analyzed age groups with BMI status, which showed a significantly higher rate of obesity and overweight in the younger age group (P = 0.001) [Table 1]. There was no significant relation between the two age groups (26% vs. 24%) with WHtR (P = 0.673).
Figure 1.
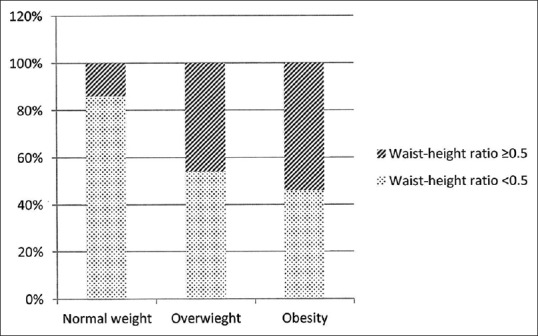
Waist-height ratio among different body mass index group (P = 0.0001)
Table 1.
BMI according to age group
DISCUSSION
The prevalence of obesity was 14% and was higher in younger age than older age group (16% vs. 8%). In our previous study done between 3 and 18 years of age, 15.3% were females which is similar to this finding.[24] The prevalence of overweight was 23% and was higher in younger age group (25% vs. 20%) in our study. In a study done in India among girls aged 13–18 years, the prevalence of overweight was 15.8%.[25] In Tunisian adolescent girls, it was found to be 16%.[26] The prevalence of overweight in our studied subjects was higher than the studies (23%) mentioned above.
In our population, the prevalence of abdominal obesity was 26%.
The prevalence of abdominal obesity was found to be 16.7% in 1500 Egyptian males and females aged 11–19 years according to WHtR.[1] McCarfhy and Ashwell reported WHtR exceeded 0.50 in 11.7% of adolescent girls aged 11–16 years in UK children in 1997.[15] In a Swedish study girls aged 15.6 ± 0.4 years, high-risk WC was detected in 30.1% of subjects.[27] In a large cohort of 985 girls (14–17 years old) in Iran, 18.2% were centrally obese.[28] Children from different populations vary in their rate of proportional growth and in fat patterning.[29,30] Body fat distribution in total mass and composition of skeletal muscles, subcutaneous, intra-abdominal adipose tissue, and bone varies with ethnicity. In Asian populations, particularly those who suffered childhood malnutrition have less skeletal muscle mass and pelvic skeleton dimensions, which may affect waist and hip circumferences.[31] Several epidemiologic studies in Asian population including Chinese, Taiwanese, Indians, and Koreans have higher amounts of body fat at lower BMIs and WC than do Western populations such as USA whites and blacks, perhaps leading to the greater prevalence of cardiovascular disease risk factors at lower BMIs in Asian populations than in Western populations.[32]
In our sample, 54% of obese, 46% of overweight, and 14% of normal weight subjects had central obesity. A high prevalence of central adiposity in our population is of concern as it increases the risk for obesity-associated morbidity and mortality in children and adults.[33]
CONCLUSION
Our study provides evidence showing a high prevalence of overall and central obesity in adolescent girls in our community. We emphasize the need for large scale surveillance programs and preventive strategies in our population to reduce the incidence of obesity.
ACKNOWLEDGMENT
We are grateful to all the students and teachers of the school for their continuous support and cooperation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Abolfotouh MA, Sallam SA, Mohammed MS, Loutfy AA, Hasab AA. Prevalence of elevated blood pressure and association with obesity in egyptian school adolescents. Int J Hypertens 2011. 2011 doi: 10.4061/2011/952537. 952537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Namburi RP, Ponnala AR, Karthik TS, Rani PR, Maheshwari R. A study on metabolic variables and its association with high sensitive C-reactive protein in obese children and adolescents. Indian J Endocrinol Metab. 2013;17(Suppl 1):S360–2. doi: 10.4103/2230-8210.119623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Neovius M, Rasmussen F. Evaluation of BMI-based classification of adolescent overweight and obesity: Choice of percentage body fat cutoffs exerts a large influence. The COMPASS study. Eur J Clin Nutr. 2008;62:1201–7. doi: 10.1038/sj.ejcn.1602846. [DOI] [PubMed] [Google Scholar]
- 4.Hall DM, Cole TJ. What use is the BMI? Arch Dis Child. 2006;91:283–6. doi: 10.1136/adc.2005.077339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nambiar S, Hughes I, Davies PS. Developing waist-to-height ratio cut-offs to define overweight and obesity in children and adolescents. Public Health Nutr. 2010;13:1566–74. doi: 10.1017/S1368980009993053. [DOI] [PubMed] [Google Scholar]
- 6.Higgins M, Kannel W, Garrison R, Pinsky J, Stokes J., 3rd Hazards of obesity – The Framingham experience. Acta Med Scand Suppl. 1988;723:23–36. doi: 10.1111/j.0954-6820.1987.tb05925.x. [DOI] [PubMed] [Google Scholar]
- 7.Hsieh SD, Muto T. The superiority of waist-to-height ratio as an anthropometric index to evaluate clustering of coronary risk factors among non-obese men and women. Prev Med. 2005;40:216–20. doi: 10.1016/j.ypmed.2004.05.025. [DOI] [PubMed] [Google Scholar]
- 8.Bosy-Westphal A, Geisler C, Onur S, Korth O, Selberg O, Schrezenmeir J , Value of body fat mass vs anthropometric obesity indices in the assessment of metabolic risk factors. Int J Obes (Lond) 2006;30:475–83. doi: 10.1038/sj.ijo.0803144. [DOI] [PubMed] [Google Scholar]
- 9.Srinivasan SR, Wang R, Chen W, Wei CY, Xu J, Berenson GS. Utility of waist-to-height ratio in detecting central obesity and related adverse cardiovascular risk profile among normal weight younger adults (from the Bogalusa Heart Study) Am J Cardiol. 2009;104:721–4. doi: 10.1016/j.amjcard.2009.04.037. [DOI] [PubMed] [Google Scholar]
- 10.Hsieh SD, Yoshinaga H. Abdominal fat distribution and coronary heart disease risk factors in men-waist/height ratio as a simple and useful predictor. Int J Obes Relat Metab Disord. 1995;19:585–9. [PubMed] [Google Scholar]
- 11.Hsieh SD, Yoshinaga H. Waist/height ratio as a simple and useful predictor of coronary heart disease risk factors in women. Intern Med. 1995;34:1147–52. doi: 10.2169/internalmedicine.34.1147. [DOI] [PubMed] [Google Scholar]
- 12.Lee JS, Aoki K, Kawakubo K, Gunji A. A study on indices of body fat distribution for screening for obesity. Sangyo Eiseigaku Zasshi. 1995;37:9–18. doi: 10.1539/sangyoeisei.37.9. [DOI] [PubMed] [Google Scholar]
- 13.Ashwell M, Lejeune S, McPherson K. Ratio of waist circumference to height may be better indicator of need for weight management. BMJ. 1996:312–377. doi: 10.1136/bmj.312.7027.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Maffeis C, Banzato C, Talamini G. Obesity Study Group of the Italian Society of Pediatric Endocrinology and Diabetology. Waist-to-height ratio, a useful index to identify high metabolic risk in overweight children. J Pediatr. 2008;152:207–13. doi: 10.1016/j.jpeds.2007.09.021. [DOI] [PubMed] [Google Scholar]
- 15.McCarthy HD, Ashwell M. A study of central fatness using waist-to-height ratios in UK children and adolescents over two decades supports the simple message – ‘Keep your waist circumference to less than half your height’. Int J Obes (Lond) 2006;30:988–92. doi: 10.1038/sj.ijo.0803226. [DOI] [PubMed] [Google Scholar]
- 16.Kahn HS, Imperatore G, Cheng YJ. A population-based comparison of BMI percentiles and waist-to-height ratio for identifying cardiovascular risk in youth. J Pediatr. 2005;146:482–8. doi: 10.1016/j.jpeds.2004.12.028. [DOI] [PubMed] [Google Scholar]
- 17.Savva SC, Tornaritis M, Savva ME, Kourides Y, Panagi A, Silikiotou N, et al. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. Int J Obes Relat Metab Disord. 2000;24:1453–8. doi: 10.1038/sj.ijo.0801401. [DOI] [PubMed] [Google Scholar]
- 18.Hara M, Saitou E, Iwata F, Okada T, Harada K. Waist-to-height ratio is the best predictor of cardiovascular disease risk factors in Japanese schoolchildren. J Atheroscler Thromb. 2002;9:127–32. doi: 10.5551/jat.9.127. [DOI] [PubMed] [Google Scholar]
- 19.Browning LM, Hsieh SD, Ashwell M. A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0·5 could be a suitable global boundary value. Nutr Res Rev. 2010;23:247–69. doi: 10.1017/S0954422410000144. [DOI] [PubMed] [Google Scholar]
- 20.Das SK, Chisti MJ, Huq S, Malek MA, Vanderlee L, Salam MA, et al. Changing trend of overweight and obesity and their associated factors in an urban population of Bangladesh. Food Nutr. 2013;4:678–89. [Google Scholar]
- 21.Flora MS, Taylor MC, Rahman M. Waist-to-height ratio and socio-demographic Characteristics of Bangladeshi adults. Ibrahim Med Coll J. 2010;4:49–58. [Google Scholar]
- 22.Kuczmarski RJ, Oglen CL, Grummer-Strawn LM. Advance Data 314. Washington, DC: Center for Disease Control and Prevention/National Center for Health Statistics; 2000. 2000 CDC Growth Charts; United States; pp. 1–28. [PubMed] [Google Scholar]
- 23.Ashwell M, Hsieh SD. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int J Food Sci Nutr. 2005;56:303–7. doi: 10.1080/09637480500195066. [DOI] [PubMed] [Google Scholar]
- 24.Mohsin F, Tayyeb S, Baki A, Sarker S, Zabeen B, Begum T, et al. Prevalence of obesity among affluent school children in Dhaka. Mymensingh Med J. 2010;19:549–54. [PubMed] [Google Scholar]
- 25.Ramachandran A, Snehalatha C, Vinitha R, Thayyil M, Kumar CK, Sheeba L, et al. Prevalence of overweight in urban Indian adolescent school children. Diabetes Res Clin Pract. 2002;57:185–90. doi: 10.1016/s0168-8227(02)00056-6. [DOI] [PubMed] [Google Scholar]
- 26.Ghannem H, Darioli R, Limam K, Harrabi I, Gaha R, Trabelsi L, et al. Epidemiology of cardiovascular risk factors among schoolchildren in Sousse, Tunisia. J Cardiovasc Risk. 2001;8:87–91. doi: 10.1177/174182670100800205. [DOI] [PubMed] [Google Scholar]
- 27.Ortega FB, Ruiz JR, Sjöström M. Physical activity, overweight and central adiposity in Swedish children and adolescents: The European Youth Heart Study. Int J Behav Nutr Phys Act. 2007:4–61. doi: 10.1186/1479-5868-4-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rafraf MA, Mohamadi EB, Gargari BP. Prevalence of overall and abdominal obesity among adolescent high school girls in Tabriz, Iran. Int Med J Malaysia. 2013;12:27–32. [Google Scholar]
- 29.McCarthy HD, Jarrett KV, Crawley HF. The development of waist circumference percentiles in British children aged 5.0-16.9 y. Eur J Clin Nutr. 2001;55:902–7. doi: 10.1038/sj.ejcn.1601240. [DOI] [PubMed] [Google Scholar]
- 30.Tybor DJ, Lichtenstein AH, Dallal GE, Daniels SR, Must A. Racial differences in central adiposity in a longitudinal cohort of black and white adolescent females. BMC Pediatr. 2010:10–2. doi: 10.1186/1471-2431-10-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Misra A, Vikram NK, Gupta R, Pandey RM, Wasir JS, Gupta VP. Waist circumference cutoff points and action levels for Asian Indians for identification of abdominal obesity. Int J Obes (Lond) 2006;30:106–11. doi: 10.1038/sj.ijo.0803111. [DOI] [PubMed] [Google Scholar]
- 32.Wildman RP, Gu D, Reynolds K, Duan X, He J. Appropriate body mass index and waist circumference cutoffs for categorization of overweight and central adiposity among Chinese adults. Am J Clin Nutr. 2004;80:1129–36. doi: 10.1093/ajcn/80.5.1129. [DOI] [PubMed] [Google Scholar]
- 33.Li C, Ford ES, Mokdad AH, Cook S. Recent trends in waist circumference and waist-height ratio among US children and adolescents. Pediatrics. 2006;118:e1390–8. doi: 10.1542/peds.2006-1062. [DOI] [PubMed] [Google Scholar]