

Abstract
De novo non-alcoholic fatty liver disease (NAFLD) is a common late complication for long-term survivors after liver transplantation. Genomic studies confirmed that PNPLA3 I148M and TM6SF2 E167K polymorphisms affected NAFLD susceptibility in the general population. However, this association was not validated in survivors after liver transplantation (LT). We performed a cross-sectional survey to investigate this relationship. A comprehensive survey, including anthropometric measurements, fasting venous blood sampling, ultrasound, and questionnaires was performed in the short-term. The clinical indications and patient’s steatosis status before LT were collected from inpatient medical records. Sixty-five long-term recipients with a survival exceeding 10 years were enrolled in the final analysis. De novo NAFLD was more frequent in PNPLA3 GG carriers (0.33 vs 0.10 for GG vs CC + CG carriers, P = 0.018), while the genetic impact on NAFLD susceptibility was insignificant when categorized by the TM6SF2 polymorphism (0.19 in CC vs 0.14 in CT + TT carriers, P = 0.883). Multi-covariate analysis revealed that PNPLA3 exerted a significant genetic effect on de novo NAFLD following a recessive model (GG vs CC + CG, OR = 14.2, 95%CI: 1.78-113, P = 0.012). Compared to recipients with only the PNPLA3 GG allele or obesity (defined as body mass index > 25 kg/m2), steatosis was highly prevalent (71.4%) in PNPLA3 GG carriers with obesity. In conclusion, PNPLA3 I148M, but not TM6SF2 E167K, affects de novo NAFLD occurrence with a prominent interaction with obesity. Weight control might be a meaningful method to reduce the genetic susceptibility to NAFLD exerted by PNPLA3 variants.
Keywords: PNPLA3, TM6SF2, Non-alcoholic fatty liver disease, Liver transplantation, Recipient
Core tip: Previous genomic studies identified PNPLA3 I148M and TM6SF2 E167K polymorphisms as the most prominent genetic variations associated with non-alcoholic fatty liver disease (NAFLD) susceptibility in general populations. However, these impacts have never been evaluated in long-term liver transplant recipients. In a collection of survivors 10 years after liver transplantation, we found that the PNPLA3 I148M, but not TM6SF2 E167K polymorphism, affected de novo NAFLD predisposition and interacted with obesity. Our results revealed that liver transplant recipients might benefit from weight control to limit the deleterious effect exerted by genetic factors.
TO THE EDITOR
De novo non-alcoholic fatty liver disease (NAFLD) is a common late complication for long-term survivors after liver transplantation (LT)[1]. De novo NAFLD affects allograft survival indirectly by increasing cardiovascular and infectious disease occurrence[2]. Previous genomic studies identified the PNPLA3 I148M and TM6SF2 E167K polymorphisms as the most likely single nucleotide polymorphisms to influence NAFLD susceptibility in the general population[3]. However, this relationship was not confirmed in long-term survivors after LT as a specific population. Therefore, we performed a cross-sectional survey to investigate the impact of genetic and environmental risk factors for de novo NAFLD in adult long-term survivors after receiving LT.
After obtaining written informed consent, a comprehensive survey, including anthropometric measurements (for body weight and height), fasting venous blood sampling (for liver function, lipid, glucose, viral biomarker testing, genotyping, etc.), ultrasound examination, and questionnaires (for alcohol intake, smoking, exercise, and immunosuppression) were performed over the short-term (December 13th-14th, 2014). Indications for LT and patients’ steatosis status before LT were collected from inpatient medical records. The study was approved by the Institutional Review Board of our hospital.
NAFLD and metabolic syndrome were defined according to previous criteria[4]. Participants with recurrent liver steatosis were excluded. Accordingly, 65 subjects (57 males and 8 females) receiving LT (from September, 1999 to November, 2004) in our hospital with a survival exceeding 10 years were enrolled into the final analysis.
All survivors were Han Chinese and negative for hepatitis B virus DNA/hepatitis C virus RNA assay. As shown in Table 1, twelve of the patients were diagnosed with de novo NAFLD. By univariate analysis, the NAFLD subgroup hada significantly higher body mass index (BMI), triglyceride (TG) levels, and fasting blood glucose (FBG) levels. De novo NAFLD was more frequent in PNPLA3 GG carriers than in CC + CG carriers (0.33 vs 0.10, P = 0.018), while the genetic impact on NAFLD susceptibility was insignificant when categorized by the TM6SF2 polymorphism (0.19 in CC vs 0.14 in CT + TT carriers, P = 0.883). Multi-covariate analysis revealed that PNPLA3 exerted a significant genetic effect on de novo NAFLD following a recessive model (GG vs CC + CG, OR = 14.2, 95%CI: 1.78-113, P = 0.012). Compared to recipients only carrying the PNPLA3 GG allele or being obese (defined as BMI > 25 kg/m2), the prevalence of steatosis was disproportionally higher (71.4%) in PNPLA3 GG carriers who were obese (Figure 1).
Table 1.
Current status of long-term recipients surviving more than 10 years
|
Univariate |
Multivariate |
||||
| NAFLD (n = 12) | Control (n = 53) | P value | OR | P value | |
| Age (yr) | 56.5 ± 8.4 | 53.6 ± 10.1 | 0.356 | 1.04 (0.92-1.18) | 0.528 |
| Gender (M/F) | 10/2 | 47/6 | 0.611 | 1.40 (0.14-14.2) | 0.427 |
| Indication for LT | |||||
| Hepatitis/cirrhosis/ cancer/others | 1/8/2/1 | 7/35/9/2 | 0.889 | ||
| Survival time (yr) | 11.2 ± 0.9 | 11.5 ± 1.4 | 0.541 | ||
| BMI (kg/m2) | 25.1 ± 3.0 | 22.5 ± 2.6 | 0.003 | 1.47 (1.03-2.08) | 0.032 |
| TG (mmol/L) | 1.6 ± 1.1 | 1.1 ± 0.6 | 0.038 | 1.34 (0.38-4.71) | 0.652 |
| HDL-C (mmol/L) | 1.2 (1.0-1.4) | 1.3 (1.0-1.7) | 0.267 | ||
| FBG (mmol/L) | 7.6 ± 3.4 | 5.7 ± 1.9 | 0.013 | 1.49 (0.93-2.37) | 0.095 |
| Hypertension (Yes/no) | 3/9 | 21/32 | 0.343 | ||
| SUA (μmol/L) | 381.6 ± 75.6 | 342.6 ± 76.4 | 0.116 | ||
| MetS (Yes/no) | 4/8 | 9/44 | 0.201 | ||
| ALT (U/L) | 36.7 ± 7.0 | 38.8 ± 6.7 | 0.882 | ||
| Alcohol intake (g/wk) | 11.6 ± 7.3 | 21.0 ± 8.2 | 0.766 | ||
| Smoking (cigar/d) | 4.2 ± 3.4 | 4.3 ± 1.2 | 0.969 | ||
| Exercise (min/d) | 18.5 ± 6.0 | 22.9 ± 2.9 | 0.513 | ||
| Immunosuppression | |||||
| Tacrolimus/ cyclosporine/ MMF/sirolimus/ none | 11/1/0/0/0 | 36/12/1/2/2 | 0.575 | ||
| PNPLA3 (CC/CG/GG) | 1/3/8 | 16/21/16 | 0.018 | 14.2 (1.78-113) | 0.012 |
| TM6SF2 (CC/CT/TT) | 11/1/0 | 47/5/1 | 0.883 | 2.68 (0.25-28.5) | 0.413 |
Continuous variables with equal variance are presented as the mean ± SD; Continuous variables with unequal variance are presented as the median (interquartile range); Categorical variables are presented as the number of subjects. One-way ANOVA was used for the comparison between continuous variables with equal variance, Mann-Whitney U test was used for the comparison between continuous variables with unequal variance, chi-square test was used for the comparison between categorical variables in univariate analysis, and logistic regression analysis was used in the multivariate analysis. The effect of the PNPLA3 I148M polymorphism was evaluated by a recessive genetic model (GG vs CG + CC); the effect of the TM6SF2 E167K polymorphism was evaluated by a dominant genetic model (CC + CT vs TT) for decreased prevalence of TT carrier. ALT: Alanine aminotransferase; BMI: Body mass index; F: Female; FBG: Fasting blood glucose; HBsAg: Hepatitis B surface antigen; HDL-C: High-density lipoprotein cholesterol; LT: Liver transplantation; M: Male; MetS: Metabolic syndrome; MMF: Mycophenolatemofetil; SUA: Serum uric acid; TG: Triglyceride.
Figure 1.
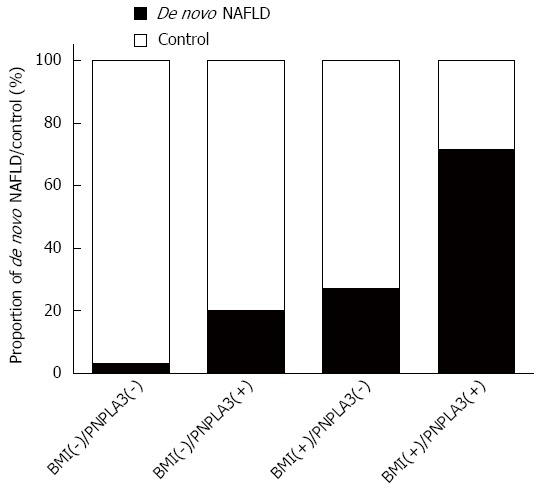
Proportion of the de novo non-alcoholic fatty liver disease/control categorized by the body mass index-PNPLA3 I148M polymorphism. BMI (+) represents BMI ≤ 25 kg/m2; BMI (-) represents BMI > 25 kg/m2; PNPLA3 (+) indicates PNPLA3 I148M GG carriers; PNPLA3 (-) indicates the PNPLA3 I148M CC + CG carriers. BMI: Body mass index; NAFLD: Non-alcoholic fatty liver disease.
This is the first report on the risk factors associated with de novo steatosis in Chinese long-term survivors after LT. PNPLA3, but TM6SF2, affects de novo NAFLD occurrence and has a prominent interaction with obesity. Weight control in recipients might be a potential method to reduce the genetic susceptibility of NAFLD exerted by the PNPLA3 variant.
Footnotes
Supported by National S and T Major Project, No. 2012ZX10002017; Foundation for Innovative Research Groups of the National Natural Science Foundation of China, Grant No. 81421062; and China Postdoctoral Science Foundation Project, No. 2015M570518.
Conflict-of-interest statement: Nothing to report.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: April 7, 2015
First decision: May 18, 2015
Article in press: July 8, 2015
P- Reviewer: Yu DY S- Editor: Ma YJ L- Editor: A E- Editor: Zhang DN
References
- 1.Hübscher SG. What is the long-term outcome of the liver allograft? J Hepatol. 2011;55:702–717. doi: 10.1016/j.jhep.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 2.Zezos P, Renner EL. Liver transplantation and non-alcoholic fatty liver disease. World J Gastroenterol. 2014;20:15532–15538. doi: 10.3748/wjg.v20.i42.15532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rinella ME, Sanyal AJ. NAFLD in 2014: Genetics, diagnostics and therapeutic advances in NAFLD. Nat Rev Gastroenterol Hepatol. 2015;12:65–66. doi: 10.1038/nrgastro.2014.232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rector RS, Thyfault JP, Wei Y, Ibdah JA. Non-alcoholic fatty liver disease and the metabolic syndrome: an update. World J Gastroenterol. 2008;14:185–192. doi: 10.3748/wjg.14.185. [DOI] [PMC free article] [PubMed] [Google Scholar]