

Abstract
The authors report the case of a 55-year-old female, hypertensive, smoker patient presenting with dysphonia, dysphagia and persistent dry cough. Laryngoscopy diagnosed left vocal cord paralysis. Computed tomography demonstrated saccular aneurysm of the inferior wall of the aortic arch, stretching the left recurrent laryngeal nerve, a finding compatible with Ortner’s syndrome.
Keywords: Ortner’s syndrome, Aortic arch aneurysm, Recurrent laryngeal nerve, Dysphonia, Dry cough
Abstract
Relatamos um caso de paciente do sexo feminino, 55 anos, hipertensa, tabagista, apresentando disfonia, disfagia e tosse seca persistente. À videolaringoscopia foi observada paralisia da prega vocal esquerda. A tomografia computadorizada mostrou aneurisma sacular da parede inferior do arco aórtico, no local de deflexão do nervo laríngeo recorrente, permitindo diagnosticar a síndrome de Ortner.
INTRODUCTION
In 1897, Ortner described the association between mitral stenosis and hoarseness related to paralysis of the left recurrent laryngeal nerve(1). Ortner’s syndrome, whose physiopathology is related to compromise of the recurrent laryngeal nerve between the aorta and the pulmonary artery, may be present in other diseases of benign cardiovascular origin(1).
In the present report, the authors describe the case of a patient presenting with symptoms compatible with the syndrome as a result of a saccular aneurysm located in the inferior wall of the aortic arch, determining an injury to the mentioned nerve.
CASE REPORT
A 55-year-old, female, hypertensive, smoker (35 pack year) patient presenting with dysphonia, mild dysphagia and persistent dry cough for four months. Videolaryngoscopy demonstrated paramedian left vocal cord paralysis (Figure 1).
Figure 1.
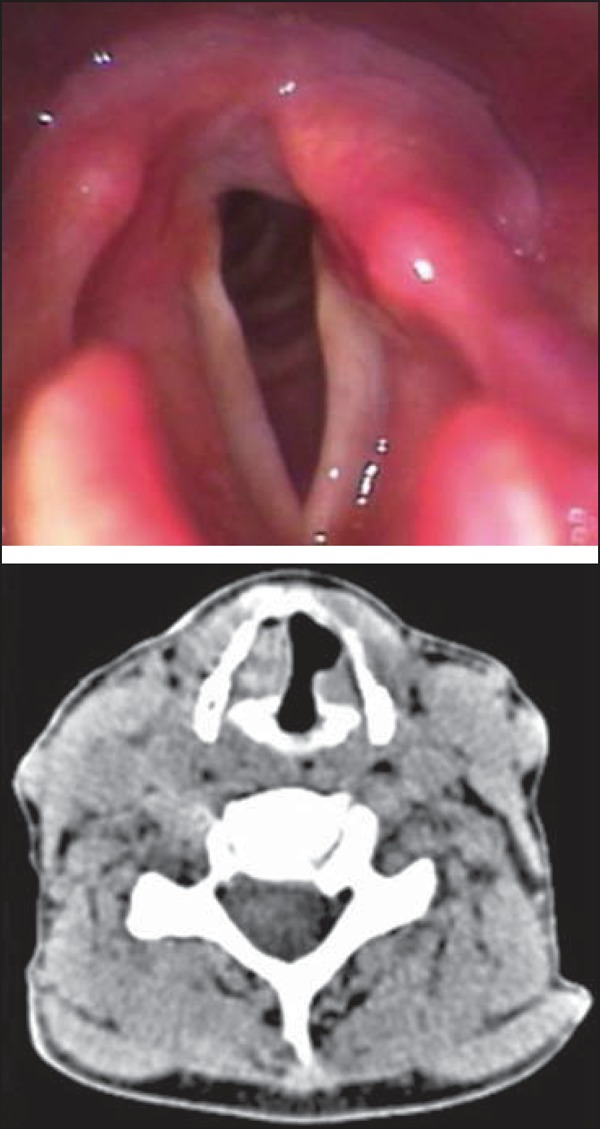
Documentation of videolaryngoscopy and axial CT section (soft tissue window) demonstrating vocal cords asymmetry, with signs of paralysis at left.
Computed tomography of cervical and thoracic regions confirmed the videolaryngoscopy findings (Figure 1) and defined the diagnosis by demonstrating the presence of a focal, saccular aneurysm on the inferior wall of the aortic arch (Figures 2, 3 and 4), responsible for stretching the left recurrent laryngeal nerve and causing the described symptoms.
Figure 2.

Sagittal oblique reconstruction with the maximum intensity projection technique identifying the aneurysm on the inferior wall of the aortic arch where the recurrent laryngeal nerve usually travels along this vessel.
Figure 3.
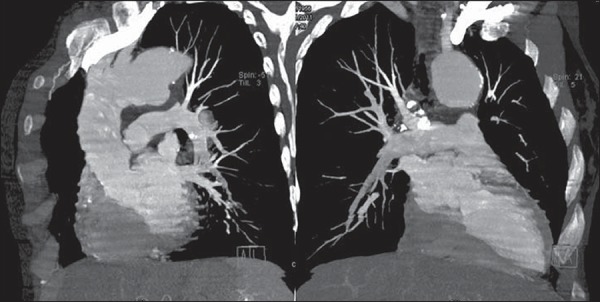
Maximum intensity projection, multiplanar reformation obtaining oblique images demonstrating the anatomical relationship between the aortic arch, pulmonary artery trunk and the aneurysm projected on the aortopulmonary window.
Figure 4.

Right and left, anteroposterior and oblique multiplanar reconstructions, utilizing the volume rendering technique, demonstrating focal dilatation of the inferior wall of the aortic arch (arrows).
DISCUSSION
Persistent cough, dysphagia and dysphonia may suggest vocal cord paralysis secondary to injury of the recurrent laryngeal nerve. The vocal cords receive motor innervation by a vagus nerve branch, the recurrent laryngeal nerve. At right, the recurrent laryngeal nerve travels along the inferior surface of the subclavian artery and, at left, it travels inferiorly to the aortic arch in the aortopulmonary window, upwards to the larynx, adjacent to the tracheoesophageal groove. The symptoms may be determined by any compression/stretching of the vagus nerve, at its origin in the lateral sulcus posterior to the bulb, on its course in the bulbocerebellar cistern, at the point where it emerges from the skull through the jugular foramen, in the carotid sheath or adjacent to the sites of recurrent laryngeal nerves deflection in the above mentioned vessels(2).
Ortner’s syndrome, also known as cardiovocal syndrome, results from compression of the recurrent laryngeal nerve secondary to benign cardiovascular causes (Table 1)(1-3). Other conditions may affect the mentioned nerve, however without causing the syndrome(2,4,5).
Table 1.
Differential diagnosis of medial causes of involvement of recurrent laryngeal nerve.
| Vascular/cardiac | Aortic dissection or pseudoaneurysm, left atrium enlargement, congenital heart diseases, pulmonary artery enlargement, pulmonary embolism |
| Neoplastic | Bronchogenic carcinoma, lymphoma, esophageal carcinoma, neurogenic tumors (paraganglioma, schwannoma), thyroid carcinoma, malignant thymus disease, lymph node metastasis; retrosternal goiter |
| Surgical/iatrogenic | Heart surgery, median sternotomy, patent ductus arteriosus ligation or embolization, left lobectomy/pneumomectomy, mediastinoscopy, radical esophagectomy, tracheal resection, thymectomy, thyroidectomy, anterior approach in spine surgeries, carotid endarterectomy, external radiotherapy |
| Inflammatory | Sarcoidosis, silicosis, fibrosing mediastinitis |
| Infiltrative | Amyloidosis |
| Infectious | Tuberculosis, histoplasmosis, coccidioidomycosis, bacterial abscess, mycotic aortic pseudoaneurysm |
| Traumatic | Deceleration injuries, penetrating chest injuries |
The tomographic findings of vocal cord paralysis include: thickening and medial positioning of the aryepiglottic fold; increased volume of the piriform sinus and ipsilateral ventricles; anteromedial positioning of the arytenoids cartilage; paramedian position of the vocal cord. In the coronal plane, one may observe subglottic arch flattening(2).
The diagnostic confirmation includes endoscopic studies of the larynx and skull, neck and chest computed tomography. The tomographic evaluation is aimed at demonstrating, besides the laryngeal abnormalities, the presence of possible lesions in the course of the vagus and recurrent laryngeal nerves, from the skull base to the aortopulmonary window(3,6,7), corroborating the diagnosis.
Footnotes
Study developed at Hospital Universitário – Universidade Federal de Juiz de Fora (HU-UFJF), Juiz de Fora, MG, Brazil.
Dutra BL, Campos LC, Marques HC, Vilela VM, Carvalho REDS, Duque AGS. Ortner’s syndrome: a case report and literature review. Radiol Bras. 2015 Jul/Ago;48(4):260–262.
REFERENCES
- 1.Sengupta A, Dubey SP, Chaudhuri D, et al. Ortner's syndrome revisited. J Laryngol Otol. 1998;112:377–379. doi: 10.1017/s0022215100140514. [DOI] [PubMed] [Google Scholar]
- 2.Paquette CM, Manos DC, Psooy BJ. Unilateral vocal cord paralysis: a review of CT findings, mediastinal causes, and the course of the recurrent laryngeal nerves. Radiographics. 2012;32:721–740. doi: 10.1148/rg.323115129. [DOI] [PubMed] [Google Scholar]
- 3.Bickle IC, Kelly BE, Brooker DS. Ortner's syndrome: a radiological diagnosis. Ulster Med J. 2002;71:55–56. [PMC free article] [PubMed] [Google Scholar]
- 4.Yumoto E, Minoda R, Hyodo M, et al. Causes of recurrent laryngeal nerve paralysis. Auris Nasus Larynx. 2002;29:41–45. doi: 10.1016/s0385-8146(01)00122-5. [DOI] [PubMed] [Google Scholar]
- 5.Hirose H. Clinical observations on 600 cases of recurrent laryngeal nerve paralysis. Auris Nasus Larynx. 1978;5:39–48. doi: 10.1016/s0385-8146(78)80005-4. [DOI] [PubMed] [Google Scholar]
- 6.Ishii K, Adachi H, Tsubaki K, et al. Evaluation of recurrent nerve paralysis due to thoracic aortic aneurysm and aneurysm repair. Laryngoscope. 2004;114:2176–2181. doi: 10.1097/01.mlg.0000149453.91005.ab. [DOI] [PubMed] [Google Scholar]
- 7.Chan P, Huang JJ, Yang YJ. Left vocal cord palsy: an unusual presentation of a mycotic aneurysm of the aorta caused by Salmonella cholerasuis. Scand J Infect Dis. 1994;26:219–221. doi: 10.3109/00365549409011787. [DOI] [PubMed] [Google Scholar]