

Abstract
Background:
Multiple sclerosis (MS) is a chronic inflammatory and demyelinating disease of the central nervous system, which is accompanied by significant disabilities. Although there are some published data regarding the epidemiological features of MS in other parts of Iran, scarce data are available about the prevalence and demographic characteristics of MS in Fars province. The current study aimed to address the prevalence and incidence rate of MS as well as the temporal trend of the disease in Fars province, southern Iran.
Methods:
This historical retrospective cohort study was carried out in Fars Multiple Sclerosis Society affiliated with Shiraz University of Medical Sciences. All the consecutive patients who fulfilled 2010 McDonald criteria for definite MS were included in the study. The patients’ gender, age at time of diagnosis, education, and clinical course were recorded. The prevalence and incidence rates were also calculated.
Results:
This study was conducted on 3,354 patients. Among the patients, 2,689 (80.2%) were female and 665 (19.8%) were male. The female/male ratio was 4.04. The point prevalence rate of the disease was 72.1/100,000 persons in October 2013. This index was 116.5 per 100,000 persons in females (95% CI: 113.4-119.6) and 28.3 per 100,000 persons in males (95% CI: 26.8-29.9). The mean annual incidence rate was 5.2/100,000 from 2002 until 2012.
Conclusion:
Considering Kurtzke classification, Fars is a high-risk area for MS and women are affected more compared with men. Moreover, the incidence rate sharply increased in the last decade.
Keywords: Multiple sclerosis, Incidence, Prevalence, Iran
Introduction
Multiple Sclerosis (MS) is a chronic inflammatory and demyelinating disease of the central nervous system, which is accompanied by significant disabilities.1
Twenty years ago, Kurtzke G. suggested three prevalence areas of MS in the world, namely low (5 per 100,000 population), medium (5-30 per 100,000 population), and high-risk areas (more than 30 per 100,000 population).2 High-risk areas were seen in Northern Europe, Northern America, Canada, Southern Australia, and New Zealand. On the other hand, medium risk areas included Asia, South America, and other uncharted regions.3-5 Based on Kurtzke classification, the Middle Eastern countries were considered as low risk areas for MS. Previously, Iran was considered to have a low prevalence rate of MS, but this rate has significantly increased in the recent years.6 Fars province is located between longitudes of 50°36’E and 55°35’E of Greenwich and latitudes of 27°03’N and 31°40’N of the equator. It has an area of 122,608 km with three distinct climatic regions and a total population of 4,651,718 until October 2013.7,8
Although there are some published data regarding the epidemiological features of MS in other parts of Iran,9-12 scarce data are available about the prevalence and demographic characteristics of MS in Fars province. Therefore, the current study aims to address the prevalence and incidence rates of MS as well as the temporal trend of the disease in Fars province, southern Iran, which is one of the largest provinces of the country.
Patients and Methods
This historical, retrospective cohort study was conducted on the data from all patients who had MS (all subtypes of MS) according to the McDonald’s criteria. They were members of the Fars Multiple Sclerosis Society (FMSS) until October 2013. All patients were referred to the MS committee of Shiraz University of Medical Sciences by neurologists and were again reevaluated by three expert neurologists to confirm their diagnosis. This is the only referral center for MS patients in Fars province and, as a result, nearly all the MS patients are registered in this computerized database. A few patients from other neighboring provinces also were registered in this database and were excluded from the study. Additional information about the patients’ gender, age at time of diagnosis, education, and clinical course were obtained from this database. The population figures for Fars province were used as the denominators for calculation of prevalence and incidence rates. Based on the information released by the Iranian central bureau, which is derived from the national census, the population of Fars province was 4,651,718 in October 2013.7 The prevalence rate of the disease was calculated considering the total number of patients and the population of Fars province in October 2013. Besides, the annual incidence rates were calculated based on the new cases diagnosed with each year and yearly estimated population of Fars province from 2002 to 2012.
Statistical Analysis
All data were analyzed using the SPSS statistical software (version 15.0). The results were reported as descriptive indices, such as frequency (percentage) and mean±standard deviation. The independent t-test was used to compare the means of age and sex in the patients with clinically isolated syndrome (CIS) and relapsing remitting MS (RRMS). In addition, 95% confidence interval (95% CI) of mean age was computed. The prevalence and incidence rates of MS were computed with respect to sex and year with 95% CI. P<0.05 was considered as statistically significant.
Results
A total of 3,354 MS patients were identified in this study. Among the study patients, 2,689 (80.2%) were female and 665 (19.8%) were male with a female/male ratio of 4.04.
The mean age of the patients was 32.94±9 years (95% CI: 32.63-33.25). In addition, the mean age of the male and female patients was 33.24±8.9 (32.5-33.9) and 32.86±9.5 (32.5-33.2) years, respectively. Moreover, about 73.8% of the patients were between 20-40 years of age. The youngest patient was 11 and the oldest one was 74 years old.
Considering the population of Fars province in October 2013 (female population: 2,398,113; male population: 2,343,705; and the total population: 4,651,718), the total point prevalence rate of MS was 72.1 per 100,000 persons (95% CI: 69.6-74.5).
Besides, the sex-specific prevalence rate of the disease was 116.5 (95% CI: 113.4-119.6) per 100,000 persons in females and 28.3 per 100,000 persons (95% CI: 26.8-29.9) in males. It should be mentioned that the total prevalence rate of the disease was 20.5/100,000 in 2002 (7.8 in males and 33.2 in females).
Among the study patients, 2,476 cases were in 20-40 year old age group with the age specific prevalence rate of 148.3 per 100,000 persons (238.5 for females and 59.6 for males).
The study findings revealed the mean annual incidence rate of 5.2/100,000 from 2002 to 2012. The incidence rate of the disease was 4.1/100,000 in 2002 and increased to 8.98/100,000 in 2012. Therefore, in the last 11 years (2002 to 2012), 2.2- and 3.57-fold increase was observed in the incidence and prevalence rates of MS, respectively. This increasing rate was seen in both females and males, but significantly more in females. The increasing incidence rate during the last 11 years is shown in figure 1. Considering the type of MS, the increasing rate was seen predominantly in CIS, while a decrease in frequency was detected in RRMS, as shown in figure 2.
Figure 1.
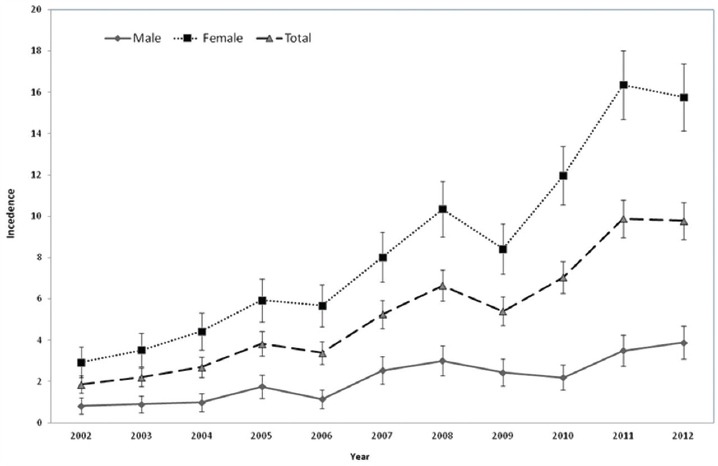
The annual incidence rate (95% CI) of multiple sclerosis in Fars province from 2002-2012 indicates an increasing incidence rate (especially in females) in Fars province during the last 11 years.
Figure 2.
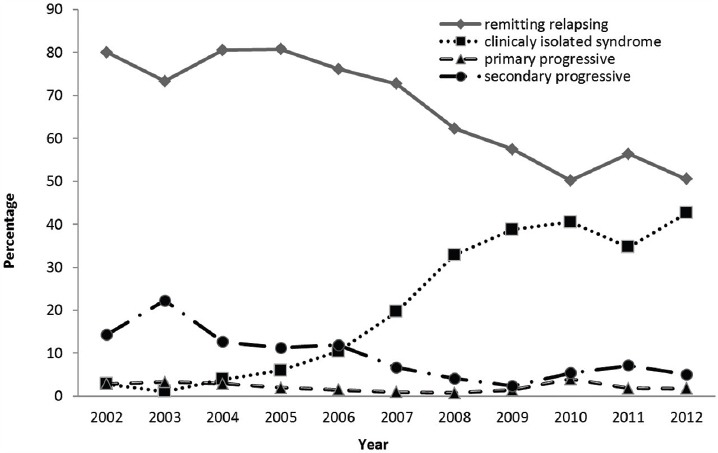
The frequency of clinical types of multiple sclerosis in Fars province from 2002-2012 shows, considering the type of MS, the increasing rate is seen predominantly in CIS while a decrease in frequency is detected in RRMS.
According to the results, the most frequent type of MS was RRMS (n=1851 patients, 61.5%) followed by CIS (n=842 patients, 28%). The mean age of the patients with CIS and RRMS was 30.2±8.4 (95% CI: 29.6-30.8) and 33.4±8.39 (95% CI: 33-33.8) years, respectively.
Discussion
Our study revealed that Fars province is a high-risk area for MS with the total prevalence rate of 72.1 per 100,000 persons (116.5/100, 000 in females and 28.3/100,000 in males). Previously, Iran was considered to have a low prevalence rate of MS according to Kurtzke categorization.2 However, recently published data revealed that some areas of Iran could be considered as high prevalence areas. The prevalence rate of MS was reported to be 35.5 per 100,000 (2006, Etemadifar M. et al.) and 73.3 per 100,000 (2011, Etemadifar M. et al.) in Isfahan (central of Iran),6,10 51.9 per 100,000 in Tehran (2010, Sahraian MA. et al.),11 20 per 100,000 in Mazandaran (north of Iran),12 5-12 per 100,000 in Khorasan (northeast of Iran),13 and 14 per 100,000 in Sistan and Baluchistan (southeast of Iran).14 Accordingly, the prevalence rate of MS significantly varies in different provinces of the country. Iran is a large country with different climates, ethnicities, and cultures. Thus, these differences in prevalence rates in different regions could be explained, at least to some extent, by these ethnic and environmental differences. Yet, why the prevalence rate in central and large provinces of Iran (Tehran, Isfahan, and Fars) is significantly higher compared to that in other provinces is not exactly clear.
Many environmental and genetic factors are considered as the contributing factors in the etiology of MS. Several reports have indicated that the prevalence of MS is higher in the regions with low sun exposure and vitamin D deficiency.15
Etemadifar et al. also suggested vitamin D deficiency as an important factor, which could affect the prevalence of MS in Iran. Although it is believed that the Iranian population has enough sun exposure, vitamin D deficiency is still prevalent in the country.10 One of the reasons that may explain the high rate of vitamin D deficiency in Iran is the lifestyle changes, such as extensive use of sunscreens or an increase in the number of people living in apartments where there is a significant decrease in sun exposure. Moreover, hijab was mentioned as a possible contributing factor to vitamin D deficiency in the Iranian population, however, there is no other documented evidence that could confirm this hypothesis.16
Furthermore, a previous study demonstrated a correlation between the prevalence of MS and specific types of heavy industries.17 The present and previous studies shown the highest prevalence rate of MS in Iranian provinces (e.g., Isfahan, Tehran, and Fars) with the highest rates of industrial activity. Industrial activity in these provinces might have contributed to this high prevalence rate.
The hygiene hypothesis may provide the explanation why there has been an increase in the prevalence rate of MS in the region. Epidemiological studies have suggested that reduced exposure to infection may be an explanation for the increased incidence of allergic and autoimmune diseases.18 Isfahan, Tehran, and Fars are three provinces with the highest socioeconomic status. These provinces also have the best hygiene among Iranian provinces. The improvement of hygiene among the Iranian population in the last decade could be the other environmental factor affecting the increasing prevalence rate of MS in Iran. In addition, some studies in India showed that MS was significantly more prevalent among Parsis (originated from Pars province, Iran) compared with other ethnic groups.19
However, the prevalence rate of MS in Fars province was higher compared with other Middle Eastern countries. The prevalence rate of the disease was reported to be 31.15/100,000, 25/100,000, and 40/100,000 in Kuwait, Saudi Arabia, and Jordan, respectively.20-22 On the other hand, the prevalence rate of MS in Eastern Asia was much lower compared with Iran and other Middle Eastern countries.23-25
Evidence has shown that environmental factors play an important role in acquisition of MS. However, considering the differences in the prevalence rates of MS in Iran and other Middle Eastern countries as well as the higher rate of MS among Persian ethnic groups in India, we advocate that genetic susceptibility and ethnicity might play a more significant role in the Iranian’s susceptibility to MS.
Alonso A. et al. in a systematic review (2008) reported that the overall worldwide incidence rate of MS was 3.6 and 2.0 cases per 100,000 person-years in females and males, respectively.26 In the current study, the mean annual incidence rate of MS was 5.2/100,000 persons and a 2.2-fold increase was observed in the incidence rate of MS in Fars province from 2002 to 2012. This increasing rate was more prominent in females. The increasing incidence and prevalence rates of MS were also reported in the previous Iranian studies.10-12
To date, 55% of the Iranian population belongs to the 15-30 years age group.7 MS mostly occurs in young patients and the predominance of young population in Iran may justify the high prevalence of MS in this country. Therefore, potential decrease in the number of young population in Iran in the coming years may result in a decrease in the incidence rate of the disease. The other possible contributing factors to the increasing rate of MS are improved diagnostic tools, such as MRI, and better and earlier diagnosis. In addition, there have been some reports of the increasing trend of other autoimmune diseases, such as Guillaine Barre syndrome, in Iran.27 Thus, conducting meticulous basic and clinical researches are highly recommended on the causes of this trend.
According to figure 2, in the recent years, the number of patients diagnosed with CIS has increased, while the prevalence rate of RRMS has decreased. The reason for this change is probably increasing knowledge about the disease and high suspicious of physicians that lead them to earlier diagnosis in earlier stages of the disease when the patient has only had one attack of neurological deficit. Revised MacDonald’s criteria (2010) and more available Magnetic Resonance Imaging (MRI), the gold standard tool for MS diagnosis, have also helped easier diagnosis in the earlier stages of the disease. The findings of this study indicated that the prevalence of secondary progressive MS has decreased in the recent years. This might be due to the fact that the patients are diagnosed in the early stages of the disease and are treated with disease modifying drugs. Early treatment of the patients with disease modifying drugs, including Beta-Interferon, can delay progression of the disease into secondary progressive MS.28
In the current study, female to male ratio was 4.04:1, which is similar to other studies performed in Iran.10-13 Yet, this ratio has been reported as 2-3:1 in the western population, but 6-9:1 in East Asian countries.1,23-25 The prevalence of MS in some areas of Iran is similar to Caucasians, but the sex ratio is different, which is an interesting finding also reported in some previous studies.
The higher rate of MS among women may be related to their physiological factors, including sex hormones. Additionally, the increasing incidence of MS in females suggests that the hormonal differences make women more susceptible to environmental risk factors.29 These exogenous factors contributing to the pathogenesis of MS could affect men and women differently.30
In the Iranian population, the number of female smokers is significantly lower than male smokers are, but low sunlight exposure and its associated vitamin D deficiency are significantly higher among females.
Alvaro Alonso in a systematic review reported that the female to male ratio increased from 1.4 in 1955 to 2.3 in 2000.26 Therefore, the female to male ratio has increased from past to present as well as from west to east.
Most of the patients in this study had RRMS (61.5%) followed by CIS (28%). This is in agreement with other studies conducted around the world, including Asian and Middle Eastern countries.15-21
Conclusion
The current study revealed that the Fars province had high prevalence and incidence rates of MS. In addition, a sharp increase was observed in the incidence rate of the disease in the last decade.
Acknowledgement
The authors are grateful for Mr. Nosrati for his cooperation in data collection. Ms. A. Keivanshekouh at the Research Improvement Center of Shiraz University of Medical Sciences is also appreciated for improving the use of English in the manuscript.
Conflicts of Interest: None declared.
References
- 1.Pugliatti M, Rosati G, Carton H, Riise T, Drulovic J, Vécsei L, et al. The epidemiology of multiple sclerosis in Europe. Euro J Neurol. 2006;13:700–22. doi: 10.1111/j.1468-1331.2006.01342.x. [DOI] [PubMed] [Google Scholar]
- 2.Kurtzke JF. Epidemiologic contributions to multiple sclerosis:an overview. Neurology. 1980;30:61–79. doi: 10.1212/WNL.30.7_Part_2.61. [DOI] [PubMed] [Google Scholar]
- 3.Kantarci O, Wingerchuk D. Epidemiology and natural history of multiple sclerosis:new insights. Curr Opin Neurol. 2006;19:248–54. doi: 10.1097/01.wco.0000227033.47458.82. [DOI] [PubMed] [Google Scholar]
- 4.Alonso A, Jick SS, Olek MJ, Hernán MA. Incidence of multiple sclerosis in the United Kingdom:findings from a population-based cohort. JNeurol. 2007;254:1736–41. doi: 10.1007/s00415-007-0602-z. [DOI] [PubMed] [Google Scholar]
- 5.Simpson S, Jr, Blizzard L, Otahal P, Van der Mei I, Taylor B. Latitude is significantly associated with the prevalence of multiple sclerosis:a meta-analysis. 2011; 82:1132–41. doi: 10.1136/jnnp.2011.240432. [DOI] [PubMed] [Google Scholar]
- 6.Izadi S, Nikseresht A, Sharifian M, Sahraian MA, Hamidian Jahromi A, Aghighi M, et al. Significant increase in the prevalence of multiple sclerosis in iran in 2011. Iran J Med Sci. 2014;39:152–3. [ PMC Free Article] [PMC free article] [PubMed] [Google Scholar]
- 7.Iran at a glance, Fars:land area/population [Internet] Statistical center of Iran c2011,-[updated 2013 June 11; cited 2014 July 7] Available from: http://www.amar.org.ir/Default.aspx?tabid=1201 .
- 8.Fars Province [Internet] Wikipedia:The Free Encyclopedia Wikimedia Foundation, Inc., [updated 10 May 2014; cited 24 May 2014] Available from: http://en.wikipedia.org/wiki/Fars/province .
- 9.Kalanie H, Gharagozli K, Kalanie AR. Multiple sclerosis:report on 200 cases from Iran. Mult Scler. 2003;9:36–8. doi: 10.1191/1352458503ms887oa. [DOI] [PubMed] [Google Scholar]
- 10.Etemadifar M, Janghorbani M, Shaygannejad V, Ashtari F. Prevalence of multiple sclerosis in Isfahan, Iran. Neuroepidemiology. 2006;27:39–44. doi: 10.1159/000094235. [DOI] [PubMed] [Google Scholar]
- 11.Sahraian MA, Khorramnia S, Ebrahim MM, Moinfar Z, Lotfi J, Pakdaman H. Multiple sclerosis in Iran:a demographic study of 8,000patients and changes over time. Euro Neurol. 2010;64:331–6. doi: 10.1159/000321649. [DOI] [PubMed] [Google Scholar]
- 12.Abedidni M, Habibi Saravi R, Zarvani A, Farahmand M. Epidemiologic study of multiple sclerosis in Mazandaran, Iran, 2007. J Mazandaran Univ Med Sci. 2008;18:82–6. [Google Scholar]
- 13.Ghandehari K, Riasi HR, Nourian A, Boroumand AR. Prevalence of multiple sclerosis in north east of Iran. Mult Scler. 2010;16:1525–6. doi: 10.1177/1352458510372150. [DOI] [PubMed] [Google Scholar]
- 14.Moghtaderi A, Rakhshanizadeh F, Shahraki-Ibrahimi S. Incidence and prevalence of multiple sclerosis in southeastern Iran. Clin Neurol Neurosurg. 2013;115:304–8. doi: 10.1016/j.clineuro.2012.05.032. [DOI] [PubMed] [Google Scholar]
- 15.Pierrot-Deseilligny C, Souberbielle JC. Is hypovitaminosis D one of the environmental risk factors for multiple sclerosis? Brain. 2010;133:1869–88. doi: 10.1093/brain/awq147. [DOI] [PubMed] [Google Scholar]
- 16.Maghzi AH, Sahraian MA, Shaygannejad V, Minagar A. Is the Iranian revolution to blame for the increasing incidence of multiple sclerosis in Iran? Neuroepidemiology. 2013;40:68–9. doi: 10.1159/000341848. [DOI] [PubMed] [Google Scholar]
- 17.Boström I, Landtblom AM, Lauer K. An ecological study of industry in a high-risk region of multiple sclerosis. J Neurol Sci. 2011;311:50–7. doi: 10.1016/j.jns.2011.09.005. [DOI] [PubMed] [Google Scholar]
- 18.Correale J, Farez MF. The impact of environmental infections (parasites) on MS activity. Mult Scler. 2011;17:1162–9. doi: 10.1177/1352458511418027. [DOI] [PubMed] [Google Scholar]
- 19.Pandit L. Insights into the changing perspectives of multiple sclerosis in India. Autoimmune Dis. 2011;2011:937586. doi: 10.4061/2011/937586. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Hashel J, Besterman AD, Wolfson C. The prevalence of multiple sclerosis in the Middle East. Neuroepidemiology. 2008;31:129–37. doi: 10.1159/000151514. [DOI] [PubMed] [Google Scholar]
- 21.Bohlega S, Inshasi J, Al Tahan AR, Madani AB, Qahtani H, Rieckmann P. Multiple sclerosis in the Arabian Gulf countries:a consensus statement. J Neurol. 2013;260:2959–63. doi: 10.1007/s00415-013-6876-4. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.El-Salem K, Al-Shimmery E, Horany K, Al-Refai A, Al-Hayk K, Khader Y. Multiple sclerosis in Jordan:Aclinical and epidemiological study. J Neurol. 2006;253:1210–6. doi: 10.1007/s00415-006-0203-2. [DOI] [PubMed] [Google Scholar]
- 23.Quintana-Murci L, Chaix R, Wells RS, Behar DM, Sayar H, Scozzari R, et al. Where west meets east:the complex mtDNA landscape of the southwest and Central Asian corridor. Am J Hum Genet. 2004;74:827–45. doi: 10.1086/383236. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Siritho S, Prayoonwiwat N. A retrospective study of multiple sclerosis in Siriraj Hospital, Bankok, Thailand. Can J Neurol Sci. 2007;34:99–104. doi: 10.1017/S0317167100005874. [DOI] [PubMed] [Google Scholar]
- 25.Lau KK, Wong LK, Li LS, Chan YW, Li HL, Wong V. Epidemiological study of multiple sclerosis in Hong Kong Chinese:questionnaire survey. Hong Kong Med J. 2002;8:77–80. [PubMed] [Google Scholar]
- 26.Alonso A, Hernán MA. Temporal trends in the incidence of multiple sclerosis:a systematic review. Neurology. 2008;71:129–35. doi: 10.1212/01.wnl.0000316802.35974.34. [ PMC Free Article] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Safari A, Borhani-Haghighi A, Heydari ST, Lankarani KB. Increased Guillain-Barre syndrome admissions in Shiraz, southern Iran. Iran J Neurol. 2013;12:15–8. [ PMC Free Article] [PMC free article] [PubMed] [Google Scholar]
- 28.Compston A, Coles A. Multiple sclerosis. Lancet. 2008;372:1502–17. doi: 10.1016/S0140-6736(08)61620-7. [DOI] [PubMed] [Google Scholar]
- 29.Orton SM, Herrera BM, Yee IM, Valdar W, Ramagopalan SV, Sadovnick AD, et al. Sex ratio of multiple sclerosis in Canada:a longitudinal study. Lancet Neurol. 2006;5:932–6. doi: 10.1016/j.bbr.2011.03.031. [DOI] [PubMed] [Google Scholar]
- 30.Ebers GC. Environmental factors and multiple sclerosis. Lancet Neurol. 2008;7:268–77. doi: 10.1016/S1474-4422(08)70042-5. [DOI] [PubMed] [Google Scholar]