

Case report
Case 1
A 21-year-old Malay woman presented with a 4-day history of left eye progressive painful blurring of vision due to cosmetic CL wear. She had always bought her CLs from a night market and disposed it after every 3–4 months. She had a very poor CL hygiene regime and continuously wore the lenses for more than 8 hours daily. Prior to the presentation, she had been using a combination of steroid and antibiotic eye drop as prescribed by a general practitioner whom she had consulted earlier for similar complaints of eye redness and pain associated with reduced vision. Her condition and vision deteriorated after 2 days of medication instillation.
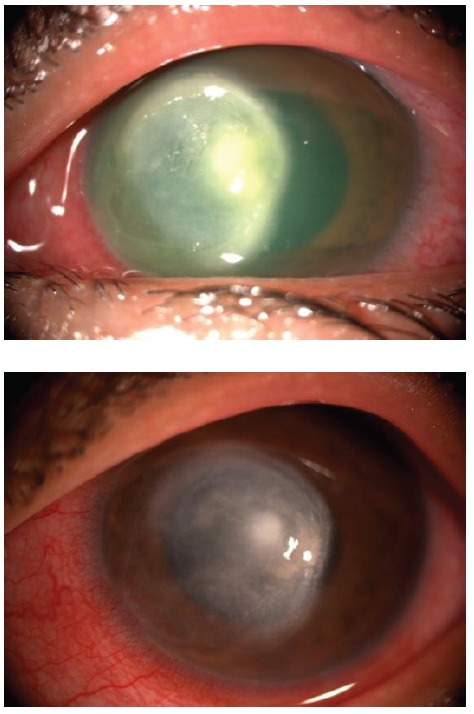
At presentation, visual acuity of the left eye was counting fingers. There was a large central corneal abcess obscuring the visual axis associated with central stromal melting (Figure 1). Also, there was significant anterior chamber cells inflammation with hypopyon level.
Figure 1: Large central corneal ulcer encroaching limbus nasally with dense stromal infiltrates (top), resulting in dense scar once healed (bottom).
Culture and sensitivity of the cornea scraping revealed Pseudomonas aeruginosa infection. The patient was admitted for intensive treatment with a combination of intensive topical antibiotics, comprising topical ceftazidime 5% and topical gentamicin 1.4%. Oral ciprofloxacin 500 mg BD was added as a prophylaxis for sclera abcess due to the close proximity of the original ulcer to the sclera.
The ulcer eventually healed with a large central dense scar following 3 weeks of inpatient stay. Final visual acuity was 6/60 and corneal graft was offered in a view of poor vision.
Case 2
A 19-year-old woman presented with a 3-day history of left eye painful blurring of vision associated with whitish discoloration of the cornea. She had slept overnight while having the cosmetic CL bought from a night market a few days back.
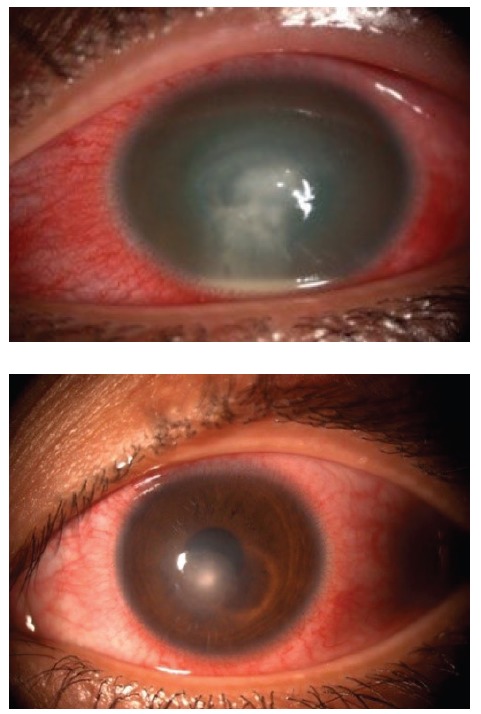
On examination, the left eye vision acuity was counting fingers due to a central corneal ulcer with dense stromal abscess. Anterior chamber activity was intense with hypopyon level (Figure 2 ). Other ocular examinations were normal.
Figure 2: Central corneal ulcer with dense infiltrates and hypopyon (top), which healed with paracentral scar (bottom).
She was treated for bacterial keratitis using the similar combination of topical antibiotics. The ulcer gradually improved and the patient was allowed to discharge after 4 weeks of inpatient treatment. The final visual acuity was 6/24.
Discussion
Worldwide, approximately 85 million of people are using CL either for optical or cosmetic purposes. In Malaysia, the popularity of cosmetic CL use is also increasing, largely among the younger age group. Therefore, it is not surprising that the incidence of contact lens-related ulcer (CLRU) is also on the rise due to poor CL care and hygiene regime. Approximately 80% of CLRU patients are culture-positive, and more than 75% of these resulted in colonisation by gram-negative bacteria.1 An alarming trend of cosmetic CLs bought at night or flea market is on the rise due to lack of awareness among the public and its much cheaper price. The multiple lens selection ‘over-the-counter’ is also appealing to the public as these lenses appear similar to the more expensive options available in the optical shops.
In Malaysia, cosmetic CLs are being dispensed by unlicensed vendors and are rampantly sold at flea market. Patients who acquire lenses from unauthorised providers are less likely to be informed about appropriate lens use and care. In a case series of reported 13 patients with severe coloured contact lens-related microbial keratitis, the users had no significant refractive error.2 They acquired the lenses from unlicensed optical shop or had shared lenses with relatives or friends.2 Furthermore, CL solutions and casings were usually kept in bathroom, where microorganism lurking and possibility of contamination was very high. Most optician and sellers do not advice on CL hygiene and proper care and cleaning of the lens and the lens casings. Consequently, the risk of suffering from debilitating sequelae and sightthreatening consequences are higher.3
Cosmetic CL use is most popular among college students. A study on regular CL users among this group of population showed that contamination with microorganism was up to approximately 21% with lens casings being the most frequently contaminated item.4 Pseudomonas aeruginosa, Klebsiella sp. and E. coli were among the most common organisms isolated from the cultures from either lens casings, solutions or the lens itself.4 These gram-negative bacteria are usually sensitive to aminoglycosides in our local setting. Topical gentamicin is effective and safe for the eye and the solution is also available in multiple concentrations; hence, it is used as first-line empirical treatment against CLRU. Resistance to antibiotic is a significant concern among ophthalmologist,5 therefore, a second antibiotic is advocated. Furthermore, aminoglycosides largely cover gram-negative bacteria and another antimicrobial agent against gram-positive bacteria should be added. More importantly, topical steroid must always be used with caution in infective corneal cases. This medication helps to reduce the associated inflammation and scarring, but the infection may worsen drastically and corneal melt may also ensue.
Corneal ulcer from CL use typically arises from bacterial contamination of the lenses, either from the lid margin or from environment. Tap water is a notorious source of microbial infection and people usually use tap water to rinse the casings. Microbial adherence to CLs and corneal epithelium depends on its virulence and the material of the CL. Lenses with higher water contents tend to cause inoculation of Pseudomonas aeruginosa,3 which probably explains the high number of infection cultured from CLRU.
Proper CL care and hygiene are one of the most important modifiable risk factor for CLRU.6 In some countries, proper licensing and thorough information of CL care is mandatory. Furthermore, CL should only be available through prescription, and definitely should not be freely available at flea market.
In the United States, the FDA provides thorough information on purchasing CL including health warnings when CL are purchased without a prescription and worn incorrectly. It is illegal to sell CL at a flea market or beauty shop. Vendors can only sell CL to buyers who have prescription from an ophthalmologist or optometrist. Although, appropriate lens care and hygiene does not fully eliminate the risk of developing corneal infection,6 to a large extent these measures are important to protect the ocular surface. Hence, primary care physicians, opticians and medical personnel should be familiar with proper hygiene and CL care. In the event of corneal infection, especially from CL use, urgent ophthalmology referral will be vision saving.
Conclusion
CLRU or microbial keratitis is an important cause of ocular surface morbidity. Readily available CL sold at night or flea market poses a major issue and may possibly cause more CLRU. Hence, people, especially the younger age group should be educated and informed on proper technique of CL care and hygiene. In an era of cosmetic CL becoming a fashionable trend more than an optical device, users must be warned against possible visual-threatening sequelae from improper CL use and care.
Footnotes
Ayesha MZ, Umi Kalthum MN, Jemaima CH, Faridah HA. Night market contact lens-related corneal ulcer: Should we increase public awareness? Malays Fam Physician. 2015;10(1):47-49.
References
- 1.Loh KY, Agarwal P. Malays Fam Physician. 2010;5:6–8. [PMC free article] [PubMed] [Google Scholar]
- 2.Steinemenn TL, Fletcher M, Bonny AE. et al. Over the counter decorative contact lenses: Cosmetic or medical devices? A case series. Eye Contact Lens. 2005;81:194–200. doi: 10.1097/01.icl.0000175654.79591.03. [DOI] [PubMed] [Google Scholar]
- 3.Tuli L, Bhatt GK, Singh DK. et al. Dark secrets behind the shimmer of contact lens: The Indian scenario. BMC Res Notes. 2009;2:79. doi: 10.1186/1756-0500-2-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Willcox MD, Holden BA. Contact lens related corneal infections. Biosci Rep. 2001;21:445–61. doi: 10.1023/a:1017991709846. [DOI] [PubMed] [Google Scholar]
- 5.Mohammadpour M, Mohajernezhadfard Z, Khodabandev A. et al. Antibiotic susceptibility patterns of Pseudomonas corneal ulcers in contact lens wearers. Middle East Afr J Ophthalmol. 2011;18:228–31. doi: 10.4103/0974-9233.84053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Goh PP, Shamala R, Chandramalar S. et al. Contact lens-related corneal ulcer: A twoyear review. Med J Malaysia. 2010;65:120–3. [PubMed] [Google Scholar]
- 7.Najjar DM, Aktan SG, Rapuano CJ. et al. Contact lens-related corneal ulcers in compliant patients. Am J Ophthalmol. 2004;137(1):170–2. doi: 10.1016/s0002-9394(03)00722-0. [DOI] [PubMed] [Google Scholar]