

Abstract
Necrotic pancreatic collections are difficult to treat endoscopically due to a concern for inadequate drainage of the necrotic debris. Multiple techniques including the use of metallic stents, endoscopic necrosectomy and use of hybrid approaches utilizing endoscopic and percutaneous approaches have been described for the management of pancreatic necrotic collections. Furthermore, multiple transluminal gateway technique has been used to create endosonography guided multiple tracts to drain a perigastric or periduodenal collection. We hereby report about a patient with walled off necrosis resulting as a complication of alcohol related acute pancreatitis that was drained using endoscopic ultrasound-guided approach. However, a spontaneous cystoduodenal fistula was used to create another tract and place transmural stents resulting in a quick resolution of symptoms.
Keywords: Endosonography, pancreatic duct, pancreatic necrosis
INTRODUCTION
Innovations in endoscopic management of pancreatic fluid collections (PFCs) have improved the management of local complications of acute pancreatitis including infected necrosis.[1,2] While the treatment of pseudocyst is feasible by creation of a route for internal drainage of pancreatic fluid using endoscopic means, treatment of necrotic collections is more complex warranting the use of many innovations including nasocystic drainage, dilatation of tract and endoscopic necrosectomy and use of metallic stents to provide a better access to the cavity for insertion of endoscope and performing direct necrosectomy.[3] In this context, creation of multiple openings between the gastrointestinal tract and the collection as in multiple transluminal gateway techniques (MTGT) has been suggested as an approach to allow better drainage in the treatment of PFCs.[4] We hereby report about a case of pancreatic necrosis who underwent endoscopic ultrasound (EUS) guided drainage of PFC, and the presence of a spontaneous cystoduodenal fistula was used to create MTGT, which helped in a quicker resolution of patient's symptoms.
CASE REPORT
A 32-year-old male presented with abdominal pain and fever of 5 days duration. He was diagnosed as alcohol-related acute necrotizing pancreatitis 2 months ago and was managed elsewhere where he was noted to have transient lung injury. He had been discharged after 8 days of admission and now was symptomatic with episodes of abdominal pain and had developed hectic fever. Evaluation revealed leukocytosis (total leucocyte count of 21,300/mm3) and normal liver and kidney functions. Contrast-enhanced computed tomography of the abdomen revealed large walled-off pancreatic necrosis (WOPN) [Figure 1]. Intravenous meropenem was initiated, but the fever and leukocytosis did not respond to the antibiotics. Two days later, in view of the possibility of infected WOPN the patient was taken up for endoscopic drainage. EUS guided transluminal drainage of perigastric WOPN was done, and two transluminal stents were placed [Figure 2]. As the endoscope was advanced into the duodenum, a small opening plugged with purulent material was noted on the medial wall of the duodenum, adjacent to the major papilla [Figure 3]. This opening was cannulated and dilated up to 12 mm using controlled radial expansion (CRE; Boston Scientific India Pvt. Ltd., Gurgaon) balloon [Figures 4 and 5]. Thick purulent material came out of the dilated opening [Figure 4] and we placed two transluminal pigtail stents. The pancreatic duct was also cannulated, and pancreatogram revealed partial disruption that was bridged with a 5 Fr stent [Figure 6]. The patient had marked improvement in his symptoms and was discharged on oral antibiotics.
Figure 1.

Computed tomography abdomen: Large walled off pancreatic necrosis (WOPN) in perigastric and periduodenal location. The small perigastric collection is communicating with the large perigastric WOPN
Figure 2.

Endoscopic ultrasound guided drainage of perigastric walled off pancreatic necrosis. The tract being dilated with balloon (arrows)
Figure 3.
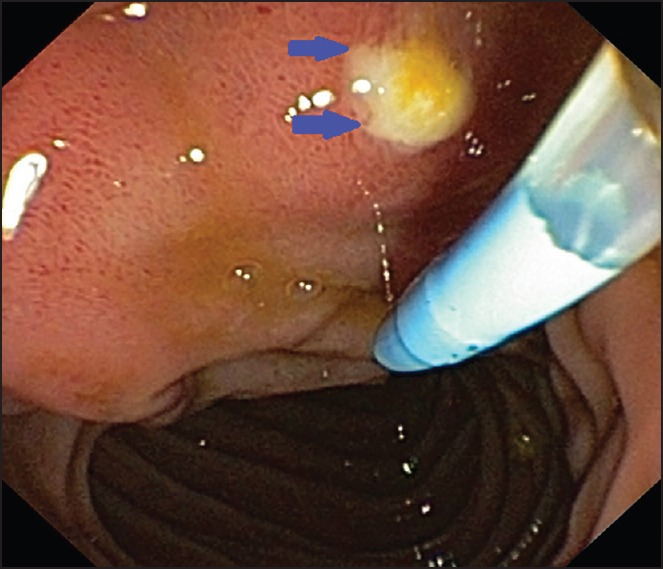
Small opening plugged with purulent material noted on the medial wall of duodenum (blue arrow)
Figure 4.

The opening being cannulated. Major papilla can be seen (arrow). Purulent material seen coming out of the opening
Figure 5.

Balloon dilatation of the opening
Figure 6.
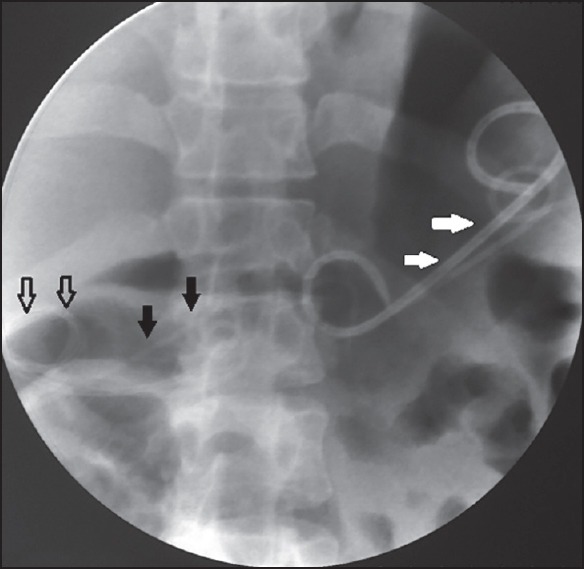
Multiple transluminal stents in perigastric (white arrow) and periduodenal walled off pancreatic necrosis seen (black open arrow). Transpapillary pancreatic duct stent also seen (black arrow)
DISCUSSION
With the availability of EUS and better accessories, endoscopic therapy for WOPN has yielded encouraging results.[2,5] However, ineffective drainage of necrotic debris remains an important concern with endoscopic methods to treat necrotic collections. The nature and amount of necrotic/solid debris decrease with time after the episode of acute pancreatitis and the amount of debris at the time of intervention predict the aggressiveness of the interventions as also the number of procedures needed.[6,7] Also by using more aggressive techniques like larger tract dilation, placement of multiple stents, aggressive irrigation and direct debridement of necrotic tissue, more effective drainage of solid necrotic material can be achieved. MTGT of creating several openings in the stomach or duodenum has also been shown to facilitate drainage and thus improve the treatment outcomes.[4] In a report on the use of the MTGT for creating multiple endosonography guided transmural drainage, the success rate of treatment was higher in the 12 patients treated with the MTGT technique.[4] In the present report, a natural fistulization of the walled off necrosis with the duodenum was utilized to create multiple transluminal gateways and the patient improved within a week of the procedure and was discharged. Multiple tracts are likely to result in a quicker drainage and lesser chances of infection.[4] Indeed a hybrid approach using the MTGT technique with the use of percutaneous drainage has also been described suggesting that more the drains the better the drainage.[8] To the best of our knowledge, this is the first report to suggest that the site of natural fistulization can be utilized to create a multiple transluminal gateway for the drainage of the contents of pancreatic collections.
Footnotes
Source of Support: Nil
Conflicts of Interest: None declared.
REFERENCES
- 1.Fisher JM, Gardner TB. Endoscopic therapy of necrotizing pancreatitis and pseudocysts. Gastrointest Endosc Clin N Am. 2013;23:787–802. doi: 10.1016/j.giec.2013.06.013. [DOI] [PubMed] [Google Scholar]
- 2.Rana SS, Bhasin DK, Rao C, et al. Non-fluoroscopic endoscopic ultrasound-guided transmural drainage of symptomatic non-bulging walled-off pancreatic necrosis. Dig Endosc. 2013;25:47–52. doi: 10.1111/j.1443-1661.2012.01318.x. [DOI] [PubMed] [Google Scholar]
- 3.Gornals JB, De la Serna-Higuera C, Sánchez-Yague A, et al. Endosonography-guided drainage of pancreatic fluid collections with a novel lumen-apposing stent. Surg Endosc. 2013;27:1428–34. doi: 10.1007/s00464-012-2591-y. [DOI] [PubMed] [Google Scholar]
- 4.Varadarajulu S, Phadnis MA, Christein JD, et al. Multiple transluminal gateway technique for EUS-guided drainage of symptomatic walled-off pancreatic necrosis. Gastrointest Endosc. 2011;74:74–80. doi: 10.1016/j.gie.2011.03.1122. [DOI] [PubMed] [Google Scholar]
- 5.Bang JY, Wilcox CM, Trevino J, et al. Factors impacting treatment outcomes in the endoscopic management of walled-off pancreatic necrosis. J Gastroenterol Hepatol. 2013;28:1725–32. doi: 10.1111/jgh.12328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rana SS, Bhasin DK, Reddy YR, et al. Morphological features of fluid collections on endoscopic ultrasound in acute necrotizing pancreatitis: Do they change over time? Ann Gastroenterol. 2014;27:258–61. [PMC free article] [PubMed] [Google Scholar]
- 7.Rana SS, Bhasin DK, Sharma RK, et al. Do the morphological features of walled off pancreatic necrosis on endoscopic ultrasound determine the outcome of endoscopic transmural drainage? Endosc Ultrasound. 2014;3:118–22. doi: 10.4103/2303-9027.131039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Varadarajulu S. A hybrid endoscopic technique for the treatment of walled-off pancreatic necrosis. Am J Gastroenterol. 2013;108:1015–7. doi: 10.1038/ajg.2013.113. [DOI] [PubMed] [Google Scholar]