

Abstract
Objectives
Fibromyalgia has seldom been associated with coronary heart disease (CHD). The aim of this study was to evaluate the risk of CHD in patients with fibromyalgia.
Methods
We used a dataset of one million participants, systemically scrambled from the Taiwanese national insurance beneficiaries, to identify 61,612 patients with incident fibromyalgia (ICD-9-CM 729.0–729.1) and 184,834 reference subjects matched by sex, age and index date of diagnosis in a 1:3 ratio from 2000 to 2005, with a mean 8.86 ± 2.68 years of follow-up until 2011. Risk of CHD was analyzed by Cox proportional hazard modeling.
Results
Patients with fibromyalgia had a mean age of 44.1 ± 16.5 years. CHD events developed in fibromyalgia patients (n = 8,280; 15.2 per 103 person-years) and reference subjects (n = 15,162; 9.26 per 103 person-years) with a significant incidence rate ratio of 1.64 (95% confidence interval: 1.61–1.68). The adjusted hazard ratio for CHD in fibromyalgia patients relative to reference subjects was 1.47 (1.43–1.51), after adjusting for age, gender, occupation, monthly income, traditional cardiovascular comorbidities, depression and anxiety. We noted that fibromyalgia and cardiovascular comorbidities had a significant interaction effect on CHD risk (p for interaction <0.01), which was markedly enhanced in fibromyalgia patients with concomitant comorbidities relative to patients with primary fibromyalgia and reference subjects (no fibromyalgia, no comorbidity).
Conclusions
Our report shows that fibromyalgia patients have an independent risk for CHD development. Fibromyalgia patients with concomitant comorbidities have markedly increased CHD risk relative to those with primary fibromyalgia.
Introduction
Fibromyalgia is a syndrome with a broad spectrum of symptoms, including chronic widespread pain, non-restorative sleep, overwhelming fatigue, emotional swings, and cognitive dysfunction, with impaired daily social function and life quality [1]. This syndrome involves pain patterns described as hyperalgesia and allodynia, but evidence is still insufficient to support fibromyalgia as an inflammatory or neuropathic disease [2].
The worldwide prevalence of fibromyalgia, according to classification criteria of the American College of Rheumatology (ACR) [3, 4], is ~2–4% of the population [5, 6], with lower prevalence in Asia [7, 8]. Although its prevalence increases with age, fibromyalgia may occur in children [9, 10]. Women are 3 to 7 times more commonly diagnosed with fibromyalgia than men [10]. On the other hand, the recent population-based studies using the modified 2010 classification criteria of American College of Rheumatology [11] reported a higher prevalence (~5–7%) of fibromyalgia [12, 13]. In general rheumatologic clinics, fibromyalgia is second to osteoarthritis as the most common condition [14].
Fibromyalgia commonly presents with comorbidity such as psychiatric diseases (major depressive disorder, anxiety disorder), headache, irritable bowel syndrome, and interstitial cystitis [15–17]. However, fibromyalgia has seldom been associated with coronary heart disease (CHD). An association between fibromyalgia and CHD with subclinical left ventricular dysfunction has been reported in older, female Korean patients [18]. Similarly, Israeli patients who had received coronary catheterization had significantly greater tenderness and higher scores on the fibromyalgia impact questionnaire [19]. The present nationwide population-based cohort study in Taiwan was undertaken to evaluate if there is an independent risk of CHD in patients with fibromyalgia including those with fibromyalgia only and those with concomitant comorbidities.
Materials and Methods
Data source
For this population-based cohort study, our main data source was the National Health Insurance Research Database (NHIRD) in Taiwan (S1 Text). This database contains information from registration and reimbursement claims to the National Health Insurance (NHI), started in 1995 and covering over 99% of Taiwan’s population. The informed consent of each individual was not obtained. Therefore, scrambling identification numbers of patients before NHIRD compilation was to protect patient privacy. We obtained a database containing medical reimbursement claims from 1996 to 2011 for 1 million people randomly selected from the NHIRD to represent the whole population. This database was released by the NHI as the Longitudinal Health Insurance Database (LHID) [20]. The age and sex of patients in the LHID and full NHIRD did not differ significantly, and the accuracy and validity of diagnoses in the NHIRD have been confirmed [20, 21]. The ethical review board of the China Medical University in Taiwan (CMU-REC-101-012) approved this study (S2 Text).
Criteria for selecting subjects
Diseases of interest were coded using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Disease coding is strictly regulated by the NHI to prevent medical fraud by overbilling for health care or inappropriate charges based on unconfirmed diagnoses. Thus, the NHI regularly monitors coding and claims submitted for reimbursement by all NHI beneficiaries. These precautions for coding errors, misdiagnosis or inappropriate treatment support the reliability of using NHIRD information to explore the risk of CHD in fibromyalgia patients. Among patients in the LHID, 61,711 incident fibromyalgia (ICD-9-CM 729.0–729.1) cases were identified during the study period (2000–2003).
Each patient’s fibromyalgia diagnosis date was defined as its entry date in the LHID. All subjects were followed-up from the entry date until censored, withdrawal from the database, or 31 December 2011. Patients were excluded from the study (n = 99), if they had missing data on age or gender and were diagnosed with CHD before fibromyalgia diagnosis. After these 99 patients were excluded, 61,612 patients with fibromyalgia remained and were ascribed to the case cohort. These patients were matched at baseline by age, gender, and diagnosis date of fibromyalgia in a 1:3 ratio with a reference cohort of non-fibromyalgia subjects in the LHID (n = 184,834; only two non-fibromyalgia reference subject did not qualify for matching criteria).
Outcome and relevant variables
The primary outcome was the event of CHD with acute coronary syndrome, including clinical conditions of angina pectoris, ischemic heart disease, and coronary atherosclerosis (ICD-9-CM 411.1, 413, 414.0, 414.8, 414.9) during the study period (2000–2011). Relevant variables were age, gender and comorbidities, including type II diabetes mellitus (ICD-9-CM 250), hypertension (ICD-9-CM 401–405), hyperlipidemia (ICD-9-CM 272), congestive heart failure with or without renal disease (ICD-9-CM 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, 428.0), cerebral vascular diseases (ICD-9-CM 430–438), depression (ICD-9-CM 296.2–296.3, 300.4, 311), and anxiety (ICD-9-CM 300.0, 300.2, 300.3, 308.3, 308.91). All comorbidities were defined before the index date of diagnosis.
Statistical analysis
Differences in demographic characteristics and comorbidities between the case cohort of fibromyalgia patients and the reference cohort were tested by chi-square test for categorical variables or Student’s t-test for continuous variables. The gender-, age- and comorbidity-specific incidence rates (per 103 person-years) of CHD between the case and reference cohorts were compared. Person-years were calculated from the entry dates to the censored dates of CHD occurrence, withdrawal from follow-up, or the end of 2011. Incidence rate ratios (IRRs) and 95% confidence intervals (95% CIs) of CHD in fibromyalgia patients relative to reference subjects were estimated using the Poisson regression model. Multivariate adjusted hazard ratios (HRs) and 95% CIs of CHD in fibromyalgia patients relative to the reference subjects were derived by Cox proportional hazard models after adjusting for age, gender, occupation status, monthly income level, and comorbidities. We further compared the risk of CHD development in patients with fibromyalgia by stratification with respect to (1) gender, (2) age, and (3) comorbidities. Age subgroups were stratified into < 35 years, 35–65 years and > 65 years. Differences in the CHD incidence of cohorts, plotted as Kaplan-Meier survival curves, were tested by log-rank test. A p value < 0.05 was considered significant in two-tailed tests. All calculations were performed using SAS version 9.1 (SAS Institute Inc., Cary, NC).
Results
From the LHID, we identified 61,612 fibromyalgia patients as the case cohort and 184,834 matched subjects without fibromyalgia as the reference cohort (1:3 match ratio), with a mean 8.86 ± 2.68 years (2,184,197 person-years in total) of follow-up. The standardized prevalence and incidence of fibromyalgia were 5.84 (95% CI 4.52–7.55) % and 20.2 (95% CI 13.1–31.6) per 103 person-years, respectively, with respect to the Taiwanese population in 2000 [22]; the standardized fibromyalgia prevalence and incidence were 5.56 (95% CI 4.27–7.23) % and 19.2 (95% CI 12.2–30.0) per 103 person-years, respectively, with respect to the World Health Organization population in 2000 [23]. Fig 1 shows the incidence of fibromyalgia in patients of both genders (per 103 person-years) with respect to age (stratified by 5 years of age). The mean age of the fibromyalgia cohort was 44.1 ± 16.5 years old, with a female-to-male ratio of 6-to-4 (59.3% versus 40.7%). The highest proportion of fibromyalgia patients was in the 35–65 year-old age subgroup (57.8%). Higher proportions of fibromyalgia patients had a blue-collar status and monthly income level of TWD 15,000 to 25,000 than non-fibromyalgia subjects. The case cohort also had a significantly higher prevalence of comorbidities, including diabetes, hypertension, hyperlipidemia, congestive heart failure, cerebral vascular diseases, depression, and anxiety than the reference cohort (Table 1).
Fig 1. The incidence of fibromyalgia (103 person-years) between women and men stratified by age subgroups.
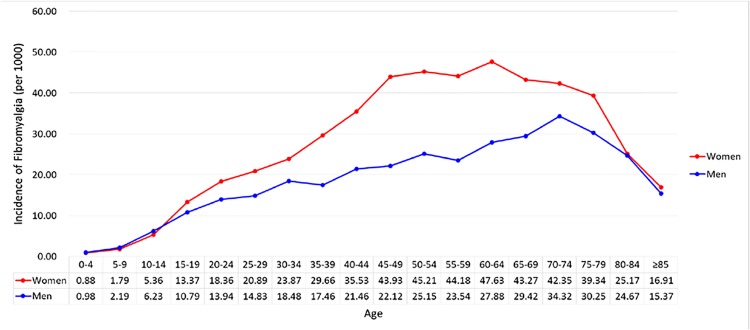
Table 1. Comparison of demographics and comorbidities between the fibromyalgia and non-fibromyalgia cohorts.
| Fibromyalgi | Referenc | p | |||
|---|---|---|---|---|---|
| n = 61612 | n = 184834 | ||||
| n | % | n | % | ||
| Gender | 0.99 | ||||
| Women | 36,546 | 59.3 | 109,638 | 59.3 | |
| Men | 25,066 | 40.7 | 75,196 | 40.7 | |
| Age, year | 0.99 | ||||
| <35 | 18,456 | 30.0 | 55,368 | 30.0 | |
| 35–65 | 35,626 | 57.8 | 106,878 | 57.8 | |
| >65 | 7,530 | 12.2 | 22,588 | 12.2 | |
| Mean (SD) # | 44.1 (16.5) | 44.0 (16.5) | 0.35 | ||
| Occupation | < .0001 | ||||
| White collar | 31,607 | 51.3 | 100,759 | 54.5 | |
| Blue collar | 24,913 | 40.4 | 67,541 | 36.5 | |
| Other | 5,092 | 8.26 | 16,534 | 8.95 | |
| Monthly income (TWD) | < .0001 | ||||
| <15,000 | 14,029 | 22.8 | 46,873 | 25.4 | |
| 15,000–25,000 | 35,197 | 57.1 | 99,408 | 53.8 | |
| >25,000 | 12,386 | 20.1 | 38,553 | 20.9 | |
| Comorbidity | |||||
| Diabetes | 5,694 | 9.24 | 12,690 | 6.87 | < .0001 |
| Hypertension | 13,112 | 21.3 | 29,788 | 16.1 | < .0001 |
| Hyperlipidaemia | 9,091 | 14.8 | 16,439 | 8.89 | < .0001 |
| Congestive heart failure | 693 | 1.12 | 1,684 | 0.91 | < .0001 |
| Cerebral vascular diseases | 4,817 | 7.82 | 9,704 | 5.25 | < .0001 |
| Depression | 2,067 | 3.35 | 3,077 | 1.66 | < .0001 |
| Anxiety | 4,489 | 7.29 | 5,492 | 2.97 | < .0001 |
TWD, Taiwanese dollar
Chi-square test
# Student’s t-test
White collar: civil services, institutional workers, enterprise, business and industrial administration personnel; Blue collar: farmers, fishermen, vendors, and industrial laborers; Other: retired, unemployed, and low-income populations
Fig 2 shows the cumulative incidence rates of CHD in the case and reference cohorts during 12 years of follow-up (log-rank test, p < 0.01). In these cohorts, 8,280 fibromyalgia patients (15.2 per 103 person-years) and 15,162 reference subjects (9.26 per 103 person-years) developed CHD, with fibromyalgia patients having a significant incidence rate ratio (IRR) of 1.64 (95% CI 1.61–1.68) and HR of 1.47 (95% CI 1.43–1.51) relative to the reference subjects, after adjusting for age, gender, occupation, monthly income, comorbidities of traditional cardiovascular risk factors, depression, and anxiety (Table 2).
Fig 2. Cumulative incidence of coronary heart diseases between the fibromyalgia cohort (dashed line) and non-fibromyalgia cohort (solid line).

Table 2. Incidence and adjusted hazard ratio for coronary heart disease stratified by gender, age, occupation, monthly income, and comorbidity status for patients with fibromyalgia and compared to those without fibromyalgia.
| Fibromyalgia | Reference | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | Event | PY | Rate | Event | PY | Rate | IRR | Adjusted HR † |
| (95% CI) | (95% CI) | |||||||
| All | 8,280 | 544,629 | 15.2 | 15,162 | 1,638,194 | 9.26 | 1.64(1.61–1.68)* | 1.47(1.43–1.51)* |
| Gender | ||||||||
| Female | 4,796 | 326,677 | 14.7 | 8,641 | 986,356 | 8.76 | 1.68(1.63–1.72)* | 1.50(1.45–1.55)* |
| Male | 3,484 | 217,952 | 16.0 | 6,521 | 651,838 | 10.0 | 1.60(1.54–1.65)* | 1.44(1.38–1.50)* |
| Age, years | ||||||||
| < 35 | 342 | 177,075 | 1.93 | 355 | 517,114 | 0.69 | 2.81(2.68–2.95)* | 2.40(2.06–2.79)* |
| 35–64 | 5,360 | 317,450 | 16.9 | 9,501 | 969,430 | 9.80 | 1.72(1.68–1.77)* | 1.45(1.40–1.50)* |
| > 65 | 2,578 | 50,104 | 51.5 | 5,306 | 151,650 | 35.0 | 1.47(1.39–1.55)* | 1.36(1.30–1.43)* |
| Occupation | ||||||||
| White collar | 3,496 | 285,382 | 12.25 | 6,904 | 908,254 | 7.60 | 1.61(1.56–1.66)* | 1.48(1.42–1.55)* |
| Blue collar | 3,948 | 216,622 | 18.23 | 6,781 | 590,683 | 11.48 | 1.59(1.53–1.64)* | 1.45(1.39–1.51)* |
| Other | 836 | 42,625 | 19.61 | 1,477 | 139,256 | 10.61 | 1.85(1.72–1.99)* | 1.54(1.41–1.68)* |
| Monthly income, TWD | ||||||||
| < 15,000 | 1,915 | 120,088 | 15.95 | 3,880 | 400,599 | 9.69 | 1.65(1.57–1.72)* | 1.49(1.41–1.57)* |
| 15,000–-25,000 | 4,832 | 311,949 | 15.49 | 8,339 | 882,458 | 9.45 | 1.64(1.59–1.69)* | 1.48(1.43–1.53)* |
| >25,000 | 1,533 | 112,592 | 13.62 | 2,943 | 355,137 | 8.29 | 1.64(1.57–1.72)* | 1.43(1.35–1.53)* |
| Comorbidity | ||||||||
| No | 2,323 | 365,924 | 6.35 | 5,399 | 1,280,423 | 4.22 | 1.51(1.46–1.55)* | 1.68(1.60–1.76)* |
| Yes | 5,957 | 178,704 | 33.3 | 9,763 | 357,770 | 27.3 | 1.22(1.18–1.27)* | 1.34(1.30–1.39)* |
PY, person-years; Rate, incidence rate (per 1,000 person-years); IRR, incidence rate ratio; HR, hazard ratio
† Adjusted HR: multiple analysis after adjusting for age, gender, occupation, monthly income, and comorbidities
*p<0.001
Although women were more likely to have fibromyalgia early in life compared with men (Fig 1), both genders of fibromyalgia patients had comparable risks for developing CHD. The incidence rates increased with age in both cohorts (Table 2); however, it is noteworthy that the highest age-specific CHD risk in fibromyalgia patients was in the youngest subgroup (age < 35 years: adjusted HR [aHR] 2.40, 95% CI 2.06–2.79), with steadily declining estimates as age increased. Finally, our analysis showed that CHD risks in fibromyalgia patients relative to non-fibromyalgia reference subjects were comparable across different occupation statuses and monthly income levels.
The impact of comorbidities on outcomes for fibromyalgia patients was assessed by stratifying the case and reference cohorts with respect to comorbidity status. CHD risks were significant in both fibromyalgia patients with (aHR 1.34, 95% CI 1.30–1.39) and without (aHR 1.68, 95% CI 1.60–1.76) comorbidities relative to their respective matched reference subjects (Table 2). We further stratified fibromyalgia patients and reference subjects with respect to comorbidity status (Table 3). In fibromyalgia patients without and with comorbidities, the aHRs for CHD ranged from 1.60–1.76 and 1.30–1.39, respectively; the HRs were significantly greater than those of their respective reference subjects.
Table 3. Incidence and adjusted hazard ratio for coronary heart diseases stratified by comorbidity for the fibromyalgia cohort and compared with the non-fibromyalgia cohort.
| Fibromyalgia | Reference | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | Event | PY | Rate | Event | PY | Rate | IRR (95% CI) | Adjusted HR † (95% CI) |
| Diabetes | ||||||||
| No | 6,457 | 502,818 | 12.8 | 11,945 | 1,545,637 | 7.73 | 1.66(1.62–1.70)** | 1.51(1.46–1.56)** |
| Yes | 1,823 | 41,810 | 43.6 | 3,217 | 92,556 | 34.8 | 1.25(1.17–1.34)** | 1.29(1.22–1.37)** |
| Hypertension | ||||||||
| No | 3,898 | 449,503 | 8.67 | 7,561 | 1,419,868 | 5.33 | 1.63(1.59–1.67)** | 1.59(1.53–1.66)** |
| Yes | 4,382 | 95,125 | 46.1 | 7,601 | 218,326 | 34.8 | 1.32(1.27–1.38)** | 1.34(1.29–1.39)** |
| Hyperlipidemia | ||||||||
| No | 5,587 | 473,821 | 11.8 | 11,315 | 1,509,897 | 7.49 | 1.57(1.54–1.61)** | 1.50(1.45–1.55)** |
| Yes | 2,693 | 70,808 | 38.0 | 3,847 | 128,297 | 30.0 | 1.27(1.20–1.34)** | 1.35(1.29–1.42)** |
| Congestive heart failure | ||||||||
| No | 7,982 | 540,580 | 14.8 | 14,615 | 1,629,147 | 8.97 | 1.65(1.61–1.68)** | 1.48(1.44–1.52)** |
| Yes | 298 | 4,049 | 73.6 | 547 | 9,047 | 60.5 | 1.22(1.02–1.46)* | 1.25(1.08–1.44)* |
| Cerebral vascular diseases | ||||||||
| No | 6,812 | 509,627 | 13.4 | 12,994 | 1,572,683 | 8.26 | 1.62(1.58–1.66)** | 1.47(1.43–1.52)** |
| Yes | 1,468 | 35,002 | 41.9 | 2,168 | 65,511 | 33.1 | 1.27(1.17–1.37)** | 1.40(1.31–1.50)** |
| Depression | ||||||||
| No | 7,872 | 527,718 | 14.9 | 14,754 | 1,613,888 | 9.14 | 1.63(1.60–1.67)** | 1.46(1.42–1.50)** |
| Yes | 408 | 16,911 | 24.1 | 408 | 24,305 | 16.8 | 1.44(1.25–1.65)** | 1.67(1.45–1.90)** |
| Anxiety | ||||||||
| No | 7,294 | 508,421 | 14.35 | 14,162 | 1,595,256 | 8.88 | 1.62(1.58–1.65)** | 1.47(1.43–1.51)** |
| Yes | 986 | 36,208 | 27.23 | 882 | 44,312 | 19.9 | 1.37(1.24–1.51)** | 1.57(1.43–1.72)** |
PY, person-year; Rate, incidence rate (per 1,000 person-years); IRR, incidence rate ratio; HR, hazard ratio
†Adjusted HR: multiple analysis after adjusting for age, gender, occupation, income and comorbidities
*p<0.05
**p<0.001
The joint effect on CHD risk and interaction between fibromyalgia and the respective comorbidity are shown in Fig 3. Relative to reference subjects without fibromyalgia and comorbidities, fibromyalgia patients without respective comorbidity of diabetes, hypertension, hyperlipidemia or congestive heart failure had aHRs for CHD ranging from 1.66–1.72, which were generally lower than the respective risk ranging from 2.16–2.75 in non-fibromyalgia patients but with these traditional cardiovascular comorbidities (p for interaction < 0.01, respectively). It is noteworthy that relative to reference subjects of no depression, no fibromyalgia, the CHD risk in patients with fibromyalgia but without depression (aHR 1.65, 95% CI 1.61–1.70) was higher than that in patients with depression but without fibromyalgia (aHR 1.21, 95% CI 1.10–1.34). However, the CHD risks between patients with fibromyalgia but without anxiety and patients with anxiety but without fibromyalgia were comparable. The effect of combing fibromyalgia with comorbidity of either diabetes, hypertension, hyperlipidemia, congestive heart failure, cerebral vascular diseases, depression or anxiety was associated with significantly higher CHD risk than that in patients with fibromyalgia only and that in those with respective comorbidity.
Fig 3. Adjusted hazard ratios for coronary heart diseases associated with the fibromyalgia-comorbidity interaction.

The first line indicates patients with the respective comorbidity. The second and red line indicates patients with primary fibromyalgia, and the third line indicates fibromyalgia patients with the respective concomitant comorbidity. *p for interaction < 0.01.
Discussion
The present study confirmed that fibromyalgia patients had a 47% increased risk of CHD after adjusting for age, gender, occupation, monthly income, and comorbidities. Although the impact of fibromyalgia on developing CHD was moderate, the risk was not as high as that for traditional cardiovascular risk factors of diabetes, hypertension, hyperlipidemia or congestive heart failure. A greater CHD risk was noted in fibromyalgia patients with concomitant comorbidities than in patients with primary fibromyalgia or in reference patients with the respective comorbidity alone.
Several limitations were noted in this study. First, fibromyalgia patients may have been misclassified in the LHID population, because patients in the case cohort with a clinical diagnosis of fibromyalgia defined by the physicians did not necessarily meet the classification criteria of American College of Rheumatology [3, 4]. However, this current study demonstrated a higher standardized prevalence rate and a greater male-to-female ratio in Taiwanese fibromyalgia patients, which findings were similar to the reports in the United States (6.4%) [13], Germany (5.4%) [12] and Nantou County, Taiwan (6.7%) [24] using the modified 2010 classification criteria of American College of Rheumatology to survey for the general population [11]. The new criteria integrates the widespread pain index and self-reported specific symptoms may facilitate epidemiological investigations and should help to identify more male and younger patients [25].
Second, the criteria to diagnose fibromyalgia include depression. A population-based study in the United Kingdom reported 16.7% of patients with chronic widespread pain (classified using ACR criteria for fibromyalgia) had mental disorders [26]. A risk of CHD was recently reported in patients with depressive disorder [27], and CHD has been associated with subsequent depression [28]. In this study, we showed an increased risk of CHD in individuals with depression, which is compatible with previous report [27]. We also found the adjusted HR for CHD in patients with primary fibromyalgia (aHR 1.65) was significantly higher than that in depressed patients without fibromyalgia (aHR 1.21) and the risk of CHD between patients with fibromyalgia and those with anxiety was comparable (aHR 1.63 versus 1.52). However, the differentiating among anxiety, depressive mood and major depression disorder in fibromyalgia patients can be vague, and we need to interpret the results with caution.
Third, the LHID does not provide parameters, including pain scores, laboratory data on inflammatory index, metabolic profiles, body mass index, and personal habits such as cigarette smoking and alcohol drinking. Therefore, we could not correlate body mass index and degree of pain [29] or assess the impact of smoking [30], which are known risk factors for fibromyalgia or CHD. However, Taiwanese women have a very low smoking rate (4.3%) compared with that in men (46.8%) [31]; it is worth noting that females and young children can be exposed to high environmental tobacco exposure due to second hand smoking [32]. Nonetheless, the impact of second hand smoking on the development of fibromyalgia, as we considered, should be far less than that on the development of CHD. Even though there is a risk of CHD due to second hand smoking, the evidenced risk of fibromyalgia resulting from second hand smoking so far is limited. Therefore, we assumed the bias that fibromyalgia patients might have CHD due to second hand smoking can be non-differential and this bias is not likely to confound fibromyalgia risk in female patients.
Fourth, patients with fibromyalgia may show an increased health-care-seeking behavior, which can explain our results that patients with fibromyalgia had significantly higher prevalence of comorbidities than the reference cohort, and may have impacted the CHD risk. Nevertheless, the independent risk of fibromyalgia for CHD was confirmed by sequential stratifications by comorbidity in both patients and reference subjects, and CHD risk persisted in fibromyalgia patients without comorbidities and was higher in younger patients.
Fifth, one could argue that CHD risk in fibromyalgia patients can be potentiated by chronic use of anti-depressants and painkillers, including non-steroidal anti-inflammatory drugs (NSAIDs) and cyclooxygenase-2 inhibitors (coxibs), which have been suggested to enhance cardiovascular risk. However, a population-based study showed that the rate of cardiovascular events was significantly higher for patients who took rofecoxib (RR 1.15) and was also significantly lower for those who took naproxen (RR 0.75) compared with the reference patients who did not use NSAIDs or coxibs [33]. Moreover, as indicated in a population-based cohort study [27] that CHD risk of depressed patients was not increased by antidepressants, which are commonly used in fibromyalgia treatment. Although we were unable to put all these treatment into modeling, these reports may suggest that painkillers and antidepressants did not lead to important modifications in patients’ cardiovascular risk [33]. People can still argue that other treatment modality or residual confounding factors can exit. For instance, although acupuncture has been used to treat pain and fibromyalgia [34–36], it has no reported risk to CHD. Whether traditional Chinese herbs can be used to deal with fibromyalgia and whether they might increase the risk of CHD are undetermined [37]. In light of the huge national insurance data and large sample size, these confounders may become non-differential bias and the evidences demonstrated above may strengthen the contention that fibromyalgia can be an independent risk factor for CHD.
Several lines of evidence can provide a possible biological explanation to support the increased CHD risk in fibromyalgia patients. First, people with chronic widespread pain have been shown in population-based studies to have greater psychological distress and mental disorders than those without pain [26, 38, 39]. Previous reports indicated that people with chronic diseases, such as fibromyalgia and CHD, have a common life experience of childhood abuse, from a perspective of mind-body medicine [40]. The potential role of early psychosocial adversities in the vulnerability of fibromyalgia and CHD should be considered and appropriate referral may be needed for follow-up counseling [41]. Second, fibromyalgia was previously shown to be significantly associated with degree of stress [24], and chronic stress contributes to persistent activation of the sympathetic nervous system and hypothalamic-pituitary-adrenal axis [42]. The autonomic dysfunction in patients with fibromyalgia is characterized by stronger parasympathetic decline [43] and maintains patients in a state of sympathetic hyperactivity [44]. Indeed, evidence showed that fibromyalgia patients with exaggerated sympathetic modulation of the sinus node and enhanced heart rate variability [45, 46] may incur the risk of CHD.
The strengths of this study warrant mention. First, the study data source, Taiwan’s NHIRD enrolls over 22 million citizens and employees in a national insurance program. The stringent NHI surveillance program, which rigorously monitors and audits insurance reimbursement claims to prevent healthcare fraud, strengthens the reliability of diagnoses based on insurance claims. Second, the characteristics of our fibromyalgia patients were consistent with previous reports of female predominance and the majority being middle-aged [5–8, 10, 24]. The similarity of these characteristics supports the validity of identifying fibromyalgia patients from the LHID and of generalizing and applying our results on a representative sample of Taiwan’s general population to other populations. Third, a recent Taiwanese cohort study reported a two-fold increased risk of CHD in fibromyalgia patients relative to the reference subjects [47]. However, the reported risk of chronic pain was unexpectedly exceeding that of traditional risk factors. Our study using the large sample for subgroup analysis ascertained the impact of fibromyalgia on CHD. Moreover, a markedly enhanced risk of CHD was evidenced by the synergistic effect of fibromyalgia with each individual comorbidity, in correspondence with previous report (47). Fourth, the adequate study power and the long patient observation period raised the potential for fibromyalgia to predispose patients to develop CHD.
In conclusion, our study finds that fibromyalgia is an independent risk for CHD development. However, the risk of primary fibromyalgia is not as high as the traditional cardiovascular risk, but its impact on CHD is significantly higher than that of depression. A noteworthy finding is the markedly enhanced risk of CHD in fibromyalgia patients with concomitant comorbidities.
Supporting Information
(DOCX)
(DOCX)
Acknowledgments
The authors thank the National Health Research Institute in Taiwan for making available insurance claims data for analyses.
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
This study was funded, in part, by the Department of Health, Executive Yuan, Taiwan (Grant DOH 97-HP-1101, 2008, Grant NSC97-2314-B-039-010-MY3, Grant NSC100-2314-B-039-012, Grant NSC101-2314-B-039-020, Grant MOST103-2314-B-039-020); China Medical University Hospital (Grant 1MS1, Grant DMR-97-059, Grant DMR-101-010, Grant DMR-102-012); Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (Grant MOHW104-TDU-B-212-113002); Academia Sinica Taiwan Biobank, Stroke Biosignature Project (Grant BM104010092); NRPB Stroke Clinical Trial Consortium (MOST 103-2325-B-039 -006); Tseng-Lien Lin Foundation, Taichung, Taiwan; Taiwan Brain Disease Foundation, Taipei, Taiwan; and Katsuzo and Kiyo Aoshima Memorial Fund. None of the funders played a role in conducting the research.
References
- 1. Wolfe F, Ross K, Anderson J, Russell IJ, Hebert L. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheum 1995;38:19–28. [DOI] [PubMed] [Google Scholar]
- 2. Staud R, Rodriguez ME. Mechanisms of disease: pain in fibromyalgia syndrome. Nat Clin Pract Rheumatol 2006;2:90–898. [DOI] [PubMed] [Google Scholar]
- 3. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum 1990;33:160–72. [DOI] [PubMed] [Google Scholar]
- 4. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res (Hoboken) 2010;62:600–10. [DOI] [PubMed] [Google Scholar]
- 5. White KP, Speechley M, Harth M, Ostbye T. The London fibromyalgia epidemiology study: the prevalence of fibromyalgia syndrome in London, Ontario. J Rheumatol. 1999;26:1570–1576. [PubMed] [Google Scholar]
- 6. Wolfe F, Ross K, Anderson J, Russell IJ, Hebert L. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheum. 1995;38:19–28. [DOI] [PubMed] [Google Scholar]
- 7. Toda K. The prevalence of fibromyalgia in Japanese workers. Scand J Rheumatol 2007;36:140–4. [DOI] [PubMed] [Google Scholar]
- 8. Kim C, Kim H, Kim J. Prevalence of chronic widespread pain and fibromyalgia syndrome: a Korean hospital-based study. Rheumatology Int 2012;32:3435–42. [DOI] [PubMed] [Google Scholar]
- 9. Buskila D, Atzeni F, Sarzi-Puttini P. Etiology of fibromyalgia: the possible role of infection and vaccination. Autoimmunity Rew 2008;8:41–43. [DOI] [PubMed] [Google Scholar]
- 10. Clark P, Burgos-Vargas R, Medina-Palma C, Lavielle P, Marina FF. Prevalence of fibromyalgia in children: a clinical study of Mexican children. J Rheumatol 1998;25:2009–2014. [PubMed] [Google Scholar]
- 11. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Hauser W, Katz RS, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J Rheumatol 2011;38:1113–1122. 10.3899/jrheum.100594 [DOI] [PubMed] [Google Scholar]
- 12. Jones GT, Atzeni F, Beasley M, Fluss E, Sarzi-Puttini P, Macfarlane GJ. The prevalence of fibromyalgia in the general population: a comparison of the american college of rheumatology 1990, 2010, and modified 2010 classification criteria. Arthritis Rheum 2015;67:568–575. [DOI] [PubMed] [Google Scholar]
- 13. Vincent A, Lahr BD, Wolfe F, Clauw DJ, Whipple MO, Oh TH, et al. Prevalence of fibromyalgia: a population-based study in Olmsted County, Minnesota, utilizing the Rochester Epidemiology Project. Arthritis Care Res (Hoboken) 2013;65:786–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Clauw DJ, Arnold LM, McCarberg BH, FibroCollaborative. The science of fibromyalgia. Mayo Clin Proc 2011;86:907–11. 10.4065/mcp.2011.0206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kim SC, Landon JE, Solomon DH. Clinical characteristics and medication uses among fibromyalgia patients newly prescribed amitriptyline, duloxetine, gabapentin, or pregabalin. Arthritis Care Res (Hoboken) 2013;65:1813–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Rehm SE, Koroschetz J, Gockel U, Brosz M, Freynhagen R, Tolle TR, et al. A cross-sectional survey of 3035 patients with fibromyalgia: subgroups of patients with typical comorbidities and sensory symptom profiles. Rheumatology (Oxford) 2010;49:1146–52. [DOI] [PubMed] [Google Scholar]
- 17. Tietjen GE, Herial NA, Hardgrove J, Utley C, White L. Migraine comorbidity constellations. Headache. 2007;47:857–865. [DOI] [PubMed] [Google Scholar]
- 18. Cho KI, Lee JH, Lee HG, Kim SM, Kim TI. Assessment of myocardial function in patients with fibromyalgia and the relationship to chronic emotional and physical stress. Korean Circ J 2010;40:74–80. 10.4070/kcj.2010.40.2.74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ablin JN, Beilinson N, Aloush V, Elkayam O, Finkelstein A. Association between fibromyalgia and coronary heart disease and coronary catheterization. Clin Cardiol 2009;32:E7–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Kang JH, Chen YH, Lin HC. Comorbidity profiles among patients with ankylosing spondylitis: a nationwide population-based study. Ann Rheum Dis 2010;69:1165–1168. 10.1136/ard.2009.116178 [DOI] [PubMed] [Google Scholar]
- 21. Cheng CL, Kao YH, Lin SJ, Lee CH, Lai ML. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol Drug Saf 2011;20:236–42. 10.1002/pds.2087 [DOI] [PubMed] [Google Scholar]
- 22. Lee CT, Chen VC, Tan HK, Chou SY, Wu KH, Chan CH, et al. Suicide and other-cause mortality among heroin users in Taiwan: a prospective study. Addict Behav 2013;38:2619–23. 10.1016/j.addbeh.2013.03.003 [DOI] [PubMed] [Google Scholar]
- 23. Chen YJ, Chang YT, Wang CB, Wu CY. The risk of cancer in patients with rheumatoid arthritis: a nationwide cohort study in Taiwan. Arthritis Rheum 2011;63:352–8. 10.1002/art.30134 [DOI] [PubMed] [Google Scholar]
- 24. Chen JH, Guo M, You Y, Liaw L, Kuo H. Factors affecting Fibromyalgia in Nantou County. Mid-Taiwan Journal of Medicine. 2008;13:136–142. [Google Scholar]
- 25. McBeth J, Mulvey MR. Fibromyalgia: mechanisms and potential impact of the ACR 2010 classification criteria. Nat Rev Rheumatol 2012;8:108–16. 10.1038/nrrheum.2011.216 [DOI] [PubMed] [Google Scholar]
- 26. Benjamin S, Morris S, McBeth J, Macfarlane GJ, Silman AJ. The association between chronic widespread pain and mental disorder: a population-based study. Arthritis Rheum 2000;43:561–7. [DOI] [PubMed] [Google Scholar]
- 27. Huang CJ, Hsieh MH, Hou WH, Liu JC, Jeng C, Tsai PS. Depression, antidepressants, and the risk of coronary heart disease: a population-based cohort study. Int J Cardiol 2013;168:4711–6. 10.1016/j.ijcard.2013.07.173 [DOI] [PubMed] [Google Scholar]
- 28. Frasure-Smith N, Lesperance F, Talajic M. Depression following myocardial infarction. Impact on 6-month survival. JAMA 1993;270:1819–1825. [PubMed] [Google Scholar]
- 29. Horvei LD, Braekkan SK, Mathiesen EB, Njolstad I, Wilsgaard T, Hansen JB. Obesity measures and risk of venous thromboembolism and myocardial infarction. Eur J Epidemiol 2014;29:821–30. 10.1007/s10654-014-9950-z [DOI] [PubMed] [Google Scholar]
- 30. Golomb BA, Chan VT, Denenberg JO, Koperski S, Criqui MH. Risk marker associations with venous thrombotic events: a cross-sectional analysis. BMJ Open. 2014;4:e003208 10.1136/bmjopen-2013-003208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bureau of Health Promotion T. Taiwan Tobacco Control Annual Report 2012. Taipei: Department of Health, Taiwan. 2012.
- 32. Wen CP, Levy DT, Cheng TY, Hsu CC, Tsai SP. Smoking behaviour in Taiwan, 2001. Tob Control. 2005;14 Suppl 1:i51–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Solomon DH, Avorn J, Sturmer T, Glynn RJ, Mogun H, Schneeweiss S. Cardiovascular outcomes in new users of coxibs and nonsteroidal antiinflammatory drugs: high-risk subgroups and time course of risk. Arthritis Rheum 2006;54:1378–89. [DOI] [PubMed] [Google Scholar]
- 34. Deluze C, Bosia L, Zirbs A, Chantraine A, Vischer TL. Electroacupuncture in fibromyalgia: results of a controlled trial. BMJ 1992;305:1249–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Iannuccelli C, Mannocci F, Guzzo MP, Olivieri M, Gerardi MC, Atzeni F, et al. Complementary treatment in fibromyalgia: combination of somatic and abdominal acupuncture. Clin Exp Rheumatol 2012;30(Suppl 74):112–6. [PubMed] [Google Scholar]
- 36. Cao H, Li X, Han M, Liu J. Acupoint stimulation for fibromyalgia: a systematic review of randomized controlled trials. Evid Based Complement Alternat Med 2013:362831 10.1155/2013/362831 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Ding F, Zhang Q, Ung CO, Wang Y, Han Y, Hu Y, et al. An analysis of chemical ingredients network of Chinese herbal formulae for the treatment of coronary heart disease. PloS One. 2015;10:e0116441 10.1371/journal.pone.0116441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Krishnan KR, France RD, Pelton S, McCann UD, Davidson J, Urban BJ. Chronic pain and depression. II. Symptoms of anxiety in chronic low back pain patients and their relationship to subtypes of depression. Pain. 1985;22:289–94. [DOI] [PubMed] [Google Scholar]
- 39. Makela M, Heliovaara M. Prevalence of primary fibromyalgia in the Finnish population. BMJ. 1991;303:216–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Springer KW, Sheridan J, Kuo D, Carnes M. The long-term health outcomes of childhood abuse. An overview and a call to action. J Gen Intern Med 2003;18(10):864–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Imbierowicz K, Egle UT. Childhood adversities in patients with fibromyalgia and somatoform pain disorder. Eur J Pain. 2003;7(2):113–9. [DOI] [PubMed] [Google Scholar]
- 42. Vargas-Alarcon G, Fragoso JM, Cruz-Robles D, Vargas A, Vargas A, Lao-Villadoniga JI, et al. Catechol-O-methyltransferase gene haplotypes in Mexican and Spanish patients with fibromyalgia. Arthritis Res Ther 2007;9:R110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Eisenlohr-Moul TA, Crofford LJ, Howard TW, Yepes JF, Carlson CR, de Leeuw R. Parasympathetic reactivity in fibromyalgia and temporomandibular disorder: associations with sleep problems, symptom severity, and functional impairment J Pain. 2015;16:247–57. 10.1016/j.jpain.2014.12.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Martinez-Martinez LA, Mora T, Vargas A, Fuentes-Iniestra M, Martinez-Lavin M. Sympathetic nervous system dysfunction in fibromyalgia, chronic fatigue syndrome, irritable bowel syndrome, and interstitial cystitis: a review of case-control studies. J Clin Rheumatol 2014;20:146–50. 10.1097/RHU.0000000000000089 [DOI] [PubMed] [Google Scholar]
- 45. Martinez-Lavin M, Hermosillo AG, Rosas M, Soto ME. Circadian studies of autonomic nervous balance in patients with fibromyalgia: a heart rate variability analysis. Arthritis Rheum 1998;41:1966–71. [DOI] [PubMed] [Google Scholar]
- 46. Solano C, Martinez A, Becerril L, Vargas A, Figueroa J, Navarro C, et al. Autonomic dysfunction in fibromyalgia assessed by the Composite Autonomic Symptoms Scale (COMPASS). J Clin Rheumatol 2009;15:172–6. 10.1097/RHU.0b013e3181a1083d [DOI] [PubMed] [Google Scholar]
- 47. Tsai PS, Fan YC, Huang CJ. Fibromyalgia is associated with coronary heart disease: a population-based cohort study. Reg Anesth Pain Med 2015;40:37–42. 10.1097/AAP.0000000000000190 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX)
(DOCX)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.