

Abstract
Background: We investigated the use of a simple novel nut and bolt task in premanifest and manifest Huntington’s disease (HD) patients to detect and quantify motor impairments at all stages of the disease.
Methods: Premanifest HD (n=24), manifest HD (n=27) and control (n=32) participants were asked to screw a nut onto a bolt in one direction, using three different sized bolts with their left and right hand in turn.
Results: We identified some impairments at all stages of HD and in the premanifest individuals, deficits in the non-dominant hand correlated with disease burden scores.
Conclusion: This simple, cheap motor task was able to detect motor impairments in both premanifest and manifest HD and as such might be a useful quantifiable measure of motor function for use in clinical studies.
INTRODUCTION
Huntington’s disease (HD) is an autosomal dominant condition causing neurodegeneration of the cortex1 white matter2 , 3 and basal ganglia4 , 5. This leads clinically to motor deficits including chorea, bradykinesia, and dystonia as well as cognitive deficits, circadian rhythm disturbances and psychiatric problems6 , 7. The ability to robustly detect early motor impairments in HD using a simple cheap test is needed to provide an objective quantifiable measure of motor performance that is useful both clinically and as an endpoint in therapeutic trials, and which can be followed over time. Also more tests that measure everyday motor tasks that impact on functional independence as the disease progresses are required. As such, many groups, including our own, have sought to develop motor tasks to detect and track early changes in premanifest HD (preHD)8 , 9 including both the finger8 , 9 and hand tapping tests 10 , 11 , 12 , 13. Motor differences are not just seen in tapping tasks, as other studies have shown that there are changes in the variability of grip force in a grasping task in HD patients 14; a reduction in tongue force in preHD patients 15; a reduction of speech rate in motor speech tasks 16 and impairments in saccade latency and velocity in HD 12 , 17. Furthermore these simple tasks have been correlated to structural brain changes in HD and preHD 18 as well as cognitive deficits 19. Other more complex motor tasks such as those involving diadochokinetic movements 20 and peg insertions, whilst able to detect impairments in manifest disease are insensitive during preHD 21. Many of these tasks described require specialized equipment and complicated analysis. In this paper we have assessed participants with manifest HD and preHD using a very simple and cheap nut and bolt test which has previously been used to look at the effects of extravehicular activity (EVA) gloves on dexterity, grip force and coordination in healthy participants 22. This new test is ideal for use in HD given its ecological validity, its ease of administration and the fact that it is so inexpensive; this makes it accessible for use in any population of HD patients and it doesn’t require any specialised custom computer software to interpret the results collected. To examine the validity of this new motor task, we tested a large group of individuals at pre-manifest and manifest stages of HD compared to healthy controls. Finally, we examined whether performance on this timed nut and bolt test was related to disease burden score (DBS). We now report for the first time that this simple inexpensive test can detect the earliest motor abnormalities in HD and performance correlates with disease burden scores across the entire disease, and so could be used to target those patients on the cusp of developing overt disease and as such may be suitable for use in new trials of disease modifying therapy.
METHODS
Participants
Participants were recruited from the regional NHS HD clinic at the John Van Geest Centre for Brain Repair between 2012 and 2014. Control subjects with no known neurological disease were recruited from friends or relatives accompanying patients to the clinic. Written informed consent was taken and the nut and bolt data was collected under ethical approval [Reference number:09/H0308/2] approved by Cambridgeshire 2 Research Ethics Committee. To collect additional data the task was also expanded to include patients seen in clinic as part of their routine clinical assessment and the collection of this data was classified as a service evaluation with the Patient Safety Unit at Addenbrooke’s Hospital (Project Register Number: 4256). The work was carried out in accordance with the World Medical Association Declaration of Helsinki 23. All preHD and HD participants had a positive genetic test for the HD mutation and were assessed using the UHDRS motor examination along with their total functional capacity (TFC) sub-section 24. PreHD participants were defined by having a diagnostic confidence level on the UHDRS of less than 4. Disease burden score was calculated using the CAG-Age Product Scale (CAPS) 25 , 26.
Nut and bolt task
The nut and bolt task was designed as a simple test to examine dexterity of the hands and fingers. The participants were asked to screw a nut onto a bolt in one direction using either the left or right hand; participants were not allowed to flick the nut and the hand holding the bolt had to remain static/stationary. The task consisted of 3 different sized nuts and bolts and was timed for both hands for all conditions. The task was performed using two test conditions; while the hands were supported resting on a table or unsupported, with the hands held in mid air. The task was timed using a standard stopwatch, the timer was started when the participant began screwing the nut onto the bolt and the timer was stopped when the nut reached the top of the bolt and could go no further. All those administering this test were instructed in how to carry out the test, but the simplicity of the task and the use of a simple stopwatch meant that no extensive training was needed.
Statistics
Statistical analysis was performed using IBM SPSS software version 21.0. The main outcome for the task was the time it took for each participant to screw the nut onto the bolt using the left and right hand sequentially, both supported and unsupported. The independent variables were the three groups (Controls, PreHD, HD). Normality for all the dependent variables was tested using one-sample Kolmogorov-Smirnov tests. Group effects for variables that were normally distributed, such as age, CAG repeat, and UHDRS motor score were analysed using parametric tests (ANOVA) followed by post-hoc comparisons (T-test) with Bonferroni corrections where significance was present, all p values reported in the manuscript are already corrected. The group main effect was found to be significant. Variables with a skewed distribution, including data obtained from the nut and bolt assessments were first logarithmically transformed to obtain normality and analysed as above with the exception of the total functional capacity scores which were analysed using Mann-Whitney U tests. Partial Spearman correlations were performed using age as a covariate.
RESULTS
Participant demographics
A total of 83 participants were tested on this task and were divided into 3 groups: healthy controls, preHD and manifest HD participants (See table 1). As would be expected, manifest HD participants had a higher UHDRS total score [p < 0.001] and a lower TFC score [p < 0.001] than preHD participants. Healthy controls and preHD participants displayed similar baseline demographics (age) [p = 0.863], while participants with manifest HD were slightly older than control participants [p = 0.004] (Table 1).
Table 1:Demographic and clinical characteristics of study participants.
| Group | Age | CAG | UHDRS | TFC |
|---|---|---|---|---|
| Premanifest (n=24) | 47.47 ± 2.66 | 41.73 ± 0.662 | 3.87 ± 0.975 | 12.26 ± 0.492 |
| Manifest (n=27) | 56.30 ± 2.62* | 43.74 ± 0.796 | 24.07 ± 2.28# | 8.78 ± 2.28# |
| Controls (n=32) | 43.08 ± 3.18 | - | - | - |
Table 1. Table shows mean ± S.E.M. UHDRS: Unified Huntington’s Disease Rating Scale: total motor score, TFC: total functional capacity. *indicates statistically significant difference when compared to controls whereas # indicates statistically significant difference when compared to preHD.PreHD participants show impaired performance in their performance with the non-dominant hand compared to controls.
PreHD participants show impairments in their performance with the non-dominant hand compared to controls.
PreHD participants were impaired on several aspects of the nut and bolt task when compared to the healthy controls, particularly when the non-dominant hand was being tested. Significant changes were observed with all sizes of the nut and bolt when the non-dominant hand was in the unsupported condition [small: p = 0.036. medium: p = 0.006 large: p = 0.001, table 2] and the large nut and bolt when the non-dominant hand was supported [p = 0.034]. In contrast, only one measurement was significantly different when testing the dominant hand [medium, unsupported: p = 0.009] indicating that dominant hand function is relatively well preserved at this stage of the condition (Table 2).
Anti-dopaminergic medication has no effect on performance on the nut and bolt task.
Anti-dopaminergic medications such as sulpiride and olanzapine are commonly used for treating the motor features of HD and hence may have an effect on performance in the nut and bolt task. In order to analyse the effect of such medications, we divided the preHD and HD participants into those who were receiving anti-dopaminergic medications and those who were not. Due to the nature of prescribing such medication for symptomatic relief of the motor features of HD, patients who were receiving such medication were in a more advanced stage of disease and hence were significantly older and a higher total motor score on the UHDRS [TMS: t = 3.29, p = 0.002, Age: t = 2.85, p = 0.006]. Therefore in order to minimise such confounding facts we included age and the total motor score as covariates in our analysis. Our results showed that there was no statistically significant difference in motor performance between those receiving anti-dopaminergic medication and those who were not [F = 1.75, p > 0.111].
Table 2: Median times for each group to complete nut and bolt task; for all task conditions.
| Median (Seconds) | p values | |||||||
|---|---|---|---|---|---|---|---|---|
| Controls | PreHD | HD | Control-PreHD | PreHD-HD | Controls-HD | |||
| Non Dominant | Supported | Small | 24 | 29 | 37 | 0.435 | 0.024 | <0.001 |
| Medium | 19 | 25 | 31 | 0.076 | 0.04 | <0.001 | ||
| Large | 14.5 | 24 | 21 | 0.034 | 0.093 | <0.001 | ||
| Unsupported | Small | 19 | 25 | 36 | 0.036 | 0.032 | <0.001 | |
| Medium | 14.5 | 23 | 30 | 0.006 | 0.198 | <0.001 | ||
| Large | 10 | 19 | 23.5 | 0.001 | 0.235 | <0.001 | ||
| Dominant | Supported | Small | 23 | 25 | 43.5 | 0.152 | 0.002 | <0.001 |
| Medium | 19.6 | 23 | 35.5 | 0.122 | 0.021 | <0.001 | ||
| Large | 17.5 | 20 | 29 | 0.559 | 0.084 | <0.01 | ||
| Unsupported | Small | 21 | 22 | 36.5 | 0.239 | 0.02 | <0.001 | |
| Medium | 16.5 | 21 | 32 | 0.009 | 0.052 | <0.001 | ||
| Large | 13 | 15 | 26.5 | 0.14 | 0.006 | <0.001 | ||
Manifest HD patients are significantly impaired in all domains of the nut and bolt task
Compared to controls the manifest group performed worse on all conditions tested while the preHD group appeared to demonstrate deficits under specific conditions (Table 2). In particular, whereas dominant hand function was not significantly different when comparing preHD to controls, manifest HD participants showed impairments compared to preHD when the dominant hand was tested with the small and medium nut and bolts whilst supported [small: p = 0.002, medium: p = 0.021] and the small and large nut and bolts whilst unsupported [small: p = 0.02, large: p = 0.006]. Performance with the small nut and bolt using the unsupported non dominant hand is significantly impaired at all stages of disease [preHD compared to controls: p = 0.036, HD compared to preHD: p = 0.032] (Figure 1) and correlates significantly with disease burden score (r=0.374), even when controlled for age [p = 0.021] (Figure 2). Finally all components of the nut and bolt task correlated with the patients UHDRS score in both preHD and manifest patients [small non-dominant unsupported nut and bolt: r = 0.494, p = 0.001].
Non dominant unsupported hand measurements of time to complete small nut and bolt test for each group.
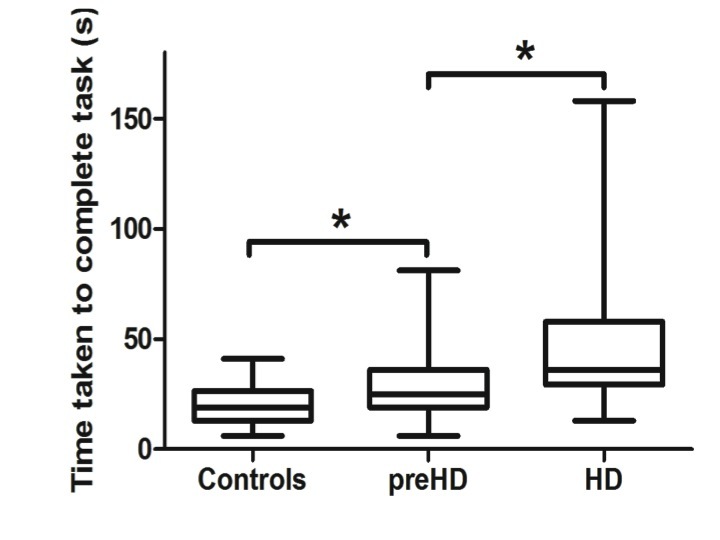
Unsupported small nut and bolt in the non dominant hand in each group. Significance is denoted by asterisks, preHD compared to controls: p = 0.036, HD compared to preHD: p = 0.032.
Small nut and bolt measurement correlates with Disease Burden Score.
![The time taken for the non dominant unsupported hand to complete the small nut and bolt task correlates with disease burden score [r = 0.374, p = 0.021]. Correlation is significant at the 0.05 level (2-tailed).](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/9e5d/4570842/227885b15a25/Slide12.jpg)
The time taken for the non dominant unsupported hand to complete the small nut and bolt task correlates with disease burden score [r = 0.374, p = 0.021]. Correlation is significant at the 0.05 level (2-tailed).
Discussion
The ability to detect, quantify and follow the loss of hand dexterity in HD is of importance for diagnosing patients at the earliest stages of disease, monitoring disease progression and evaluating the efficacy of novel treatments. Previous tests that have been proposed to be useful in this regard include finger 8 , 9 and hand tapping 10 , 11 , 12 , 13 with both tasks tracking disease course over time 10 , 27 , 28. However, while they capture changes in motor speed they do not measure changes in dexterity. In our new study, we introduced a novel task: the nut and bolt test, which we have now shown to be a useful way of measuring the impact of HD on fine motor coordination in a large group of patients. In particular, we have found significant differences in performance between preHD and controls in their non dominant hand with the dominant hand function remaining intact until later in the disease course. Furthermore the non dominant nut and bolt performance correlated with disease burden scores suggesting a relationship with proximity to disease onset. Therefore, the nut and bolt task may be both diagnostically useful and helpful for identifying premanifest patients at immediate risk of developing manifest disease who may also therefore be suitable for future trials of disease modifying therapy.
This finding of decreased performance in the non dominant hand is in agreement with the existing literature; specifically the TRACK-HD study that showed that there is a reduction in finger tapping in the non dominant hand over time 28. In the cohort of premanifest and early HD patients, it was found that tapping was one of the few functional measurements that had significant differences in preHD participants compared to controls and also progressed over time 28. Previously, differences in performance on simple speed tapping tasks in preHD and early stage HD cohorts have been correlated with cortical thickness, disease burden scores and motor scores 18 and in another study manifest and early HD patients tapping scores correlated with cognitive test scores, regional brain atrophy and UHDRS scores 19. All of which highlights that these simple motor measures are useful measures of disease stage with a pathology that can also be quantified.
Other motor tasks that have also be used in a similar way in HD include saccadic eye movements in which it has been shown that preHD patients can have a number of abnormalities that seem to track disease course over time 17. Quantitative measurements of tongue protrusion force in preHD and HD have also detected deficits in motor force 15 and in motor speech timing tasks in manifest HD patients showing impaired speech rhythm with defects in speech rate, increased pauses, impaired syllable repetition all of which correlated with motor tapping assessments 16. Other studies have shown slowing of rapid alternating movements in HD patients, as well as deficits in tapping and on peg insertion tasks 20. This confirms earlier findings where the peg insertion task was significantly different in HD patients compared to controls but failed to detect early changes in preHD groups 21. These tasks along with our simple task may suggest that the combination of speed and simple movements may highlight early deficits in HD, especially in the less dextrous non dominant hand. Indeed our nut and bolt task is unique in that is takes into account speed, dexterity, hand movements and motivation and as such may be more sensitive to the very earliest problems in HD which effects all of these functions. This would fit with imaging and post mortem data showing that those brain regions involved in these motor and affective activities are known to be abnormal in preHD and early HD including the striatum 28 , 29 , 30 the nucleus accumbens, pallidum 31 precentral and postcentral gyri as well as the supplementary motor area 32. Thus the clinical data sits well with the known neuropathology of premanifest and early HD.
Although, our test has many advantages including its cost and ease of administration and simple interpretation of results there are also some limitations with our study . This includes the absence of longitudinal data, and the need to trial it in larger numbers of patients and the problems of employing it in very advanced patients. However, this latter group are unlikely to be the target of new therapeutic interventions in the first instance, so this is less of an issue. Furthermore the nut and bolt task was timed manually using a standard stop watch and although the timing was not automated, each individual was trained in the same way and thus is unlikely to have contributed to any significant issues on the accuracy of the data collection. However using an automated timer may be a useful addition to our task. Finally our study captured a selection of un-medicated and medicated preHD and HD patients seen in our regional clinic, including HD patients on anti-dopaminergic medication such as sulpiride and olanzapine. Although we found no significant difference in our task in those patients on anti-dopaminergic medications compared to those who were not, we cannot rule out that this may effect their performance. In the future longitudinal studies that specifically address this issue are needed.
In summary, we describe a simple, inexpensive and robust task that is useful in defining disease onset as well as being of possible value in therapeutic trials of disease modifying therapies in both manifest patients and pre-HD patients approaching the time of phenoconversion. Furthermore it can be used in any clinic on its own or as part of a battery of tests to assess dexterity across all stages of HD given its simplicity and low cost.
Competing Interests
The authors have declared that no competing interests exist.
Author Information
Lucy M. Collins and Faye Begeti contributed equally to this work.
Acknowledgments
We are grateful to an NIHR award of a Biomedical Research Centre to Addenbrooke’s Hospital and the University of Cambridge. We are also grateful to William Carey-Hill for work on the conceptualization of the study.
Biography
Lecturer in Healthcare Science at Anglia Ruskin University
Funding Statement
The work in the John van Geest Centre for Brain Repair, Cambridge, UK was funded by an NIHR award of a Biomedical Research Centre (http://www.nihr.ac.uk/about/biomedical-research-centres.htm) to Addenbrooke’s Hospital and the University of Cambridge grant number RG64473. The work in the John van Geest Centre for Brain Repair, Cambridge, UK was also funded by CHDI Foundation (http://chdifoundation.org) grant number RG50786 and Jacques and Gloria Gossweiler Foundation (http://www.jggf.ch/en/) grant number RG77329. Lucy Collins is funded by the Rosetrees Trust (http://www.rosetreestrust.co.uk). Faye Begeti was funded through a Medical Research Council Studentship and James Baird Fund. Sarah L. Mason is funded by an NIHR Clinical Research Network (http://www.nihr.ac.uk/about/biomedical-research-centres.htm) grant number RG64473. The role of the funders was to support salaries and consumables for the project. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Contributor Information
Francesca Panin, John van Geest Centre for Brain Repair, Cambridge, United Kingdom; Faculty of Medical Sciences, Anglia Ruskin University, Cambridge, United Kingdom.
Alpar S. Lazar, John van Geest Centre for Brain Repair, Cambridge, United Kingdom
Travis Cruickshank, School of Medical Sciences, Edith Cowan University, Perth, Western Australia, Australia.
Mel Ziman, School of Medical Sciences, Edith Cowan University, Perth, Western Australia, Australia.
Sarah L. Mason, John van Geest Centre for Brain Repair, Cambridge, United Kingdom
Roger A. Barker, John van Geest Centre for Brain Repair, Cambridge, United Kingdom; School of Medical Sciences, Edith Cowan University, Perth, Western Australia, Australia
References
- 1.Rosas HD, Salat DH, Lee SY, Zaleta AK, Pappu V, Fischl B, Greve D, Hevelone N, Hersch SM. Cerebral cortex and the clinical expression of Huntington's disease: complexity and heterogeneity. Brain. 2008 Apr;131(Pt 4):1057-68. PubMed PMID:18337273. [DOI] [PMC free article] [PubMed]
- 2.Reading SA, Yassa MA, Bakker A, Dziorny AC, Gourley LM, Yallapragada V, Rosenblatt A, Margolis RL, Aylward EH, Brandt J, Mori S, van Zijl P, Bassett SS, Ross CA. Regional white matter change in pre-symptomatic Huntington's disease: a diffusion tensor imaging study. Psychiatry Res. 2005 Oct 30;140(1):55-62. PubMed PMID:16199141. [DOI] [PubMed]
- 3.Rosas HD, Tuch DS, Hevelone ND, Zaleta AK, Vangel M, Hersch SM, Salat DH. Diffusion tensor imaging in presymptomatic and early Huntington's disease: Selective white matter pathology and its relationship to clinical measures. Mov Disord. 2006 Sep;21(9):1317-25. PubMed PMID:16755582. [DOI] [PubMed]
- 4.Aylward EH, Brandt J, Codori AM, Mangus RS, Barta PE, Harris GJ. Reduced basal ganglia volume associated with the gene for Huntington's disease in asymptomatic at-risk persons. Neurology. 1994 May;44(5):823-8. PubMed PMID:8190282. [DOI] [PubMed]
- 5.Aylward EH, Codori AM, Barta PE, Pearlson GD, Harris GJ, Brandt J. Basal ganglia volume and proximity to onset in presymptomatic Huntington disease. Arch Neurol. 1996 Dec;53(12):1293-6. PubMed PMID:8970459. [DOI] [PubMed]
- 6.Andrich J, Saft C, Ostholt N, Müller T. Complex movement behaviour and progression of Huntington's disease. Neurosci Lett. 2007 Apr 18;416(3):272-4. PubMed PMID:17321683. [DOI] [PubMed]
- 7.Rosenblatt A, Liang KY, Zhou H, Abbott MH, Gourley LM, Margolis RL, Brandt J, Ross CA. The association of CAG repeat length with clinical progression in Huntington disease. Neurology. 2006 Apr 11;66(7):1016-20. PubMed PMID:16606912. [DOI] [PubMed]
- 8.Tabrizi SJ, Langbehn DR, Leavitt BR, Roos RA, Durr A, Craufurd D, Kennard C, Hicks SL, Fox NC, Scahill RI, Borowsky B, Tobin AJ, Rosas HD, Johnson H, Reilmann R, Landwehrmeyer B, Stout JC. Biological and clinical manifestations of Huntington's disease in the longitudinal TRACK-HD study: cross-sectional analysis of baseline data. Lancet Neurol. 2009 Sep;8(9):791-801. PubMed PMID:19646924. [DOI] [PMC free article] [PubMed]
- 9.Tabrizi SJ, Scahill RI, Durr A, Roos RA, Leavitt BR, Jones R, Landwehrmeyer GB, Fox NC, Johnson H, Hicks SL, Kennard C, Craufurd D, Frost C, Langbehn DR, Reilmann R, Stout JC. Biological and clinical changes in premanifest and early stage Huntington's disease in the TRACK-HD study: the 12-month longitudinal analysis. Lancet Neurol. 2011 Jan;10(1):31-42. PubMed PMID:21130037. [DOI] [PubMed]
- 10.Collins LM, Lazic SE, Barker RA. A retrospective analysis of hand tapping as a longitudinal marker of disease progression in Huntington's disease. BMC Neurol. 2014 Feb 24;14:35. PubMed PMID:24564568. [DOI] [PMC free article] [PubMed]
- 11.Rupp J, Blekher T, Jackson J, Beristain X, Marshall J, Hui S, Wojcieszek J, Foroud T. Progression in prediagnostic Huntington disease. J Neurol Neurosurg Psychiatry. 2010 Apr;81(4):379-84. PubMed PMID:19726414. [DOI] [PMC free article] [PubMed]
- 12.Antoniades CA, Xu Z, Mason SL, Carpenter RH, Barker RA. Huntington's disease: changes in saccades and hand-tapping over 3 years. J Neurol. 2010 Nov;257(11):1890-8. PubMed PMID:20585954. [DOI] [PubMed]
- 13.Michell AW, Goodman AO, Silva AH, Lazic SE, Morton AJ, Barker RA. Hand tapping: a simple, reproducible, objective marker of motor dysfunction in Huntington's disease. J Neurol. 2008 Aug;255(8):1145-52. PubMed PMID:18465109. [DOI] [PubMed]
- 14.Reilmann R, Bohlen S, Klopstock T, Bender A, Weindl A, Saemann P, Auer DP, Ringelstein EB, Lange HW. Grasping premanifest Huntington's disease - shaping new endpoints for new trials. Mov Disord. 2010 Dec 15;25(16):2858-62. PubMed PMID:20818671. [DOI] [PubMed]
- 15.Reilmann R, Bohlen S, Klopstock T, Bender A, Weindl A, Saemann P, Auer DP, Ringelstein EB, Lange HW. Tongue force analysis assesses motor phenotype in premanifest and symptomatic Huntington's disease. Mov Disord. 2010 Oct 15;25(13):2195-202. PubMed PMID:20645403. [DOI] [PubMed]
- 16.Skodda S, Schlegel U, Hoffmann R, Saft C. Impaired motor speech performance in Huntington's disease. J Neural Transm. 2014 Apr;121(4):399-407. PubMed PMID:24221215. [DOI] [PubMed]
- 17.Blekher T, Johnson SA, Marshall J, White K, Hui S, Weaver M, Gray J, Yee R, Stout JC, Beristain X, Wojcieszek J, Foroud T. Saccades in presymptomatic and early stages of Huntington disease. Neurology. 2006 Aug 8;67(3):394-9. PubMed PMID:16855205. [DOI] [PubMed]
- 18.Bechtel N, Scahill RI, Rosas HD, Acharya T, van den Bogaard SJ, Jauffret C, Say MJ, Sturrock A, Johnson H, Onorato CE, Salat DH, Durr A, Leavitt BR, Roos RA, Landwehrmeyer GB, Langbehn DR, Stout JC, Tabrizi SJ, Reilmann R. Tapping linked to function and structure in premanifest and symptomatic Huntington disease. Neurology. 2010 Dec 14;75(24):2150-60. PubMed PMID:21068430. [DOI] [PMC free article] [PubMed]
- 19.Saft C, Andrich J, Meisel NM, Przuntek H, Müller T. Assessment of simple movements reflects impairment in Huntington's disease. Mov Disord. 2006 Aug;21(8):1208-12. PubMed PMID:16700032. [DOI] [PubMed]
- 20.Müller T, Saft C, Andrich J, Harati A. Diadochokinetic movements differ between patients with Huntington's disease and controls. NeuroRehabilitation. 2013;33(4):649-55. PubMed PMID:24018370. [DOI] [PubMed]
- 21.Saft C, Andrich J, Meisel NM, Przuntek H, Müller T. Assessment of complex movements reflects dysfunction in Huntington's disease. J Neurol. 2003 Dec;250(12):1469-74. PubMed PMID:14673581. [DOI] [PubMed]
- 22.The effects of extra vehicular activity (EVA) gloves on human performance
- 23.World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013 Nov 27;310(20):2191-4. PubMed PMID:24141714. [DOI] [PubMed]
- 24.Unified Huntington's Disease Rating Scale: reliability and consistency. Huntington Study Group. Mov Disord. 1996 Mar;11(2):136-42. PubMed PMID:8684382. [DOI] [PubMed]
- 25.Paulsen JS, Hayden M, Stout JC, Langbehn DR, Aylward E, Ross CA, Guttman M, Nance M, Kieburtz K, Oakes D, Shoulson I, Kayson E, Johnson S, Penziner E. Preparing for preventive clinical trials: the Predict-HD study. Arch Neurol. 2006 Jun;63(6):883-90. PubMed PMID:16769871. [DOI] [PubMed]
- 26.Zhang Y, Long JD, Mills JA, Warner JH, Lu W, Paulsen JS. Indexing disease progression at study entry with individuals at-risk for Huntington disease. Am J Med Genet B Neuropsychiatr Genet. 2011 Dec;156B(7):751-63. PubMed PMID:21858921. [DOI] [PMC free article] [PubMed]
- 27.Tabrizi SJ, Reilmann R, Roos RA, Durr A, Leavitt B, Owen G, Jones R, Johnson H, Craufurd D, Hicks SL, Kennard C, Landwehrmeyer B, Stout JC, Borowsky B, Scahill RI, Frost C, Langbehn DR. Potential endpoints for clinical trials in premanifest and early Huntington's disease in the TRACK-HD study: analysis of 24 month observational data. Lancet Neurol. 2012 Jan;11(1):42-53. PubMed PMID:22137354. [DOI] [PubMed]
- 28.Tabrizi SJ, Scahill RI, Owen G, Durr A, Leavitt BR, Roos RA, Borowsky B, Landwehrmeyer B, Frost C, Johnson H, Craufurd D, Reilmann R, Stout JC, Langbehn DR. Predictors of phenotypic progression and disease onset in premanifest and early-stage Huntington's disease in the TRACK-HD study: analysis of 36-month observational data. Lancet Neurol. 2013 Jul;12(7):637-49. PubMed PMID:23664844. [DOI] [PubMed]
- 29.Scahill RI, Hobbs NZ, Say MJ, Bechtel N, Henley SM, Hyare H, Langbehn DR, Jones R, Leavitt BR, Roos RA, Durr A, Johnson H, Lehéricy S, Craufurd D, Kennard C, Hicks SL, Stout JC, Reilmann R, Tabrizi SJ. Clinical impairment in premanifest and early Huntington's disease is associated with regionally specific atrophy. Hum Brain Mapp. 2013 Mar;34(3):519-29. PubMed PMID:22102212. [DOI] [PMC free article] [PubMed]
- 30.Reiner A, Albin RL, Anderson KD, D'Amato CJ, Penney JB, Young AB. Differential loss of striatal projection neurons in Huntington disease. Proc Natl Acad Sci U S A. 1988 Aug;85(15):5733-7. PubMed PMID:2456581. [DOI] [PMC free article] [PubMed]
- 31.van den Bogaard SJ, Dumas EM, Acharya TP, Johnson H, Langbehn DR, Scahill RI, Tabrizi SJ, van Buchem MA, van der Grond J, Roos RA. Early atrophy of pallidum and accumbens nucleus in Huntington's disease. J Neurol. 2011 Mar;258(3):412-20. PubMed PMID:20936300. [DOI] [PMC free article] [PubMed]
- 32.Carey LM, Abbott DF, Egan GF, Tochon-Danguy HJ, Donnan GA. The functional neuroanatomy and long-term reproducibility of brain activation associated with a simple finger tapping task in older healthy volunteers: a serial PET study. Neuroimage. 2000 Feb;11(2):124-44. PubMed PMID:10679185. [DOI] [PubMed]