

Abstract
Rapid deceleration during running is key for successful participation in most childhood activities and sports; this requires modulation of body momentum and consequent challenges to postural equilibrium. The purpose of this study was to investigate the strategies employed by adults and children to control forward momentum and terminate running gait. Sixteen young adults and 15 pre-pubertal children completed two tasks as fast as possible: an unobstructed run (RUN) and a run and stop (STOP) at a pre-determined location. For STOP, center of mass (COM) approach velocity and momentum prior to deceleration and spatiotemporal characteristics and COM position during deceleration were compared between groups. Position and velocity variables were normalized to height and maximum velocity during RUN, respectively. Children used fewer steps with relatively longer step length to decelerate over a relatively longer distance and longer time than adults. Children approached at higher relative velocity than adults, but adults approached with greater momentum. Adults positioned their COM lower and more posterior than children throughout deceleration. Our results suggest that pre-pubertal children and young adults employ different strategies to modulate body momentum, with adults exhibiting mechanics characteristic of a more stable strategy. Despite less stable mechanics, children and adults achieved similar success.
Keywords: Gait termination, Dynamic stability, Center of mass, Children
1. Introduction
Research focusing on the development of locomotor skills in children has found that while typically developing children exhibit adult-like gait kinematics by the age of 7 years (Sutherland, 1997), development of more complex locomotor strategies appear to continue into late childhood. Differences between children and adults are observed during locomotor tasks that have more challenging environmental demands. During reduced visual conditions (Berard & Vallis, 2006; Hallemans et al., 2009) and when asked to negotiate more than one obstacle during gait (Berard & Vallis, 2006) children make adjustments including decreased walking speed and step length, and increased step width while adults do not. These adjustments are thought to characterize a more cautious strategy in children when faced with more complex or challenging locomotor tasks. In addition, during obstacle circumvention tasks, pre-pubertal children take longer than adults to implement required postural adjustments, such as altered foot placement and body segment rotations (Vallis & McFadyen, 2005). Age-related differences in joint kinetics and postural strategies for more complex locomotor tasks are attributed to the lack of neuromuscular maturity (Berard & Vallis, 2006; Ganley & Powers, 2005; McFadyen, Malouin, & Dumas, 2001).
The ability to rapidly decelerate and change directions while running is key for successful participation in most forms of childhood activities and sports (e.g., tag, soccer). Understanding how typically developing children perform locomotor tasks relevant to physical activity participation is important for establishing age-appropriate expectations as children who do not attain age-appropriate motor skills are less likely to engage in physical activities (Barnett, van Beurden, Morgan, Brooks, & Beard, 2009; Smyth & Anderson, 2000). Similar to locomotor tasks used in previous experimental paradigms, running tasks require modulation of body momentum (the product of mass and velocity) and consequent challenges to postural equilibrium. However, during running, increased speed and momentum add additional challenges to postural equilibrium, which possibly increases task complexity. Based on the results of the studies mentioned above using more complex gait tasks, it is expected that children would adopt a more cautious strategy when performing running tasks; however, it is not known how the interpretation of data from complex locomotor tasks translates to faster tasks related to physical activity participation.
Differences in gait spatiotemporal variables such as velocity and step length and width are thought to reflect strategies used for stability of the center of mass (COM) (MacLellan & Patla, 2006); however, direct measures of COM may provide more detailed information regarding postural strategies. Stability during dynamic tasks is achieved not just by maintaining the projection of the COM within the base of support (BOS), but by maintaining the relationship between these variables (COM and BOS) in the context of the magnitude and direction of the COM velocity. This relationship has been established during walking gait termination with the adult population, as adults use a stereotypical strategy to control forward momentum and maintain dynamic stability (Bishop, Brunt, Pathare, & Patel, 2004; Jian, Winter, Ishac, & Gilchrist, 1993). Pai and Patton (1997) modeled this relationship and found that for a given initial COM posterior position relative to the BOS during the terminating step there is a range of horizontal velocities that can be successfully reduced to zero. If the COM forward velocity is too great and falls outside this range, dynamic stability cannot be maintained and the individual will be required to change his or her BOS and take another step. Unlike walking gait termination that can be accomplished with less than 2 steps (Hase & Stein, 1998), stopping forward progression during running requires modulation of faster velocity and is likely accomplished over several steps. Comparison of COM position and velocity variables between children and adults across deceleration of a running termination task will provide information about how adults and children maintain dynamic stability during tasks more closely related to the demands of physical activities.
Using an experimental task designed to increase locomotor demands over those of steady state gait by increasing the demands for modulation of body momentum, this study aimed to investigate the strategies employed by adults and children to control forward momentum and terminate running gait. Based on previous literature, it was hypothesized that children would utilize mechanics that would be suggestive of a more stable strategy when compared with adults, observed with changes in gait spatiotemporal characteristics and COM velocity and position variables during running termination task.
2. Methods
2.1. Participants
Thirty-one male subjects participated (16 adults and 15 children; Table 1). A priori analysis from pilot data determined that 12 subjects per group would provide adequate power to detect group differences with alpha of 0.05 and 90% power.
Table 1.
Participants’ characteristics.
| Adults (n = 16) | Children (n = 15) | |
|---|---|---|
| Age (yrs) | 27.13 (3.98) | 8.87 (1.46) |
| Mass (kg) | 73.96 (7.89) | 32.02 (7.26) |
| Height (m) | 1.77 (0.09) | 1.35 (0.12) |
| COM height (m) | 0.95 (0.05) | 0.66 (0.07) |
| Leg length (m) | 0.93 (0.06) | 0.69 (0.08) |
| Physical activity (min/week) | 376.25 (229.31) | 728.00 (419.71) |
Adults, ages 20–35 years, and children, ages 7–11 years, considered physically active were recruited. Physically active was defined as engaging in physical activity for at least 150 and 420 min per week for adults and children, respectively (USDHHS, 2008). Typically developing pre-pubertal children were recruited to control for effects of motor development (Sundermier, Woolacott, Roncesvalles, & Jensen, 2001) and physical maturation (puberty) (Sigward, Pollard, Havens, & Powers, 2012; Sigward, Pollard, & Powers, 2012) on performance. Classification as pre-pubertal was based on the scores obtained from parents’ report of Tanner stages for pubic hair development from figure drawings (Schmitz et al., 2004). Children were included if they indicated the absence of pubic hair (stage 1). Developmental level is a better predictor of reactive postural strategies than chronological age (Sundermier et al., 2001). To control for the influence of motor proficiency, children were included if they could complete age-appropriate locomotor skills defined by Bruininks-Oseretsky Test of Motor Proficiency (BOTMP) (Bruininks, 1978). All children were classified as average or above compared with normative data (Bruininks, 1978). Participants were excluded if they had a history of lower extremity or spine injury in the last six months, concurrent injury that restricted physical activities or any other condition that may impair their ability perform the experimental tasks. All testing procedures were explained and informed consent was obtained as approved by the University's Institutional Review Board.
2.2. Procedures
Testing took place at the Division of Biokinesiology & Physical Therapy's Human Performance Laboratory, located within the Competitive Athlete Training Zone (CATZ), Pasadena. Participants wore their own running/athletic shoes. Prior to testing, adult subjects and children's parents filled out the Children's Physical Activity Questionnaire (Chinapaw, Mokkink, van Poppel, van Mechelen, & Terwee, 2010; Nor Aini, Poh, & Chee, 2013) to quantify the average number of minutes per week of physical activity in the previous month. Height and mass were measured. Children performed locomotor subtests of BOTMP short-form, including running speed and agility, single limb standing, and walking forward heel-to-toe on balance beam.
Reflective markers were placed over anatomical landmarks to reconstruct the three-dimensional movement of trunk, pelvis, and lower extremity segments. Marker placement included, bilaterally when applicable, the distal end of first toe (on the shoe), medial and lateral malleoli, medial and lateral epicondyles of femur, greater trochanters, iliac crests, L5–S1 junction, acromioclavicular joint, cervical process of C7. Marker clusters mounted on semi-rigid plates were secured to thighs, shanks, and posterior shoes. After a standing calibration trial was collected markers over anatomical landmarks were removed except for those over the iliac crests, L5–S1 junction, acromioclavicular joint, and C7. Participants performed an 8 min warm-up that included fundamental motor skills such as running, skipping, galloping, dodging, and sliding (Gallahue & Ozmun, 1998), and locomotor skills such as carioca, high heels, and high knees. To control for fatigue as a potential confounding factor, participants were asked to rate their level of fatigue using a scale of perceived fatigue from zero to ten, with zero representing no fatigue and ten representing extreme fatigue. The perceive fatigue score prior to testing was 3.1 ± 1.3 for the adults and 3.5 ± 1.8 for the children, suggesting that fatigue was not an issue for the participants of our study.
An eleven-camera motion analysis system (Qualisys®, Gothenburg, Sweden) captured three-dimensional kinematic data (250 Hz). Participants performed two experimental tasks. First, participants ran as fast as possible on a 21-m unobstructed pathway (RUN). Three trials were collected. Next, participants ran as fast as possible and stopped at a pre-determined location 13 m from the start position (STOP). A cylindrical piece of foam placed in front of the stop location provided a visual cue that could be identified from the start position. After coming to a complete stop as close to the foam target as possible, they were to maintain their balance and hold still, for a count of 2 (Fig. 1). Infrared timing gates (Automatic Timing and Controls, Lancaster, PA) positioned 6 meters apart and 5 meters from the start were used to provide running time feedback. The number of seconds it took them to run through the timing gates was displayed after each trial. Participants were encouraged to run as fast as possible and try to decrease the time it took them to complete the task after each trial. The first trial was considered a familiarization trial and was not used for analysis. Five successful trials were collected. A trial was considered unsuccessful if the participant touched the foam target or stepped over it.
Fig. 1.

Experimental set-up. A sequence of several steps within the deceleration phase (from left to right) for an adult participant performing the STOP task. Participants were asked to run as fast as possible and come to a complete stop (maintaining their balance and holding their posture still) as close to the foam target as possible.
2.3. Data analysis
Marker trajectories were filtered using a fourth order Butterworth low-pass filter with a 12 Hz cut-off frequency. Three-dimensional kinematics were calculated using Visual3D™ (C-Motion, Inc., Rockville, MD, USA) software. Local coordinate systems of trunk, pelvis, thighs, shanks, and feet were derived from the standing calibration trial. Lower extremity segments and the thorax were modeled as frustra of cones and the pelvis as a cylinder. Six degrees-of-freedom of each segment were determined from the segment's triad by transforming the triad of markers to the position and orientation of each segment determined from the standing calibration trial. Joint kinematics were calculated using a joint coordinate approach (Grood & Suntay, 1983).
COM position was calculated as the weighted average of the COM position of 8 body segments: 6 lower extremity segments, pelvis, and trunk. Segmental masses were assigned based on the anthropometric data of Dempster (1955) for adults and Jensen (1986) for children. COM position variables were normalized to the COM height (COMz) obtained from the static trial. For both tasks, COM forward velocity was calculated as the first derivative of COM position in the anterior–posterior (A–P) direction.
The deceleration phase of STOP was determined using COM forward velocity and the position of markers affixed to the heel and toes of the participant's shoes. The beginning of the deceleration phase was defined at the first initial contact (IC) of the step immediately following the peak COM forward velocity. Initial contact was determined as the minimum vertical position of the heel marker using a position-based detection algorithm and verified by visual inspection. The end of the deceleration phase was defined using the heel marker (for a heel strike) or toe marker (for a forefoot strike) trajectory from the terminating step as the time at which the forward displacement of the marker was zero, indicating that the foot came to a complete stop. This event was also determined using a position-based detection algorithm and verified by visual inspection. The terminating step was defined as the last full step and movement of the trailing limb to position the feet together was not considered.
Dependent variables considered for analysis were gait spatiotemporal characteristics, COM approach velocity, and COM position. Spatiotemporal variables including number of steps, step length, stance time, duration of deceleration and distance covered were calculated in the deceleration phase. Step length was calculated as the A–P distance between the heel marker at IC of each step. Stance time was calculated as the time between IC and toe-off for each step. Toe-off was determined as the onset of vertical motion of the kinematic marker placed over the toe (on the shoe) of the stance foot. Deceleration distance and step length were normalized to the participant's leg length (LL, as greater trochanter to floor).
Approach velocity was calculated as the average COM forward velocity 120 ms prior to the first IC of deceleration. This duration (120 ms) is equivalent to the average stance phase time in the steps prior to deceleration. Approach velocity was also considered as a percentage of the maximum velocity (Vmax) achieved during the RUN task (%Vmax) to account for performance differences between groups due to individual capabilities. Approach momentum was calculated as the product of approach velocity and the participant's mass (kg m/s).
COM position was calculated in A–P and vertical directions as the distance between the center of gravity (COG) of the stance foot and the body's COM and both were normalized to COMz. To characterize the position of the COM during deceleration, COM excursion was calculated during the stance phase of each deceleration step and was averaged across deceleration. The amount of time the COM was positioned anterior and vertical to the COG of the stance foot was determined. COM excursion during stance was calculated by subtracting the COM position at toe-off from the COM position at IC in the A–P and vertical directions. Excursions were averaged across deceleration steps. Average COM position across deceleration was calculated with respect to the right and left foot (Fig. 2). No differences were observed between feet; therefore, the average between the right and left feet were considered for analysis. The amount of time that the COM was positioned anterior to the foot COG and higher to the COM standing height (COMz) during deceleration was determined and presented as a percentage of the total deceleration phase time.
Fig. 2.
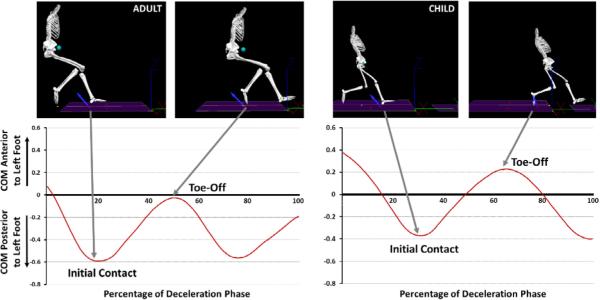
The position of the COM relative to the COG of the left foot across the deceleration phase using a representative trial of one adult (left) and one child (right). Distance is normalized to COMz. Arrows, initial contact and toe-off, indicate the beginning and end of stance phase of left foot.
2.4. Statistical analysis
Dependent variables considered for analysis were calculated prior to the deceleration phase (COM velocity variables: approach velocity, approach momentum, and approach %Vmax), and during the deceleration phase (spatiotemporal characteristics: time, number of steps, distance, normalized distance, step length, normalized step length, stance time; and COM position variables: A–P and vertical excursion, average posterior and vertical position, percent of time anterior to feet and above standing height).
Independent-samples t-tests (SPSS Inc., Chicago IL, USA) were used to determine whether differences exist between children and adults. When data were not normally distributed, Mann–Whitney U test was applied. Significance level was set at 0.05, and effect sizes (ES) were reported as Cohen d. The first 5 successful trials were averaged for each subject. A total of 13 unsuccessful trials for adults and 11 unsuccessful trials for children were observed.
3. Results
Besides step length (ES 0.18) and stance time (ES 0.38), significant differences between children and adults were observed for all spatiotemporal variables of the STOP task (Table 2). Compared with adults, children used fewer steps (ES 0.66) to decelerate over a shorter distance (ES 0.58) and longer deceleration time (ES 0.47). When normalized to leg length, children decelerated using relatively longer step length (ES 1.83) over a relatively longer distance (ES 0.98) compared with adults.
Table 2.
Spatiotemporal characteristics and center of mass (COM) position variables during the deceleration phase of the STOP task, mean (standard deviation).
| Adults | Children | p | |
|---|---|---|---|
| Time (s) | 0.72 (0.11) | 0.78 (0.15) | .04 |
| Number of steps | 5.13 (0.91) | 4.59 (0.72) | <.001 |
| Distance (m) | 2.89 (0.54) | 2.58 (0.51) | .04 |
| Normalized distancea | 3.10 (0.57) | 3.80 (0.82) | <.001 |
| Step length (m) | 0.71 (0.12) | 0.74 (0.15) | .26 |
| Normalized step lengtha | 0.77 (0.14) | 1.08 (0.20) | <.001 |
| Stance time (s) | 0.16 (0.03) | 0.17 (0.04) | .60 |
| COM A–P excursionb | 0.48 (0.09) | 0.65 (0.14) | .001 |
| COM vertical excursionb | 0.27 (1.9) | 0.13 (1.7) | .83 |
| Average COM posterior positionb | 0.30 (0.04) | 0.14 (0.08) | <.001 |
| Average COM vertical positionb | 0.86 (0.03) | 0.94 (0.07) | <.001 |
| % time COM is anterior to feetc | 8.99 (3.73) | 33.39 (6.00) | <.001 |
| % time COM is above standing heightc | n/a | 13.00 (14.0) | <.001 |
n/a = Not applicable (adults maintained a COM position that was lower than their COM standing height throughout deceleration).
Normalized to lower limb length.
Normalized to center of mass during static standing (COMz).
Normalized to time of deceleration phase.
Significant differences were observed in approach velocity and approach velocity normalized to Vmax (Fig. 3). Compared with adults, children approached the task at a slower velocity (ES 2.56). When normalized to the maximum velocity achieved during RUN, this relationship changed. Children approached the task at a higher relative (%Vmax) velocity than adults (ES 1.57). When mass was considered with approach velocity, adults exhibited 2.71 times greater forward momentum than children (ES 5.80; Fig. 3).
Fig. 3.
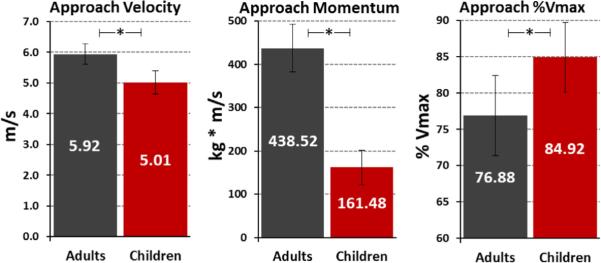
Center of mass (COM) velocity variables calculated prior to the deceleration phase. * Indicates significant differences at p < .001.
During the stance phase children exhibited a significantly greater A–P excursion of the COM than adults (ES 1.44, Table 2). No significant difference between groups was observed for COM vertical excursion (ES 0.08). The average position of the COM during the deceleration phase was less posterior (ES 2.53) and higher (ES 1.60) for children compared with adults. Also, children spent more time anterior to their feet (ES 0.22) during deceleration than adults (Table 2, Fig. 2). Children positioned their COM higher than the position of their COM during standing (COMz) while the position of the COM for the adults did not go above COMz at any time during deceleration (Table 2).
4. Discussion
The purpose of this study was to compare the strategies employed by adults and children to control whole body (COM) forward momentum during running gait termination. In contrast to our hypothesis, differences observed in spatiotemporal characteristics as well as COM velocity and position suggest that when compared with young adults, pre-pubertal children use mechanics indicative of a less stable strategy to modulate body momentum during a running termination task.
Adults and children had similar levels of success with task performance. On average children required a total of 16 trials to accomplished 5 successful trials without stepping over the target and adults required 18 trials. Small (~10%) but significant differences were observed with respect to the amount of time and distance required to decelerate. Adults stopped faster over a relatively shorter distance than children. Distinct differences were observed between adults and children with respect to their approach velocity and spatiotemporal characteristics. Adults approached the task at a faster velocity than children; however, when considered relative to the maximum velocity achieved during a straight run, children approached 10.5% faster than adults. For both children and adults deceleration took place over several steps before coming to a final stationary position. Nonetheless, this was accomplished by children with fewer, larger steps when compared with adults. Actual step length was not different between groups but when normalized, adults’ steps were 77% of their limb length versus 108% for the children. The faster relative approach speed and larger steps observed in the children would be indicative of a less cautious strategy.
Consistent with the differences in spatiotemporal variables, differences in COM position variables between groups also suggested that children employed features of a less stable strategy for deceleration. On average, the posterior position for the adults was 2 times greater than that of the children across the deceleration phase. This average position considers the distance between the COM and the foot on the ground throughout deceleration. As seen in Fig. 2, the COM is posterior to the foot at initial contact and moves anteriorly toward foot during stance. For a period of time after toe-off the COM travels anterior to the now swing foot before it is brought forward again to prepare for the next initial contact. Fig. 2 shows that children maintained a less posterior position overall, and their COM traveled anterior to their feet for approximately one third of the deceleration phase compared with adults. This is consistent with the greater COM A–P excursion observed in children, and is likely the result of the longer steps. In order to take a longer step, the COM would need to travel anterior to the swing limb as the stance limb reaches forward for the next step. Together, these variables describe a posture more closely related to forward propulsion of the body during gait or running (Jian et al., 1993), and not deceleration.
When considering the dynamic stability modeled by Pai and Patton (1997), a more posterior position of the COM is necessary to decelerate a faster forward velocity and a more anterior COM position would be considered unstable, potentially requiring an additional adjustment or step to maintain dynamic balance. While this relationship was modeled for termination of forward motion and identified during tasks performed under slow velocity conditions (Pai & Lee, 1994; Pai, Maki, Iqbal, McIlroy, & Perry, 2000; Pai, Rogers, Patton, Cain, & Hanke, 1998; Patton, Pai, & Lee, 1999), it suggests that the less posterior posture exhibited by the children is indicative of a less stable strategy. This trend was also apparent when considering the vertical position of their COM; in contrast to adults, children maintained a position that was on average higher than their standing height throughout the entire deceleration. This higher vertical position could provide a larger lever arm for destabilizing forces.
Together differences in spatiotemporal and COM position variables describe a strategy that reflects less stability or cautiousness on the part of the children. This is in contrast to previous studies that indicated that when the demands of loco-motor tasks increased (by adding obstacles or altering visual input) children adopted more stable mechanics by decreasing step length and velocity, and increasing step width (Berard & Vallis, 2006). It is not clear why children and adults used different strategies to modulate forward momentum using our experimental paradigm. Perhaps the more mature adults were able to anticipate the task demands and modulate their strategy appropriately (Pai & Lee, 1994; Rosengren, McAuley, & Mihalko, 1998). Even though the task allowed for planning, the longer time and distance required for deceleration combined with less stable deceleration mechanics in the children suggests that adult-like anticipatory adjustments for deceleration and termination were not made. This is consistent with Vallis and McFadyen who reported that, when compared with adults, children took longer to implement required postural adjustments to accomplish a locomotor task (Vallis & McFadyen, 2005). However, despite the differences in strategies, children and adults were able to complete the task with similar success. No differences between groups were observed in the number of failed trials, indicating that the strategies employed by the children (and adults) were appropriate to maintain dynamic stability.
Differences between children and adults may have also been the product of differing anthropometrics and as a consequence, physical demands. Although differences were observed for approach velocity, the magnitude of the difference between groups was not large (0.91 m/s) compared with the more pronounced difference in body mass (41.94 kg). As a result, approach momentum was 63% greater in adults than children suggesting that the demands to modulate forward momentum are lower for the children. Therefore, the children may not have needed to adopt the adult features of a more cautious strategy to successfully complete the task as fast as possible, as instructed. Moreover, the variables that are suggestive of a less stable strategy in children may represent an appropriately stable strategy based on their anthropometrics and abilities. Previous studies report that children as young as 5 years of age are able to make adult-like judgments to motor capabilities based on their individual anthropometrics (Cesari, Formenti, & Olivato, 2003) and the dynamics of their movement (Snapp-Childs & Bingham, 2009; Wilmut & Barnett, 2011). Comparisons between children and adults are inherently difficult due to the obvious differences in anthropometrics and physical abilities. Variables such as body mass index, muscle mass and available strength were not considered in the current study which may limit the interpretation of these data as age-related differences in these variables could also contribute to the differences observed between groups. Future studies considering anthropometrics and physical capabilities in the context of the task demands are needed to determine if the differences in strategies are indeed reflective of differences in stability.
While the overall interpretation of these data are in contrast to previous studies assessing locomotor strategies in children, direct comparisons between studies are not possible given the differences in experimental conditions. The current experimental paradigm primarily challenged dynamic stability and coordination of motion in a single plane without manipulations to sensory stimulation (e.g., Berard & Vallis, 2006) or requirements for precision over multiple steps (Berard & Vallis, 2006; Michel, Grobet, Dietz, & van Hedel, 2010). Our experimental task demands were more similar to the demands of athletic tasks or game requiring the participants to control body momentum to accurately reach a target as fast as possible. This is the first study to describe strategies employed by healthy pre-pubertal children and young adults to control body momentum in a task that is ecologically related to the demands of physical activity and sports.
Care was taken to control for the potential influence of puberty, developmental level, physical activity level, and sex on motor performance. While the ages of the children ranged from 7 to 11 years, they all fell in the same developmental range as indicated by their scores on the locomotor skills portion of Bruininks-Oseretsky Test of Motor Proficiency (Bruininks, 1978). Inclusion of participants across this age range was supported statistically as participants at either range of the age groups did not present as outliers in any outcome variable and visual inspection of the data did not reveal age related trends. Therefore, interpretation of the current data is limited to physically active, male, typically developing pre-pubertal children and active young adults. As such, our data provide a foundation for the study of the development of postural strategies to control forward momentum during more demanding tasks related to participation in physical activities. Further work comparing strategies across different ages and levels of physical development in both males and females will provide a more in-depth understanding of age-appropriate capabilities and how these strategies change with sex, age and physical and neurologic development. It is not known whether similar strategies would be observed in other populations, such as less physically active individuals, children exhibiting lower developmental levels, or different stages of maturation (i.e., puberty). The current study is the first step in establishing age-appropriate expectations for children involved in physical activities and sports that require manipulation of forward momentum. Future studies determining difference in strategies utilized by children who are developing typically (current study) and delayed will inform interventions aimed at improving skills needed for physical activity participation. This is particularly important in children because those who do not attain age-appropriate motor skills are less likely to engage in physical activity across their lifetime (Barnett et al., 2009).
Acknowledgements
This research was supported by the North American Society for Psychology of Sport and Physical Activity (NASPSPA). Also, this research was supported in part by grant # K12 HD0055929 from the National Institutes of Health (NIH) – United States. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. The authors would like to thank the Competitive Athlete Training Zone (CATZ), Pasadena, for their assistance with subject recruitment and the use of their facilities, and Alia H. Parvez, Dawn M. Joutras, and Ligia Y. Mochida, PT, MS, for their help during data collection and data processing.
Footnotes
Conflict of interest statement
No conflicts of interest are declared by the authors related to the completion of this project and manuscript.
References
- Barnett LM, van Beurden E, Morgan PJ, Brooks LO, Beard JR. Childhood motor skill proficiency as a predictor of adolescent physical activity. Journal of Adolescent Health. 2009;44:252–259. doi: 10.1016/j.jadohealth.2008.07.004. [DOI] [PubMed] [Google Scholar]
- Berard JR, Vallis LA. Characteristics of single and double obstacle avoidance strategies: A comparison between adults and children. Experimental Brain Research. 2006;175:21–31. doi: 10.1007/s00221-006-0529-0. [DOI] [PubMed] [Google Scholar]
- Bishop M, Brunt D, Pathare N, Patel B. The effect of velocity on the strategies used during gait termination. Gait & Posture. 2004;20:134–139. doi: 10.1016/j.gaitpost.2003.07.004. [DOI] [PubMed] [Google Scholar]
- Bruininks RH. Bruininks-Oseretsky test of motor proficiency: Examiner's manual. American Guidance Service; Circle Pines, Minnesota: 1978. [Google Scholar]
- Cesari P, Formenti F, Olivato P. A common perceptual parameter for stair climbing for children, young and old adults. Human Movement Science. 2003;22:111–124. doi: 10.1016/s0167-9457(03)00003-4. [DOI] [PubMed] [Google Scholar]
- Chinapaw MJ, Mokkink LB, van Poppel MN, van Mechelen W, Terwee CB. Physical activity questionnaires for youth: A systematic review of measurement properties. Sports Medicine. 2010;40:539–563. doi: 10.2165/11530770-000000000-00000. [DOI] [PubMed] [Google Scholar]
- Dempster WT. WADC Technical Report 55-159. Wright-Patterson Air Force Base. Carpenter Litho & Printing Co.; Ohio. Springfield, Ohio: 1955. Space requirements of the seated operator. Geometrical, kinematic, and mechanical aspects of the body with special reference to the limbs. [Google Scholar]
- Gallahue DL, Ozmun JC. Understanding motor development: Infants, children, adolescents, adults. 4th ed. McGraw Hill; Boston: 1998. [Google Scholar]
- Ganley KJ, Powers CM. Gait kinematics and kinetics of 7-year-old children: A comparison to adults using age-specific anthropometric data. Gait & Posture. 2005;21:141–145. doi: 10.1016/j.gaitpost.2004.01.007. [DOI] [PubMed] [Google Scholar]
- Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: Application to the knee. Journal of Biomechanical Engineering. 1983;105:136–144. doi: 10.1115/1.3138397. [DOI] [PubMed] [Google Scholar]
- Hallemans A, Beccu S, Van Loock K, Ortibus E, Truijen S, Aerts P. Visual deprivation leads to gait adaptations that are age- and context-specific: I. Step-time parameters. Gait & Posture. 2009;30:55–59. doi: 10.1016/j.gaitpost.2009.02.018. [DOI] [PubMed] [Google Scholar]
- Hase K, Stein RB. Analysis of rapid stopping during human walking. Journal of Neurophysiology. 1998;80:255–261. doi: 10.1152/jn.1998.80.1.255. [DOI] [PubMed] [Google Scholar]
- Jensen RK. Body segment mass, radius and radius of gyration proportions of children. Journal of Biomechanics. 1986;19:359–368. doi: 10.1016/0021-9290(86)90012-6. [DOI] [PubMed] [Google Scholar]
- Jian Y, Winter DA, Ishac MG, Gilchrist L. Trajectory of the body COG and COP during initiation and termination of gait. Gait & Posture. 1993;1:9–22. [Google Scholar]
- MacLellan MJ, Patla AE. Adaptations of walking pattern on a compliant surface to regulate dynamic stability. Experimental Brain Research. 2006;173:521–530. doi: 10.1007/s00221-006-0399-5. [DOI] [PubMed] [Google Scholar]
- McFadyen BJ, Malouin F, Dumas F. Anticipatory locomotor control for obstacle avoidance in mid-childhood aged children. Gait & Posture. 2001;13:7–16. doi: 10.1016/s0966-6362(00)00090-4. [DOI] [PubMed] [Google Scholar]
- Michel J, Grobet C, Dietz V, van Hedel HJA. Obstacle stepping in children: Task acquisition and performance. Gait & Posture. 2010;31:341–346. doi: 10.1016/j.gaitpost.2009.12.001. [DOI] [PubMed] [Google Scholar]
- Nor Aini J, Poh BK, Chee WS. Validity of a children's physical activity questionnaire (cPAQ) for the study of bone health. Pediatrics International. 2013;55:223–228. doi: 10.1111/ped.12035. [DOI] [PubMed] [Google Scholar]
- Pai YC, Lee WA. Effect of a terminal constraint on control of balance during sit-to-stand. Journal of Motor Behavior. 1994;26:247–256. doi: 10.1080/00222895.1994.9941680. [DOI] [PubMed] [Google Scholar]
- Pai YC, Maki BE, Iqbal K, McIlroy WE, Perry SD. Thresholds for step initiation induced by support-surface translation: A dynamic center-of-mass model provides much better prediction than a static model. Journal of Biomechanics. 2000;33:387–392. doi: 10.1016/s0021-9290(99)00199-2. [DOI] [PubMed] [Google Scholar]
- Pai YC, Patton J. Center of mass velocity-position predictions for balance control. Journal of Biomechanics. 1997;30:347–354. doi: 10.1016/s0021-9290(96)00165-0. [DOI] [PubMed] [Google Scholar]
- Pai YC, Rogers MW, Patton J, Cain TD, Hanke TA. Static versus dynamic predictions of protective stepping following waist-pull perturbations in young and older adults. Journal of Biomechanics. 1998;31:1111–1118. doi: 10.1016/s0021-9290(98)00124-9. [DOI] [PubMed] [Google Scholar]
- Patton JL, Pai Y, Lee WA. Evaluation of a model that determines the stability limits of dynamic balance. Gait & Posture. 1999;9:38–49. doi: 10.1016/s0966-6362(98)00037-x. [DOI] [PubMed] [Google Scholar]
- Rosengren KS, McAuley E, Mihalko SL. Gait adjustments in older adults: Activity and efficacy influences. Psychology and Aging. 1998;13:375–386. doi: 10.1037//0882-7974.13.3.375. [DOI] [PubMed] [Google Scholar]
- Schmitz KE, Hovell MF, Nichols JF, Irvin VL, Keating K, Simon GM, Jones KL. A validation study of early adolescents’ pubertal self-assessments. Journal of Early Adolescence. 2004;24:357–384. [Google Scholar]
- Sigward SM, Pollard CD, Havens KL, Powers CM. Influence of sex and maturation on knee mechanics during side-step cutting. Medicine and Science in Sports and Exercise. 2012a;44:1497–1503. doi: 10.1249/MSS.0b013e31824e8813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sigward SM, Pollard CD, Powers CM. The influence of sex and maturation on landing biomechanics: Implications for anterior cruciate ligament injury. Scandinavian Journal of Medicine and Science in Sports. 2012b;22:502–509. doi: 10.1111/j.1600-0838.2010.01254.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smyth MM, Anderson HI. Coping with clumsiness in the school playground: Social and physical play in children with coordination impairments. British Journal of Developmental Psychology. 2000;18:389–413. [Google Scholar]
- Snapp-Childs W, Bingham GP. The affordance of barrier crossing in young children exhibits dynamic, not geometric, similarity. Experimental Brain Research. 2009;198:527–533. doi: 10.1007/s00221-009-1944-9. [DOI] [PubMed] [Google Scholar]
- Sundermier L, Woolacott M, Roncesvalles N, Jensen J. The development of balance control in children: Comparisons of EMG and kinetic variables and chronological and developmental groupings. Experimental Brain Research. 2001;136:340–350. doi: 10.1007/s002210000579. [DOI] [PubMed] [Google Scholar]
- Sutherland D. The development of mature gait. Gait & Posture. 1997;6:163–170. [Google Scholar]
- USDHHS, US Department of Health and Human Services . Physical activity guidelines for Americans. US Department of Health and Human Services; Hyattsville, MD: 2008. p. 65. Hyattsville, MD: US Department of Health and Human Services. [Google Scholar]
- Vallis LA, McFadyen BJ. Children use different anticipatory control strategies than adults to circumvent an obstacle in the travel path. Experimental Brain Research. 2005;167:119–127. doi: 10.1007/s00221-005-0054-6. [DOI] [PubMed] [Google Scholar]
- Wilmut K, Barnett AL. Locomotor behaviour of children while navigating through apertures. Experimental Brain Research. 2011;210:185–194. doi: 10.1007/s00221-011-2614-2. [DOI] [PubMed] [Google Scholar]