

Abstract
In 2013, the Integrating the Healthcare Enterprise (IHE) Radiology workgroup developed the Management of Radiology Report Templates (MRRT) profile, which defines both the format of radiology reporting templates using an extension of Hypertext Markup Language version 5 (HTML5), and the transportation mechanism to query, retrieve, and store these templates. Of 200 English-language report templates published by the Radiological Society of North America (RSNA), initially encoded as text and in an XML schema language, 168 have been converted successfully into MRRT using a combination of automated processes and manual editing; conversion of the remaining 32 templates is in progress. The automated conversion process applied Extensible Stylesheet Language Transformation (XSLT) scripts, an XML parsing engine, and a Java servlet. The templates were validated for proper HTML5 and MRRT syntax using web-based services. The MRRT templates allow radiologists to share best-practice templates across organizations and have been uploaded to the template library to supersede the prior XML-format templates. By using MRRT transactions and MRRT-format templates, radiologists will be able to directly import and apply templates from the RSNA Report Template Library in their own MRRT-compatible vendor systems. The availability of MRRT-format reporting templates will stimulate adoption of the MRRT standard and is expected to advance the sharing and use of templates to improve the quality of radiology reports.
Keywords: Radiology reporting, Reporting, Structured reporting, Integrating the Healthcare Enterprise (IHE), Infrastructure, Standards, MRRT
Background
Effective communication of the results of radiological procedures is critical to high-quality health care. The use of itemized, structured reports—which present information in a consistent manner using a standardized vocabulary—is preferred by a majority of radiologists and referring clinicians [1]. Template-based radiology reports have been shown to improve communication, improve accuracy, and reduce certain types of errors [2–4]. Institutions are beginning to adopt standardized reporting templates throughout their radiology department [5].
To support the evaluation and adoption of structured reporting, the Radiological Society of North America (RSNA) developed a set of more than 200 radiology reporting templates [6]. The templates are freely available online (www.radreport.org), and since their initial release in 2009, they have been viewed or downloaded more than 1.8 million times. These templates were made available both as text documents for readability and in Extensible Markup Language (XML) for interoperability. The XML-format templates have been encoded using the Regular Language for XML–Next Generation (RELAX NG) schema language [7] (Fig. 1). Although RELAX NG is a standardized schema language, the RELAX NG templates were created before a standard for radiology reporting templates had been defined.
Fig. 1.
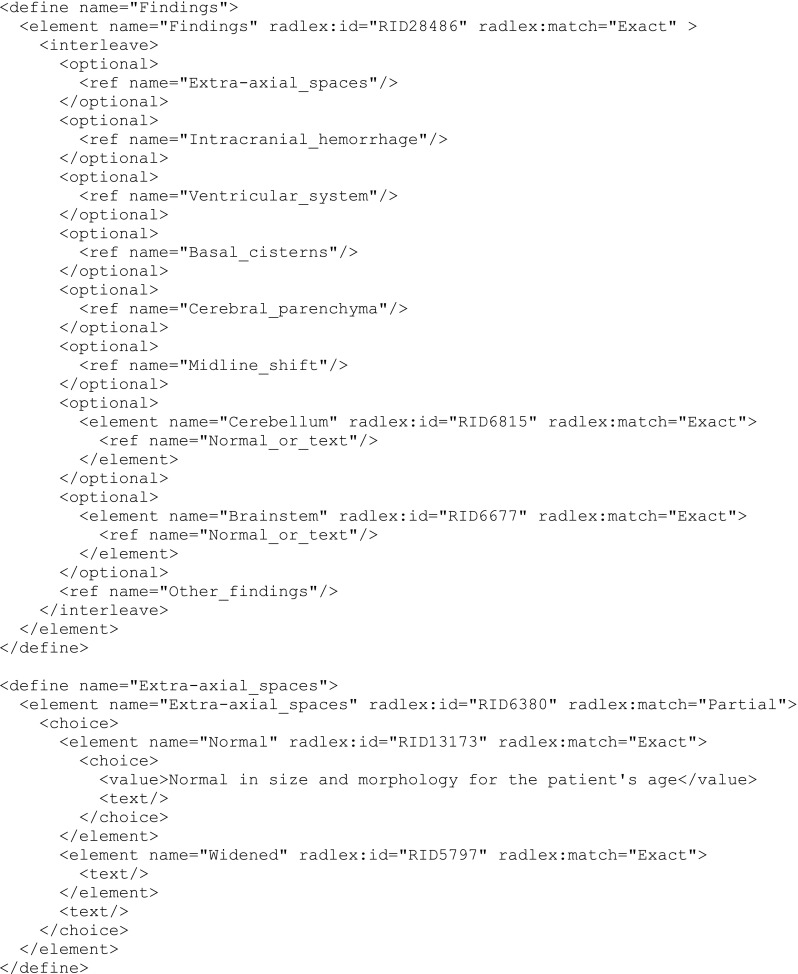
Part of the RELAX NG encoding of the CT Brain report template, showing the “Findings” section. Note that blocks such as “Extra-axial spaces” are incorporated by reference; the <ref> tag points to the block of RELAX NG code enclosed by the corresponding <define> tag
Integrating the Healthcare Enterprise (IHE) is an organization that promotes interoperability through the use of profiles that define common behavior between systems. The IHE Radiology workgroup developed the Management of Radiology Report Templates (MRRT) profile to specify a standardized approach for reporting templates [8]. The MRRT profile specifies the format of reporting templates using an extension of Hypertext Markup Language version 5 (HTML5) [9] and was approved for trial implementation in October 2013.
The IHE MRRT profile was developed to address the following issues with both the pre-existing RSNA template framework and existing reporting systems:
The existing RELAX NG format provides a method to encode structured observations linked to controlled terminology but does not easily accommodate narrative portions of a report template.
There is a need to import and export templates in many scenarios, such as facilitating their migration when reporting systems are replaced or when radiologists move to new organizations.
As RSNA and other organizations develop libraries where radiologists can find exemplary best-practice templates, a format that vendors accept can enable radiologists to begin using templates as soon as they are downloaded from a library.
Many reporting systems lack important features that radiologists need, such as fields that are filled from a menu, auto-fill and range checking of field values, user alerts when fields are incomplete, and annotation of report content with controlled terminology.
A standardized template format decouples template authoring and template use. Thus, reporting templates will not have to be created within the system where they will be used. It is expected that the MRRT standard will encourage the creation of template authoring tools that offer feature-rich interfaces.
The MRRT profile describes imaging report templates used by radiologists to guide the creation of a clinical diagnostic imaging report. The profile describes methods to format imaging report templates and to manage their transport between template libraries and report creation systems. The MRRT profile also describes an enhanced feature set for report authoring templates, delineates how such templates from a vendor-agnostic template library could be used immediately by a reporting system, and provides a format for migration of templates between reporting systems [9].
HTML5 was selected as the framework for the IHE MRRT profile because of its strength in communicating content with context, which, like report templates, entails not only the presentation of narrative text but also the description of user interface elements that accept user input. The MRRT format incorporates HTML5 custom data attributes using the “data-*” syntax, such as “data-field-type” (with values such as “NUMERIC”, “TEXT”, and “MERGE”) and “data-field-verbal-trigger” (to specify a word or phrase to direct the Report Creator actor software to the field). MRRT uses the “id” attribute to link a field or data item to coded content and the “title” attribute to provide a text description (“hint”) that a reporting system could display when a user’s mouse hovers over the item. The MRRT profile provides the ability to participate in workflows involving reporting systems (such as dictation and transcription services) through the use of the HTML5 metadata within the template.
Some of the MRRT design choices came directly from how the previous RELAX NG format functioned. For example, for metadata, both formats specify the use of Dublin Core metadata (dublincore.org). Dublin Core metadata allow authors and readers to identify each template’s title, authors, editor, creation and modification dates, sponsoring organizations, subspecialty codes, and indexing terms. These metadata are encoded in a uniform format that allows templates to be discovered and indexed easily by web-based agents. How the metadata are specified in the template, however, differs between RELAX NG and MRRT, and thus had to be converted.
The MRRT profile does not define how template-based reports are transmitted from a radiology reporting system to an electronic health record system. Supplement 155 of the Digital Imaging and Communication in Medicine (DICOM) Standard, currently in development, defines how MRRT-based reports are to be converted into HL7 Clinical Document Architecture (CDA) documents for transmission. Such work is beyond the scope of the MRRT profile and is not discussed in this article.
This manuscript describes the conversion of the RSNA template library’s reporting templates to the new MRRT profile and presents an evaluation of that process. We analyze the success in preserving references from reporting elements (data fields or their values) to terms in biomedical ontologies such as RadLex, a unified lexicon of radiology terms. In addition, we describe validation of the conversion process to ensure that the resulting HTML5 templates express the content of the original template and conform to the MRRT syntax.
Materials and Methods
Each RELAX NG-based radiology reporting template included a header section, which captured metadata about the template, and a body section, which captured the contents of the template itself. The template body incorporated references from the reporting elements to discrete terms in biomedical ontologies (vocabularies and knowledge models) such as the RadLex radiology lexicon [10, 11], Systematized Nomenclature of Medicine (SNOMED) Clinical Terms [12], and Logical Observation Identifier Names and Codes (LOINC) [13, 14]. One of the goals in converting the templates into the MRRT format was to preserve those coded references. Figure 2 summarizes the conversion process.
Fig. 2.

Schematic diagram depicts the semi-automated process of converting the reporting templates into MRRT. The manual editing and editorial review steps required expertise in radiology and/or HTML5
The initial approach employed an Extensible Stylesheet Language Transformation (XSLT) script (www.w3.org/TR/xslt) to transform the XML-format templates into HTML5 documents (Fig. 3). Because XSLT lacked the ability to facilitate discovery, retrieval, and on-the-fly customization of reporting templates, a subsequent approach extended a prototype system built for real-time display of reporting templates [15]. This second approach utilized a Representational State Transfer (REST) interface [16] with an XML parsing engine to deconstruct each RELAX NG template into its individual components. The XML parsing engine applied a Java servlet and JavaScript Object Notation (JSON) to convert templates into MRRT format. This approach allowed the process to be adjusted to accommodate idiosyncrasies in the original templates.
Fig. 3.

Portion of the XSLT stylesheet used to transform a RELAX NG reporting template into MRRT
The MRRT profile uses HTML5 extensions, such as tags and attributes, to express report templates in HTML5. Some of these extensions, although valid in HTML5, are not visible in a standard web browser. Unlike standard HTML5, the MRRT profile requires all HTML5 tags to have corresponding closing tags (e.g., </input>) so that the report template can be validated as an XML document. Although the report templates are expressed in HTML5, HTML is simply a convenient method to express the concepts in the template. The MRRT profile’s “Report Creator” actor, which presents the templates to the radiologist and uses them to create report instances, is not required to use an HTML rendering engine. Internal and external CSS style sheets may be used to render these templates; inline styles are not permitted. The MRRT standard required several changes to the report template data-input fields. Some examples of this include:
Numeric data fields—which were specified as either integer or floating-point values in RELAX NG, were converted to floating-point “number” fields. The optional “step” attribute was used to specify the precision; e.g., step = “1” specifies an integer value.
A “merge” field allowed the reporting system to incorporate external data, such as measurements from an imaging device, calculations from a script within the template, or information from an external web service.
Fields in which the user selected among a set of fixed responses (“pick lists”) were converted from <choice> tags in RELAX NG into the MRRT format.
The MRRT format also lacks some of the constructs in RELAX NG, such as the ability to define repeated sections in a report, which are specified in RELAX NG with <zeroOrMore> or <oneOrMore> tags.
After automated conversion and manual editing, the templates underwent editorial review and technical validation. The templates were reviewed by two radiologists, each with more than 20 years of experience in radiology and medical informatics. The syntax validation process consisted of two components: one each for HTML5 and MRRT. The templates were validated for proper HTML5 syntax using the World Wide Web Consortium (W3C) Validator service (validator.w3.org). The templates were validated for correct MRRT syntax using a document schema developed by the authors in the RELAX NG compact schema language (Fig. 4) and applied using a validation web service (html5.validator.nu).
Fig. 4.

MRRT header section for the CT Brain reporting template. Note the Dublin Core metadata
Results
The automated transformation process maintained the sequential order and hierarchical relationships of concepts in the reporting templates and successfully preserved references to RadLex, SNOMED CT, and LOINC terms. This process completely preserved the Dublin Core metadata that appeared in the template header section (Fig. 5).
Fig. 5.

Conversion of RELAX NG to MRRT. Corresponding portions of the template for CT Brain show how the RELAX NG code for the report element “Cerebellum” has been converted. The upper panel shows the RELAX NG encoding, in which the data element incorporate a <choice> tag that allows either the element “Normal” or free text. The RadLex IDs for the terms Cerebellum (RID6815) and Normal (RID13173) are shown. The lower panel shows the <head> and <body> sections of the corresponding MRRT document. Note that the RadLex code for “Cerebellum” is preserved in the <coded_content> section of the document header, but not the encoding for “Normal.”
Almost all of the initial templates included mappings of their reporting elements to RadLex terms, and many had terms mapped to SNOMED CT and LOINC as well. These mappings were preserved, although the serialization of data elements in MRRT required some terms to be repeated. In RELAX NG, mappings to terminologies were defined “inline” as attributes in the <element> tag (Fig. 6). In contradistinction, mappings to terminologies such as RadLex are encoded in MRRT by linking the data-entry elements of the template document’s body with code specifications within the <coded_content> block of the document header. For example, many of the RELAX NG templates used a construct that allowed a radiologist to choose the value “Normal” (possibly with a pre-defined text string) or to enter a text value. In converting such templates, the code for the default value (“Normal”) was lost, and there was not a way to specify the ontological reference properly. A Change Proposal to the MRRT standard is under consideration to specify coded content for default text values; thus, if the default value is left unaltered, the input field can be assigned the corresponding code value (such as RID13173, “Normal”).
Fig. 6.

A portion of a schema for MRRT, written in RELAX NG compact syntax, used to validate the syntax of converted templates
For most templates, manual review was needed to optimize the templates in the MRRT format. Each template required 5 to 45 min of manual editing. The conversion effort required an understanding of how the templates would be used in a clinical setting. Subheadings within the Findings section were added manually to make longer templates easier to navigate and use. Some data elements were converted from pick lists to text fields with a default value. In some templates, for example, a pick-list field for Ascites with values of None, Mild, Moderate, or Severe was converted to a text field with default value “None.” Although such changes reduce the structured data available from reports based on the template, such an approach reduced the overall complexity of the reporting templates. The MRRT-format CT Brain template is shown in Figs. 7 and 8.
Fig. 7.

MRRT encoding of part of the Findings section of the CT Brain reporting template
Fig. 8.

The MRRT-encoded CT Brain reporting template, as rendered in a web browser. MRRT uses HTML5 to allow viewing of data-entry elements in a web browser but does not require that a clinical reporting system support web browser capabilities
The converted templates were uploaded to the template library web site, where they have superseded the prior RELAX NG templates. The latter is still available from the template library, but once an MRRT template has been uploaded, there is no longer a link from the template page to the script that presents the template in RELAX NG. The original RELAX NG templates still can be downloaded; for example, to download the “CT Brain” template (template #4), one can use the URL “http://www.radreport.org/xml/4”.
Discussion
The RSNA reporting templates were converted successfully into the MRRT template format and validated for proper HTML5 and MRRT syntax. These templates conform to a format accepted by the international healthcare information standards-setting community. The semi-automated approach allowed editorial decisions to balance the complexity and usability of the templates in a clinical setting. An important consideration in implementing report templates throughout a department is to assure that they are not unnecessarily complex [5]. The incorporation of “voice triggers” and audible prompts for the report’s data-entry fields into a reporting system can help radiologists by reducing the need to look away from the images being interpreted [17]. Such features are available in MRRT templates.
Semi-automated conversion of the templates offered advantages and disadvantages over fully manual translation. Our process preserved the template metadata, such as the template’s title, contributors, and indexing codes, and maintained the data-entry fields’ previously identified references to RadLex, SNOMED CT, and LOINC terms. The data-entry fields were generated by the conversion process. Headers that demarcated the major sections of the report template, such as “Clinical information” and “Findings,” were converted automatically. Subsection headers, such as might appear within the Findings section of a report template, required manual editing. Common RELAX NG constructs that allowed a user to enter a default value (e.g., “Normal”) or free text were converted into two data-entry fields; they had to be edited manually into a single text field with the specified default value. Overall, the semi-automated conversion process was judged to be effective.
An open-source, web-based editing tool to create and edit reporting templates and their metadata has been developed (www.karoshealth.com/resources/report-template-editor). This tool promises to simplify the effort to edit MRRT-format templates and manage the template metadata in a graphical WYSIWYG (“what you see is what you get”) environment. Given recent evidence that most academic radiology departments are using or experimenting with structured reports [18], the availability of this editing tool and a set of freely available MRRT-format templates should help support the growing interest in structured reporting.
The availability of report templates in the MRRT format encourages manufacturers to develop software that can consume these templates and should help radiologists share their best-practice templates with each other across organizations. By using MRRT transactions and MRRT-format templates, radiologists will be able to directly import and apply templates from the RSNA Report Template Library in their own systems. MRRT is now the standard for reporting templates. Going forward, it is expected that reporting templates will be developed directly in MRRT. It is anticipated that the standardization and dissemination of reporting templates will engender innovation and improvement in the reporting process [19]. Such changes seek to improve the completeness, clarity, and usefulness of clinical radiology reports to the benefit of patients and referring clinicians.
Acknowledgments
The authors thank Gerald Cameron, MS, for the development of the conversion and validation algorithms.
References
- 1.Bosmans JM, Weyler JJ, De Schepper AM, Parizel PM: The radiology report as seen by radiologists and referring clinicians: results of the COVER and ROVER surveys. Radiology 259:184–195, 2011 [DOI] [PubMed]
- 2.Schwartz LH, Panicek DM, Berk AR, Li Y, Hricak H: Improving communication of diagnostic radiology findings through structured reporting. Radiology 260:174–181, 2011 [DOI] [PMC free article] [PubMed]
- 3.Lin E, Powell D, Kagetsu N. Efficacy of a checklist-style structured radiology reporting template in reducing resident misses on cervical spine computed tomography examinations. J Digit Imaging. 2014;27:588–593. doi: 10.1007/s10278-014-9703-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hawkins CM, Hall S, Zhang B, Towbin A. Creation and implementation of department-wide structured reports: an analysis of the impact on error rate in radiology reports. J Digit Imaging. 2014;27:581–587. doi: 10.1007/s10278-014-9699-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Larson DB, Towbin AJ, Pryor RM, Donnelly LF: Improving consistency in radiology reporting through the use of department-wide standardized structured reporting. Radiology 267:240–250, 2013 [DOI] [PubMed]
- 6.Kahn Jr, CE, et al: Toward best practices in radiology reporting. Radiology 252:852–856, 2009 [DOI] [PubMed]
- 7.Bozkurt S, Kahn Jr, CE: An open-standards grammar for outline-style radiology report templates. J Digit Imaging 25:359–364, 2012 [DOI] [PMC free article] [PubMed]
- 8.Hempel JM, Pinto dos Santos D, Kloeckner R, Dueber C, Mildenberger P: [Reporting initiatives. An update on treatment in radiology]. Radiologe 54:696–699, 2014 [DOI] [PubMed]
- 9.Management of Radiology Report Templates (MRRT). Available at http://www.ihe.net/uploadedFiles/Documents/Radiology/IHE_RAD_Suppl_MRRT.pdf. Accessed 20 October 2014, 2014
- 10.Langlotz CP: RadLex: a new method for indexing online educational materials. RadioGraphics 26:1595–1597, 2006 [DOI] [PubMed]
- 11.Rubin DL. Creating and curating a terminology for radiology: ontology modeling and analysis. J Digit Imaging. 2008;21:355–362. doi: 10.1007/s10278-007-9073-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.SNOMED CT. Available at http://www.ihtsdo.org/snomed-ct/. Accessed July 24, 2013, 2013
- 13.Huff SM, et al. Development of the Logical Observation Identifier Names and Codes (LOINC) vocabulary. J Am Med Inform Assoc. 1998;5:276–292. doi: 10.1136/jamia.1998.0050276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McDonald CJ, et al. LOINC, a universal standard for identifying laboratory observations: a 5-year update. Clin Chem. 2003;49:624–633. doi: 10.1373/49.4.624. [DOI] [PubMed] [Google Scholar]
- 15.Genereaux BW, Dennison DK. REST enabling the report template library. J Digit Imaging. 2014;27:331–336. doi: 10.1007/s10278-013-9668-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fielding RT, Taylor RN. Principled design of the modern Web architecture. ACM Trans Internet Technol. 2002;2:115–150. doi: 10.1145/514183.514185. [DOI] [Google Scholar]
- 17.Sistrom CL. Conceptual approach for the design of radiology reporting interfaces: the talking template. J Digit Imaging. 2005;18:176–187. doi: 10.1007/s10278-005-5167-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Powell DK, Silberzweig JE: State of structured reporting in radiology, a survey. Acad Radiol 22:226–233, 2015 [DOI] [PubMed]
- 19.Li KC, et al. Digitization of medicine: how radiology can take advantage of the digital revolution. Acad Radiol. 2013;20:1479–1494. doi: 10.1016/j.acra.2013.09.008. [DOI] [PubMed] [Google Scholar]