

Abnormalities in diastolic function are more sensitive than changes in the left ventricular ejection fraction for detecting acute cardiotoxicity and are related to the dose-volume of the heart irradiated in patients with left-sided breast cancer receiving radiotherapy with trastuzumab, highlighting the importance of decreasing the dose-volume as a protective strategy. Therefore, diastolic dysfunction should be incorporated as a routine parameter in the monitoring of cardiotoxicity.
Keywords: Diastolic dysfunction, Breast cancer, Radiotherapy, Trastuzumab, Concurrent treatment
Abstract
Background.
Left ventricular ejection fraction (LVEF) is used routinely to monitor cardiac dysfunction associated with breast cancer treatment. In this study the prevalence of early left ventricular diastolic dysfunction (LVDD) and its relationship to the dose-volume of the heart irradiated were evaluated in HER2-positive breast cancer patients undergoing concurrent trastuzumab and adjuvant radiotherapy (RT).
Materials and Methods.
Data from 40 breast cancer patients treated with concurrent trastuzumab and left-sided adjuvant RT between September 2011 and October 2012 were collected prospectively. For comparison, 32 patients treated with concurrent trastuzumab and right-sided adjuvant RT and 71 patients treated with left-sided RT alone were collected retrospectively. Echocardiography was obtained before RT, immediately following RT, and 3 and 6 months after RT. Doses to the heart and left ventricle (LV) were quantified.
Results.
Prior to RT with concurrent trastuzumab, 11 of 29 (left) and 8 of 25 (right) patients with normal baseline left ventricular diastolic function (LVDF) developed LVDD. In patients receiving left-sided RT alone, 12 of 61 patients with normal baseline LVDF developed LVDD. Dmean, D15–D40, D60–D70, and V3–V10 of the LV were significantly higher in patients who developed LVDD after concurrent trastuzumab and left-sided RT. In contrast, only two patients developed grade 1 LVEF decrease after both concurrent treatment and left-sided RT alone.
Conclusion.
Changes in LVDF compared with LVEF are more sensitive for early detection of cardiotoxicity. The dose-volume of the heart contributes significantly to the risk of LVDD in patients with left-sided breast cancer treated concurrently with trastuzumab.
Implications for Practice:
Abnormalities in diastolic function are more sensitive than changes in the left ventricular ejection fraction for detecting acute cardiotoxicity and are related to the dose-volume of the heart irradiated in patients with left-sided breast cancer receiving radiotherapy concurrently with trastuzumab. This result highlights the importance of decreasing the dose-volume of heart irradiated as a protective strategy in the treatment setting of concurrent trastuzumab and radiotherapy. Diastolic dysfunction may serve as a more sensitive tool for the early detection of cardiac damage and should be incorporated as a routine parameter in the functional monitoring of cardiotoxicity.
Introduction
Cardiotoxicity is a well-known complication following cancer treatment, including chemotherapy, targeted therapy, endocrine therapy, and radiotherapy (RT). In patients receiving breast conservative surgery or high-risk patients receiving mastectomy, RT is an important therapeutic component that significantly reduces the risk of recurrence and breast cancer mortality [1]. However, long-term follow-up has shown that the survival benefit from RT was partially counterbalanced by an increased risk of death from cardiac events [1]. Although improvements in RT technology have allowed for better protection of the heart and less cardiotoxicity [2–5], considering anatomical position, the risk of cardiac damage remains a major concern in patients with left-sided breast cancer.
Between 20 and 25% of breast cancers overexpress human epidermal growth factor receptor 2 (HER2), and these patients have a poor prognosis [6]. Trastuzumab (Herceptin; Roche, Basel, Switzerland, http://www.roche.com), a humanized monoclonal antibody against the extracellular domain of HER2, in combination with RT has been shown to significantly extend disease-free progression and survival in this subgroup of breast cancer patients [7]. However, similar to RT, trastuzumab detrimentally impacts cardiac function [7]. Preclinical data suggest a radiosensitizing effect of trastuzumab on breast cancer cells [8, 9]. Although it is not yet clear whether it causes radiosensitization of normal cells, the major concern remains the potential synergistic effect of concurrent trastuzumab and RT on heart involved in the radiation field.
Monitoring of cardiac function is considered to be of critical importance for preventing treatment-related cardiac events in these patients. Serial measurement of left ventricular ejection fraction (LVEF) is the most widely used approach. However, because of the cardiac contractility reserve, LVEF may be insensitive for detecting minor cardiac damage. Left ventricular diastolic dysfunction (LVDD), on the other hand, has demonstrated sensitivity as an early sign of functional abnormality in several cardiac pathologies, including those related to cancer treatment [10–13].
It has been established that radiation-related cardiotoxicity is dose-dependent [14]. Furthermore, our previous study showed that left-sided irradiation with increased low dose-volume was associated with increased left ventricular systolic dysfunction after concurrent treatment with trastuzumab [15]. It still remains unclear how radiation dose to the heart might alter cardiac diastolic function when RT is administered concurrently with trastuzumab. In this study, we prospectively evaluated a cohort of breast cancer patients for treatment-related cardiotoxicity. Our goal was first to determine the prevalence of LVDD in the setting of concurrent treatment and second to identify any relationship between dose-volume of cardiac structures irradiated and LVDD in these patients.
Materials and Methods
Patients
A series of 40 women receiving concurrent treatment of trastuzumab and adjuvant RT for clinical stage I/III [16] left-sided breast cancer between September 2011 and October 2012 were prospectively collected. For comparison, 32 patients treated with concurrent trastuzumab and right-sided adjuvant RT together with 71 patients treated with left-sided RT alone were collected retrospectively within the same period. Patients with HER2 overexpression (defined as immunohistochemistry score of 3 or fluorescence in situ hybridization positive) were eligible for adjuvant trastuzumab for 1 year if they had node-positive or high-risk node-negative disease. Patients with cardiac disease or LVEF below 50% prior to RT were excluded from this study.
A total of 22 patients with a primary diagnosis of stage IIA–IIIA disease received neoadjuvant chemotherapy. All but 8 of the 143 patients received adjuvant chemotherapy. The decision of adjuvant chemotherapy was made by a multidisciplinary breast cancer team consisting of surgeons, medical oncologists, radiation oncologists, and pathologists. Trastuzumab was delivered once every 3 weeks concurrently with RT. Endocrine therapy was given to patients with hormone receptor (HR)-positive breast cancers as determined by immunohistochemistry (≥10% positive). Demographic data and potential cardiac risk factors were collected, such as body mass index, smoking history, and relevant comorbidity in addition to the treatment details of each patient.
Radiation Therapy and Cardiac Dose Collection
Dose prescription was 50 Gy in 25 fractions over 5 weeks. A boost of 10 Gy in 5 fractions over 1 week was delivered to the tumor bed using electron beams following whole breast irradiation. All patients underwent computed tomography simulation in a supine position, immobilized on a breast board (Med-Tec, Inc. Orange City, IA, http://www.medtec.com) with both arms abducted and raised overhead. For chest wall RT, field-in-field forward-planned intensity-modulated radiotherapy (FiF-IMRT) was used [17]. Breast RT was performed with simplified multifield inverse-planned IMRT (sIMRT). sIMRT constraints were defined as follows: beam directions ≤ 5, segment size ≥ 10 cm2, and monitor units per segment ≥ 10 [18]. For left-sided tumors, the constraints of the heart were defined as follows: mean heart dose (Dmean) ≤8 Gy, and ≤10 Gy if internal mammary nodes were included, V30 ≤ 5%. Field borders of tangent fields and delineation of target fields were arranged according to the Radiation Therapy Oncology Group definition [19]. Supraclavicular and internal mammary chain lymph nodes were irradiated at the discretion of the radiation oncologist. No scar boost was used in patients receiving chest wall RT.
The heart and left ventricle (LV) were delineated according to a recently validated heart atlas [20]. The dose-volume histogram (DVH) parameters of the heart and LV were calculated using individual dose distribution data in the RT planning system (ADAC Pinnacle 3, version 8.0m). The DVH parameters of the heart and the LV were collected and included the minimum dose reaching relative volume levels ranging from 1% to 95% (D1 to D95) and the relative volume receiving dose levels ranging from 1 Gy to 50 Gy (V1 to V50). The mean cardiac dose received from supraclavicular lymph node field irradiation has been reported to be 0.3-0.8 Gy for left-sided fields [21]. The contribution of the tumor bed boost dose to the heart dose was also very low [22]. Thus, adjustments for cardiac dose were not carried out for patients treated with supraclavicular lymph node or tumor bed boost irradiation.
Echocardiography
Echocardiographic examination was conducted on all patients at rest and lying on the left side with the GE Vivid 7 and M3S probe at a harmonic mode of 1.7/3.4 MHz (GE Healthcare, Milwaukee, WI, http://www.gehealthcare.com). The transthoracic technique was used. All parameters were measured twice, and the average value was recorded. Left ventricular diastolic parameters were evaluated by pulsed-wave Doppler and tissue Doppler techniques. The maximum early diastolic mitral flow velocity (E) and maximum late diastolic mitral flow velocity (A) were determined by pulsed-wave Doppler. The early diastolic mitral annular velocity (Em), late diastolic mitral annular velocity (Am), and peak myocardial sustained systolic velocity (Sm) were all evaluated by tissue Doppler. M-mode echocardiography was used to measure left ventricular end-systolic diameters and end-diastolic diameters. LVEF was calculated using a modified Simpson’s method [23].
Assessment of Cardiac Function
Baseline cardiac function was assessed by echocardiography immediately before the start of RT. This assessment by echocardiography, along with the clinical assessment of cardiac function, was also performed immediately following completion of RT, as well as at 3 and 6 months afterward.
LVDD was diagnosed when the E/Em ratio was ≥15, according to current recommendations [24]. For patients with a value of E/Em ratio within the range of 8–15, accessory criteria were used based on evaluation of the mitral inflow profile. When the effect of age on the normal E/A ratio was taken into account, LVDD was defined in patients <45 years as an E/A ratio <1.0, whereas in patients ≥45 years, LVDD was defined as an E/A ratio <0.6 or >1.5. Left ventricular systolic dysfunction was evaluated according to the National Cancer Institute Common Toxicity Criteria (version 2.0; 1999).
Statistical Analysis
Descriptive analysis was performed using proportion (for categorical variables) and median with range (for quantitative variables). Comparison of cardiac function parameters within each group versus baseline was realized using repeated measures analysis of variance. Differences between groups were assessed using the χ2 test (or Fisher’s exact test) for categorical variables and the Mann-Whitney U test for quantitative variables. Comparison between groups for dosimetric details was analyzed using the Student’s t test. Dosimetric parameters were analyzed for correlation with LVEF decrease using Spearman’s rank correlation. A stepwise backward procedure was used to construct a set of independent risk factors of LVDD. All factors achieving a p value of <.10 were considered and sequentially removed if the p value in the multiple models was >.05. All p values were two-sided, and p < .05 was considered significant. SPSS software version 16.0 was used (2007; SPSS Inc., Chicago, IL, http://www-01.ibm.com/software/analytics/spss/).
Results
Patients and Treatment
Clinical features of the 143 patients are summarized in Table 1. Neoadjuvant chemotherapy was administrated according to the following schedule: four cycles of carboplatin and paclitaxel in 10 patients and in addition with trastuzumab in 12 patients, given at days 1, 8, and 15 of a 28-day cycle. In the 12 patients, trastuzumab was continued with a standard weekly dose with no interruption during neoadjuvant chemotherapy.
Table 1.
Patient and treatment characteristics
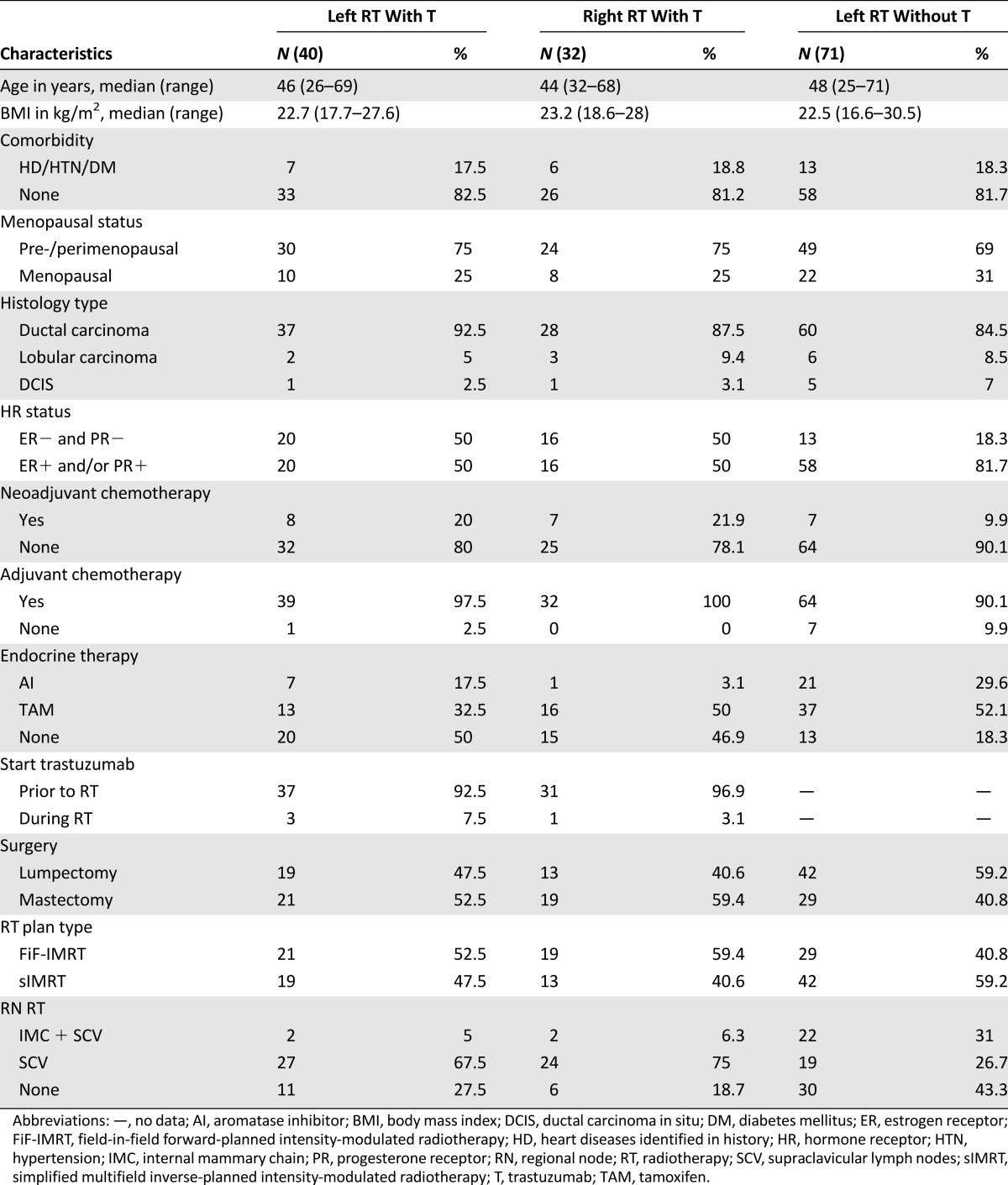
In 72 patients receiving concurrent trastuzumab and RT, all patients underwent adjuvant chemotherapy with the exception of 1 patient who achieved a complete pathologic response after neoadjuvant chemotherapy. Adjuvant chemotherapy was anthracycline-based in 57 patients (79.2%) with trastuzumab and 56 patients (78.9%) without trastuzumab. Only one right-sided patient received anthracycline and trastuzumab concurrently in the adjuvant setting. All patients completed their planned RT without interruption. Endocrine therapy was administered to all HR-positive patients following completion of RT.
Follow-Up of Cardiac Function
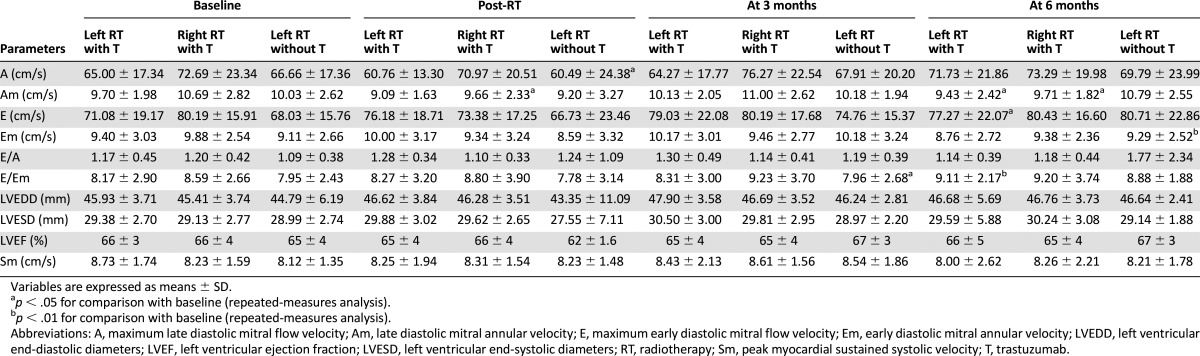
Changes in diastolic function of patients during follow-up are displayed in Table 2. Echocardiographic parameters of diastolic function including A, Am, E, Em, and the ratio of E to Em (E/Em) differed significantly over time during follow-up. In contrast to diastolic function, no significant change was observed in echocardiographic parameters for left ventricular systolic function (LVEF, Sm) at any post-RT time point.
Table 2.
Evolution of echocardiographic parameters before and after concurrent treatment of RT and trastuzumab
Prior to RT with concurrent trastuzumab, only 29 of 40 patients with left-sided tumors (72.5%) and 25 of 32 patients with right-sided tumors (78.1%) presented with normal left ventricular diastolic function (LVDF). In the left-sided group, 11 of 29 patients (37.9%) developed LVDD during the follow-up. For patients with right-sided tumors, 8 of 25 patients (32%) developed LVDD. The chemotherapy was anthracycline-based in 8 of 29 patients with left-sided RT and in 21 of 25 patients with right-sided RT (p < .0001). There was no significant difference in time from the completion of adjuvant chemotherapy to the start of RT between patients with and without LVDD in these two groups. At the visit 6 months after completion of RT concurrent with trastuzumab, only 5 of 11 patients with left-sided tumors and 4 of 8 patients with right-sided tumors recovered normal LVDF.
In patients treated with left-sided RT alone, baseline LVDF was normal in 61 of 71 patients (85.9%). Of those 61 patients, 12 (19.7%) developed LVDD during follow-up. At the visit 6 months after completion of RT, 6 of 12 patients recovered normal LVDF.
The median baseline LVEF was 67% (range: 59%–75%) and 66% (range: 57%–76%) in patients treated with left-sided and right-sided RT concurrently with trastuzumab, respectively. During follow-up, the median LVEF decrease from baseline to the lowest value was 2.5% (range: 10% decrease to 7% increase) and 3.0% (range: 16% decrease to 11% increase) after left-sided and right-sided RT with concurrent trastuzumab, respectively. One patient developed grade 1 LVEF decrease with concurrent trastuzumab in the left-sided and right-sided group, respectively. In patients treated with left-sided RT alone: the median baseline LVEF was 66% (range: 53%–73%); the median LVEF decrease from baseline to the lowest value was 0% (range: 11% decrease to 13% increase). Two patients developed grade 1 LVEF decrease. All 4 of these patients recovered normal LVEF at the visit 6 months after completion of RT. No patient developed congestive heart failure.
Cardiac Risk Factors in Patients With Concurrent Treatment
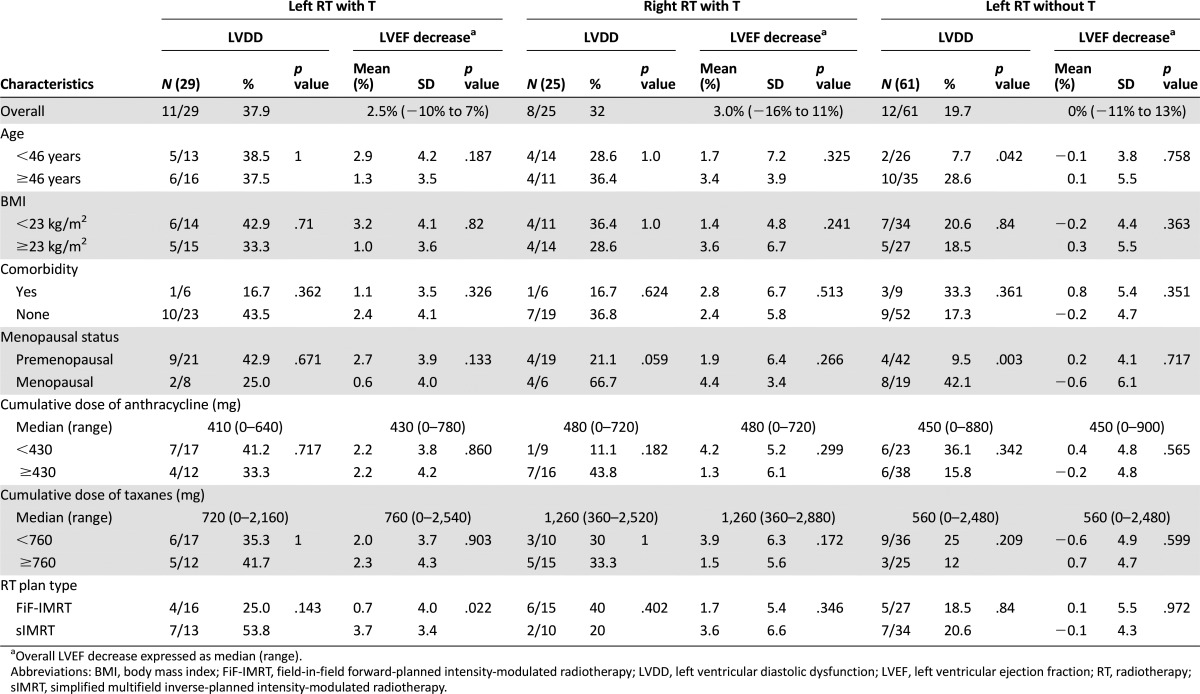
Univariate analysis tested the effect of patient- and treatment-related factors on the frequency of LVDD and LVEF decrease during the follow-up (Table 3). In patients receiving left-sided RT with concurrent trastuzumab, RT plan type was found to be the only significant factor affecting LVEF. The proportion of patients exhibiting LVDD was also higher when sIMRT was used compared with FiF-IMRT (53.8% and 25%, respectively), although these differences were not statistically significant. Age and menopausal status were significant risk factors of LVDD in patients treated with left-sided RT alone. In patients receiving concurrent treatment of right-sided RT and trastuzumab, menopausal status was a borderline significant risk factor of LVDD (p = .059).
Table 3.
Univariate analyses of left ventricle diastolic dysfunction and LVEF decrease after concurrent trastuzumab and RT
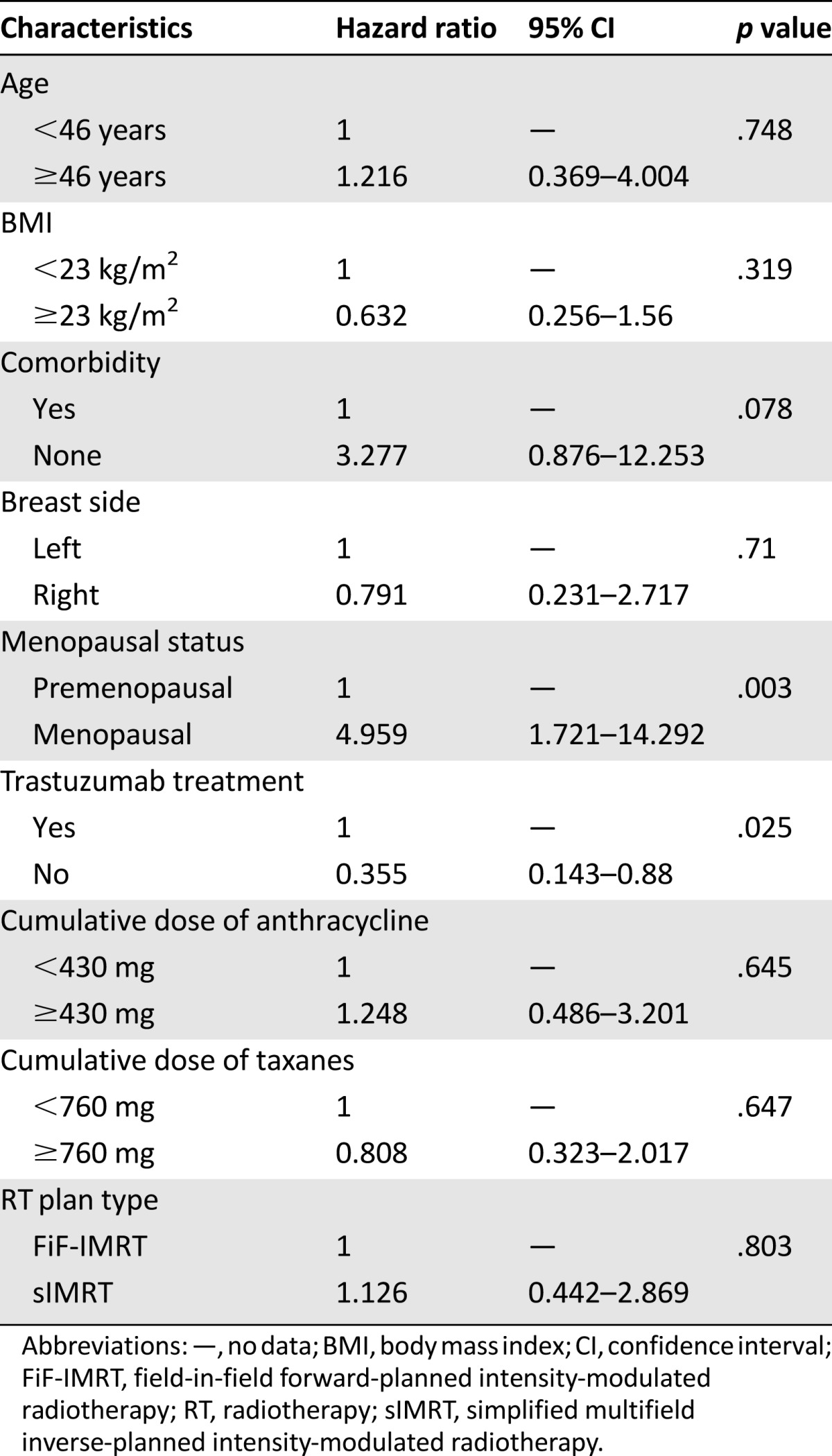
Multivariate analysis for risk factors of LVDD in all 143 patients (Table 4) showed that trastuzumab treatment and postmenopausal status were significantly associated with increased risk of LVDD. No significant difference in the risk of LVDD existed between patients treated with left-sided and right-sided RT.
Table 4.
Multivariate analysis of cardiac risk factors for left ventricle diastolic dysfunction after RT
Effect of Radiation Dose and Volume on Cardiac Dysfunction in Patients With Concurrent Treatment
The overall value of dose-volume parameters was significantly higher in left-sided patients (p < .0001). Among the 29 patients with normal baseline LVDF treated with concurrent left-sided RT and trastuzumab, the dose-volume of both the heart and LV was higher in the 11 patients who developed LVDD compared with those who did not (Fig. 1). Further analysis of the average value of dosimetric parameters indicated that the dose-volume of the LV, Dmean, D15–D70, and V3–V7 were significantly increased in patients who developed LVDD relative to those who did not (p < .05). No significant difference in the dosimetric parameters of the heart between patients with and without LVDD was found.
Figure 1.

Diastolic dysfunction of treated patients correlates with the dose-volume of heart irradiated. (A–D): Averages of Dn (Gy) of heart (A) and LV (B) and averages of Vn (%) of heart (C) and LV (D) in patients with normal baseline left ventricular diastolic function.
Abbreviations: Dn, minimum dose that reached at least n percentage of volume; LV, left ventricle; Vn, percentage of volume receiving at least n Gy.
Spearman’s rank correlation was performed to verify the effect of radiation dose and volume on LVEF decreases in all 40 patients treated with concurrent left-sided RT and trastuzumab. Significant correlations of the dose-volume of the heart were found between the decrease in LVEF and Dmean, D10–D95, and V1–V15 (p < .05, data not shown). Dmean, D20–D95, and V1–V10 of the LV were all also well correlated with LVEF decrease (p < .05, data not shown). For right-sided RT, no significant impact of the dose-volume of both the heart and LV was found on the risk of LVDD and LVEF decrease.
Comparison of cardiac dosimetric parameters between sIMRT and FiF-IMRT techniques showed that the average values of the Dmean, D10–D95, and V1–V15 of the heart were significantly higher in patients receiving sIMRT. Likewise, a continuous increase of Dmean, D20–D95, and V1–V10 for the LV was also statistically significant in patients treated by sIMRT (p < .05). Meanwhile, V40–V50 of the heart and V35–V45 of the LV for sIMRT were significantly lower than for FiF-IMRT (p < .05).
Discussion
To the best of our knowledge, this work represents one of the first studies to evaluate early LVDD in the setting of adjuvant RT for breast cancer. Our study revealed a high prevalence of LVDD in both patients treated with concurrent trastuzumab and RT and left-sided RT alone. A correlation between the dose-volume of irradiated cardiac structures and early LVDD was also found in patients with left-sided tumor receiving concurrent trastuzumab and RT.
Refinement of modern RT technique seems to have significantly reduced the risk of cardiac dysfunction. However, cardiac function assessment is still focused largely on systolic rather than diastolic dysfunction in breast cancer patients. In our study, the frequency of diastolic dysfunction was found to be much higher than that of systolic dysfunction whether after concurrent treatment (35.2% versus 2.8%, respectively) or after left-sided RT alone (19.7% versus 2.7%). Although the prevalence of late left ventricular diastolic dysfunction has been reported to be higher than that of systolic dysfunction after chest irradiation [25], data of early LVDD associated with trastuzumab or breast cancer RT is currently lacking. In other studies, myocardial perfusion defects have been reported to be the main cardiac event after breast cancer RT in short-term follow-up. Hardenbergh et al. [26] reported that 60% of patients receiving irradiation to the chest wall for left-sided breast cancer developed new perfusion defects during a follow-up 6 months after RT, whereas only a single patient developed a decrease in LVEF greater than 10% from baseline within the same time frame. At 6, 12, 18, and 24 months after RT, such perfusion defects could still be observed [3]. Although the clinical significance of perfusion defects subsequent to early myocardial capillary damage is unclear, these defects may eventually lead to myocardial fibrosis and ultimately, diastolic dysfunction [27].
In this study, we found a higher prevalence of LVDD in patients receiving concurrent treatment than RT alone, although the difference was not statistically significant (35.2% versus 19.7%, p = .061). The major mechanism proposed for trastuzumab-associated cardiac toxicity is that blocking HER2 has a negative impact on the response of the heart to stress and myocardial damage [28, 29]. Lack of resistance to stresses within the HER2-blocked myocardium may lead to amplified signs of injury, especially when cardiotoxic agents, such as anthracycline and irradiation, are administered in combination with trastuzumab [28, 30]. However, cardiac complications did not seem to be consistently increased when trastuzumab was delivered concurrently with adjuvant RT in previous studies [31–33]. Given the fact that radiation-related cardiotoxicity tends to appear after more than 10 years of follow-up, relatively short follow-up may prevent existing studies from reflecting clinically significant cardiac events. At the same time, in almost all clinical studies to date in which subclinical cardiac toxicity was assessed, LVEF was the only surrogate. Because LVEF is a less sensitive measure of cardiac function, cardiotoxicity may be substantially underestimated in breast cancer patients. Diastolic dysfunction as a potential sensitive surrogate might help to detect more subclinical cardiac toxicity and therefore to identify patients at high risk.
Cardiac diastolic function represents a complex interplay of physiologic events. Among these are the two major determinants of left ventricular filling: ventricular relaxation and chamber compliance [34]. Increased myocardial stiffness caused by diffuse interstitial fibrosis is one way that chamber compliance becomes compromised. Left ventricular filling subsequently increases, which is the definition of diastolic dysfunction. One of the features of radiation-induced myocardial injury is diffuse interstitial fibrosis that can be detected as early as 50 days after exposure to irradiation and that increases in severity up to 82 days [35]. The considerable myocardial contractility reserve can maintain the ejection fraction within normal range until late stage left ventricular dysfunction. Consequently, in early stage of myocardium injury, diastolic left ventricular disorder rather than systolic dysfunction is more likely to be manifested. Our finding that LVDF may be more sensitive to subclinical cardiac damage than LVEF is consistent with the above cardiopathophysiology.
The dosimetric data of the heart and LV from our study indicated that there is a direct relationship between dose-volume of cardiac structure irradiated and early cardiac dysfunction in patients treated with left-sided RT concurrently with trastuzumab. The relationship between dose-volume of heart irradiated and systolic dysfunction found in this study was consistent with our previous report [15]. It has also been reported that the incidence of myocardial perfusion defects was related to dose and volume of LV irradiated in patients with left-sided breast cancer [3, 26]. Nevertheless, dose-response of LVDD has not been well documented. In this study, we identified for the first time a direct relationship between the risk of early LVDD and dose-volume of heart irradiation. Almost every agent used in breast cancer therapy carries a potential risk of cardiac toxicity, but the extent of these risks remains uncertain. Because the number of patients with and without LVDD was well balanced with respect to the proportion of patients receiving anthracycline-based chemotherapy and the cumulative dose of anthracycline, the LVDD observed in our study should be attributed mainly to the relatively high irradiated dose of the heart. At the same time, although a higher proportion of patients with right-sided tumor received anthracycline-based chemotherapy, the frequency of LVDD was still slightly higher in left-sided patients after concurrent treatment. As breast cancer RT techniques have been improved so as to reduce the volume of cardiac exposure, there has been a steady decline in the relative risk for RT-associated cardiotoxicity [4]. Nevertheless, data from our study indicate that the heart dose-volume remains an important cardiac risk factor for patients undergoing concurrent administration of trastuzumab and RT.
Our additional finding in the same population is that the risk of early LVDD and the extent of LVEF decrease were significantly elevated when sIMRT was used instead of FiF-IMRT. Compared with FiF-IMRT, the introduction of sIMRT in breast RT substantially altered the distribution of dose to the heart, mainly in the pattern of decreased high dose area at the cost of elevated low dose-volume [36, 37]. Consistently, sIMRT in our study significantly improved volume of the heart receiving more than 40 Gy and the LV receiving more than 35 Gy, whereas the mean dose and low dose-volumes of both the heart and LV for sIMRT were significantly higher than for FiF-IMRT. Although the impact of such an alteration has not been clearly established, our study indicates that an increase in low dose-volume might be detrimental.
Apart from the treatment-related factors, postmenopausal status was found to be an independent risk factor of LVDD. In total, the proportion of LVDD in pre- and postmenopausal patients was 20.7% versus 42.4%, with hazard ratio of 4.96 (95% confidence interval, 1.72–14.29). In a review of multicenter investigations, Tarantini et al. [38] found that patients aged 61 and older had an increased trastuzumab-related cardiovascular risk. In patients receiving concurrent trastuzumab and RT, postmenopausal status was also reported to be associated with increased acute cardiotoxicity of concurrent trastuzumab and RT [33]. Natural menopause has an unfavorable physiological impact on lipid metabolism, which is associated with the increased risk of coronary disease. The potential additive effect of anticancer treatment to the impaired coronary system may explain that postmenopausal patients are at higher risk of cardiac events. Therefore, we suggest that a more comprehensive list of cardiac functional parameters and personal history be incorporated into the clinical histories of breast cancer patients so that a personalized assessment of baseline risk can be realized.
Only 115 of the 143 patients enrolled in this study had normal baseline LVDF; thus, we had to limit the analysis to these patients. Until more recently, there has been a lack of quantitative evaluation for diastolic function. Nevertheless, Doppler echocardiography still plays a central role in the assessment of LVDF. Its major pitfall, however, is that its sensitivity and specificity in detecting diastolic abnormalities can be affected by several factors including heart rate, age, preload, afterload, and the skill of the echocardiographic operator [39]. The indicators of LVDD in our study were chosen based on clinical recommendation [24] and a report from Bella et al. [40], which showed that an E/A ratio of <0.6 or >1.5 was associated with significant increase of all-cause and cardiac mortality. Serum markers, such as N-terminal pro-B type natriuretic peptide and serum cardiac troponin-T, and myocardial strain measured by cardiac magnetic resonance imaging or tissue Doppler may also provide alternative options to detect the presence of LVDD in a more quantified manner and will be integrated in our future study [41–43].
The question of long-term clinical significance of early LVDD is not addressed in this study. Diastolic dysfunction has been reported to be associated with increased cardiac morbidity and mortality, as well as serve as a prognostic factor for cardiac toxicity induced by irradiation or trastuzumab [12, 25, 29]. Although additional studies and longer follow-up are needed to verify whether and to what extent these early dysfunction will translate into clinically meaningful defect, it is possible that cardiac injury under modern multidisciplinary treatment of breast cancer is higher than we have realized. Comprehensive evaluation of the cardiac function, not only at baseline but also at the beginning of each different treatment strategy, should be proposed to each patient. For radiation therapy, every effort should be made to minimize irradiation of the heart facing current finding.
Conclusion
A higher prevalence of early LVDD was identified in breast cancer patients treated with concurrent trastuzumab and RT or left-sided RT alone, which suggests that LVDD may serve as a more sensitive tool for early detection of cardiac damage and should be incorporated as a routine parameter in the functional monitoring of cardiotoxicity. A direct relationship between dose-volume of heart irradiated and early cardiac dysfunction was found in breast cancer patients who underwent left-sided RT with concurrent trastuzumab.
Acknowledgment
This study was supported in part by National Natural Science Foundation of China Grant 81172504.
Footnotes
For Further Reading: Sandra M. Swain, Michael S. Ewer, Javier Cortés et al. Cardiac Tolerability of Pertuzumab Plus Trastuzumab Plus Docetaxel in Patients With HER2-Positive Metastatic Breast Cancer in CLEOPATRA: A Randomized, Double-Blind, Placebo-Controlled Phase III Study. The Oncologist 2013;18:257–264.
Implications for Practice: CLEOPATRA was the first phase III trial in which the combination of pertuzumab with trastuzumab and docetaxel was studied in patients with HER2-positive metastatic breast cancer in the first line. As therapy with trastuzumab, especially in combination with anthracyclines, has been associated with cardiac dysfunction, it was important to investigate the cardiac tolerability of the study combination of two HER2-targeted antibodies, trastuzumab and pertuzumab, with docetaxel. Our analyses showed that the combination of pertuzumab, trastuzumab, and docetaxel was not associated with an increase in cardiac dysfunction, especially LVSD, compared with placebo, trastuzumab and docetaxel. Cardiac adverse events were largely reversible and clinically manageable. Despite our encouraging findings, we recommend the regular cardiac monitoring of patients while long-term safety data with pertuzumab-trastuzumab-based treatment are still being accrued in clinical practice.
Author Contributions
Conception/Design: Lu Cao, Gang Cai, Jia-Yi Chen
Provision of study material or patients: Lu Cao, Gang Cai, Cai Chang, Ai-Yu Miao, Zhao-Zhi Yang, Jin-Li Ma, Jia-Yi Chen
Collection and/or assembly of data: Lu Cao, Cai Chang, Ai-Yu Miao, Qian Zhang
Data analysis and interpretation: Lu Cao, Gang Cai, Cai Chang, Xiao-Li Yu, Zhao-Zhi Yang, Jiong Wu, Xiao-Mao Guo, Jia-Yi Chen
Manuscript writing: Lu Cao, Xiao-Li Yu, Jia-Yi Chen
Final approval of manuscript: Jia-Yi Chen
Disclosures
The authors indicated no financial relationships.
References
- 1.Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;366:2087–2106. doi: 10.1016/S0140-6736(05)67887-7. [DOI] [PubMed] [Google Scholar]
- 2.Darby SC, McGale P, Taylor CW, et al. Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: Prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol. 2005;6:557–565. doi: 10.1016/S1470-2045(05)70251-5. [DOI] [PubMed] [Google Scholar]
- 3.Marks LB, Yu X, Prosnitz RG, et al. The incidence and functional consequences of RT-associated cardiac perfusion defects. Int J Radiat Oncol Biol Phys. 2005;63:214–223. doi: 10.1016/j.ijrobp.2005.01.029. [DOI] [PubMed] [Google Scholar]
- 4.Giordano SH, Kuo YF, Freeman JL, et al. Risk of cardiac death after adjuvant radiotherapy for breast cancer. J Natl Cancer Inst. 2005;97:419–424. doi: 10.1093/jnci/dji067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Patt DA, Goodwin JS, Kuo YF, et al. Cardiac morbidity of adjuvant radiotherapy for breast cancer. J Clin Oncol. 2005;23:7475–7482. doi: 10.1200/JCO.2005.13.755. [DOI] [PubMed] [Google Scholar]
- 6.Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659–1672. doi: 10.1056/NEJMoa052306. [DOI] [PubMed] [Google Scholar]
- 7.Yin W, Jiang Y, Shen Z, et al. Trastuzumab in the adjuvant treatment of HER2-positive early breast cancer patients: A meta-analysis of published randomized controlled trials. PLoS One. 2011;6:e21030. doi: 10.1371/journal.pone.0021030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pietras RJ, Poen JC, Gallardo D, et al. Monoclonal antibody to HER-2/neureceptor modulates repair of radiation-induced DNA damage and enhances radiosensitivity of human breast cancer cells overexpressing this oncogene. Cancer Res. 1999;59:1347–1355. [PubMed] [Google Scholar]
- 9.Liang K, Lu Y, Jin W, et al. Sensitization of breast cancer cells to radiation by trastuzumab. Mol Cancer Ther. 2003;2:1113–1120. [PubMed] [Google Scholar]
- 10.Sherief LM, Kamal AG, Khalek EA, et al. Biomarkers and early detection of late onset anthracycline-induced cardiotoxicity in children. Hematology. 2012;17:151–156. doi: 10.1179/102453312X13376952196412. [DOI] [PubMed] [Google Scholar]
- 11.Mukherjee M, Dusaj R, Stewart K, et al. Predictors of abnormal longitudinal strain using left ventricular speckle tracking in ambulatory hypertensive patients with preserved ejection fraction. J Am Coll Cardiol. 2013 [Google Scholar]
- 12.Redfield MM, Jacobsen SJ, Burnett JC, Jr., et al. Burden of systolic and diastolic ventricular dysfunction in the community: Appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202. doi: 10.1001/jama.289.2.194. [DOI] [PubMed] [Google Scholar]
- 13.Zaya M, Mehta P, Mohammadi AH, et al. Microvascular coronary dysfunction, left ventricular volumes and mass: Results from the women's ischemia syndrome evaluation-coronary vascular dysfunction study. J Am Coll Cardiol. 2013;61:E1442. [Google Scholar]
- 14.Gagliardi G, Constine LS, Moiseenko V, et al. Radiation dose-volume effects in the heart. Int J Radiat Oncol Biol Phys. 2010;76(suppl):S77–S85. doi: 10.1016/j.ijrobp.2009.04.093. [DOI] [PubMed] [Google Scholar]
- 15.Cao L, Hu WG, Kirova YM, et al. Potential impact of cardiac dose-volume on acute cardiac toxicity following concurrent trastuzumab and radiotherapy. Cancer Radiother. 2014;18:119–124. doi: 10.1016/j.canrad.2014.01.001. [DOI] [PubMed] [Google Scholar]
- 16.Edge SB, Compton CC. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol . 2010;17:1471–1474. doi: 10.1245/s10434-010-0985-4. [DOI] [PubMed] [Google Scholar]
- 17.Kestin LL, Sharpe MB, Frazier RC, et al. Intensity modulation to improve dose uniformity with tangential breast radiotherapy: Initial clinical experience. Int J Radiat Oncol Biol Phys. 2000;48:1559–1568. doi: 10.1016/s0360-3016(00)01396-1. [DOI] [PubMed] [Google Scholar]
- 18.Hui G, Jianrong D, Yexiong L, et al. A simplified intensity modulated radiation therapy technique for difficult clinical cancer condition. Chinese Journal of Radiation Oncology. 2006;15:411–415. [Google Scholar]
- 19.Radiation Therapy Oncology Group. Breast cancer contouring atlas. Available at http://www.rtog.org/CoreLab/ContouringAtlases/BreastCancerAtlas.aspx.
- 20.Feng M, Moran JM, Koelling T, et al. Development and validation of a heart atlas to study cardiac exposure to radiation following treatment for breast cancer. Int J Radiat Oncol Biol Phys. 2011;79:10–18. doi: 10.1016/j.ijrobp.2009.10.058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Taylor CW, Nisbet A, McGale P, et al. Cardiac exposures in breast cancer radiotherapy: 1950s–1990s. Int J Radiat Oncol Biol Phys. 2007;69:1484–1495. doi: 10.1016/j.ijrobp.2007.05.034. [DOI] [PubMed] [Google Scholar]
- 22.Erven K, Florian A, Slagmolen P, et al. Subclinical cardiotoxicity detected by strain rate imaging up to 14 months after breast radiation therapy. Int J Radiat Oncol Biol Phys. 2013;85:1172–1178. doi: 10.1016/j.ijrobp.2012.09.022. [DOI] [PubMed] [Google Scholar]
- 23.Simonson JS, Schiller NB. Descent of the base of the left ventricle: An echocardiographic index of left ventricular function. J Am Soc Echocardiogr. 1989;2:25–35. doi: 10.1016/s0894-7317(89)80026-4. [DOI] [PubMed] [Google Scholar]
- 24.Paulus WJ, Tschöpe C, Sanderson JE, et al. How to diagnose diastolic heart failure: A consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28:2539–2550. doi: 10.1093/eurheartj/ehm037. [DOI] [PubMed] [Google Scholar]
- 25.Heidenreich PA, Hancock SL, Vagelos RH, et al. Diastolic dysfunction after mediastinal irradiation. Am Heart J. 2005;150:977–982. doi: 10.1016/j.ahj.2004.12.026. [DOI] [PubMed] [Google Scholar]
- 26.Hardenbergh PH, Munley MT, Bentel GC, et al. Cardiac perfusion changes in patients treated for breast cancer with radiation therapy and doxorubicin: Preliminary results. Int J Radiat Oncol Biol Phys. 2001;49:1023–1028. doi: 10.1016/s0360-3016(00)01531-5. [DOI] [PubMed] [Google Scholar]
- 27.Adams MJ, Hardenbergh PH, Constine LS, et al. Radiation-associated cardiovascular disease. Crit Rev Oncol Hematol. 2003;45:55–75. doi: 10.1016/s1040-8428(01)00227-x. [DOI] [PubMed] [Google Scholar]
- 28.Yavas G, Yildiz F, Guler S, et al. Concomitant trastuzumab with thoracic radiotherapy: A morphological and functional study. Ann Oncol. 2011;22:1120–1126. doi: 10.1093/annonc/mdq590. [DOI] [PubMed] [Google Scholar]
- 29.Cochet A, Quilichini G, Dygai-Cochet I, et al. Baseline diastolic dysfunction as a predictive factor of trastuzumab-mediated cardiotoxicity after adjuvant anthracycline therapy in breast cancer. Breast Cancer Res Treat. 2011;130:845–854. doi: 10.1007/s10549-011-1714-9. [DOI] [PubMed] [Google Scholar]
- 30.Crone SA, Zhao YY, Fan L, et al. ErbB2 is essential in the prevention of dilated cardiomyopathy. Nat Med. 2002;8:459–465. doi: 10.1038/nm0502-459. [DOI] [PubMed] [Google Scholar]
- 31.Halyard MY, Pisansky TM, Dueck AC, et al. Radiotherapy and adjuvant trastuzumab in operable breast cancer: Tolerability and adverse event data from the NCCTG Phase III Trial N9831. J Clin Oncol. 2009;27:2638–2644. doi: 10.1200/JCO.2008.17.9549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Shaffer R, Tyldesley S, Rolles M, et al. Acute cardiotoxicity with concurrent trastuzumab and radiotherapy including internal mammary chain nodes: A retrospective single-institution study. Radiother Oncol. 2009;90:122–126. doi: 10.1016/j.radonc.2008.09.003. [DOI] [PubMed] [Google Scholar]
- 33.Belkacémi Y, Gligorov J, Ozsahin M, et al. Concurrent trastuzumab with adjuvant radiotherapy in HER2-positive breast cancer patients: Acute toxicity analyses from the French multicentric study. Ann Oncol. 2008;19:1110–1116. doi: 10.1093/annonc/mdn029. [DOI] [PubMed] [Google Scholar]
- 34.Nishimura RA, Tajik AJ. Evaluation of diastolic filling of left ventricle in health and disease: Doppler echocardiography is the clinician’s Rosetta Stone. J Am Coll Cardiol. 1997;30:8–18. doi: 10.1016/s0735-1097(97)00144-7. [DOI] [PubMed] [Google Scholar]
- 35.Stewart JR, Fajardo LF. Radiation-induced heart disease. Clinical and experimental aspects. Radiol Clin North Am. 1971;9:511–531. [PubMed] [Google Scholar]
- 36.Beckham WA, Popescu CC, Patenaude VV, et al. Is multibeam IMRT better than standard treatment for patients with left-sided breast cancer? Int J Radiat Oncol Biol Phys. 2007;69:918–924. doi: 10.1016/j.ijrobp.2007.06.060. [DOI] [PubMed] [Google Scholar]
- 37.Coon AB, Dickler A, Kirk MC, et al. Tomotherapy and multifield intensity-modulated radiotherapy planning reduce cardiac doses in left-sided breast cancer patients with unfavorable cardiac anatomy. Int J Radiat Oncol Biol Phys. 2010;78:104–110. doi: 10.1016/j.ijrobp.2009.07.1705. [DOI] [PubMed] [Google Scholar]
- 38.Tarantini L, Gori S, Faggiano P, et al. Adjuvant trastuzumab cardiotoxicity in patients over 60 years of age with early breast cancer: A multicenter cohort analysis. Ann Oncol. 2012;23:3058–3063. doi: 10.1093/annonc/mds127. [DOI] [PubMed] [Google Scholar]
- 39.Grodecki PV, Klein AL. Pitfalls in the echo-Doppler assessment of diastolic dysfunction. Echocardiography. 1993;10:213–234. doi: 10.1111/j.1540-8175.1993.tb00032.x. [DOI] [PubMed] [Google Scholar]
- 40.Bella JN, Palmieri V, Roman MJ, et al. Mitral ratio of peak early to late diastolic filling velocity as a predictor of mortality in middle-aged and elderly adults: The Strong Heart Study. Circulation. 2002;105:1928–1933. doi: 10.1161/01.cir.0000015076.37047.d9. [DOI] [PubMed] [Google Scholar]
- 41.Tschöpe C, Kasner M, Westermann D, et al. The role of NT-proBNP in the diagnostics of isolated diastolic dysfunction: Correlation with echocardiographic and invasive measurements. Eur Heart J. 2005;26:2277–2284. doi: 10.1093/eurheartj/ehi406. [DOI] [PubMed] [Google Scholar]
- 42.Kilickap S, Barista I, Akgul E, et al. cTnT can be a useful marker for early detection of anthracycline cardiotoxicity. Ann Oncol. 2005;16:798–804. doi: 10.1093/annonc/mdi152. [DOI] [PubMed] [Google Scholar]
- 43.Nagueh SF, Appleton CP, Gillebert TC, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr. 2009;10:165–193. doi: 10.1093/ejechocard/jep007. [DOI] [PubMed] [Google Scholar]