

Abstract
Background
Recently, a Korean fracture-risk assessment tool (FRAX) model has become available, but large prospective cohort studies, which are needed to validate the model, are still lacking, and there has been little effort to evaluate its usefulness. This study evaluated the clinical usefulness of the FRAX model, a FRAX developed by the World Health Organization, in Korea.
Methods
In 405 postmenopausal women and 139 men with a proximal femoral fracture, 10-year predicted fracture probabilities calculated by the Korean FRAX model (a country-specific model) were compared with the probabilities calculated with a FRAX model for Japan, which has a similar ethnic background (surrogate model).
Results
The 10-year probabilities of major osteoporotic and hip fractures calculated by the Korean model were significantly lower than those calculated by the Japanese model in women and men. The fracture probabilities calculated by each model increased significantly with age in both sexes. In patients aged 70 or older, however, there was a significant difference between the two models. In addition, the Korean model led to lower probabilities for major osteoporotic fracture and hip fracture in women when BMD was excluded from the model than when it was included.
Conclusions
The 10-year fracture probabilities calculated with FRAX models might differ between country-specific and surrogate models, and caution is needed when applying a surrogate model to a new population. A large prospective study is warranted to validate the country-specific Korean model in the general population.
Keywords: Hip fractures, Japan, Osteoporotic fractures, Republic of Korea, Risk assessment
INTRODUCTION
Fractures related to osteoporosis are a major health issue worldwide and a significant economic and social burden. Hip fractures in particular result in higher costs and greater morbidity and mortality than do other osteoporotic fractures.[1] Thus, it is important to recognize and manage individuals who are at high risk of fractures, and many efforts have been made to predict fracture risk. Bone mineral density (BMD) is known to account for about 70% of bone strength.[2] However, the prevalence of osteoporosis, as assessed with peripheral BMD, is quite low (18%) in women sustaining fracture,[3] and hip fractures occur in 36% of women without osteoporosis, as determined by femoral neck BMD.[4]
To improve the prediction of major osteoporotic fractures (MOFs), such as those of the spine, forearm, shoulder, and hip, the World Health Organization (WHO) has developed a fracture-risk assessment tool (FRAX).[5] The model uses easily obtainable clinical risk factors related to fractures to predict fracture probability. However, the FRAX model for a given country should be customized based on the epidemiology of the fracture and life expectancy of the population in relation to geography and ethnicity,[6] so a population-specific FRAX model is necessary for each country or ethnicity.[7]
When a country-specific FRAX model is not developed, a surrogate model based on data from a similar ethnic background can be considered. We previously reported that the Japanese FRAX model might be appropriate as a surrogate model of fracture risk for Korean women.[8] In women with hip fracture, the Japanese model leads to higher fracture probabilities than the Chinese or Turkish model, which increase in an age-dependent manner, and furthermore, the hip fracture risk for women is considered to be intermediate in both Korea and Japan.[8] Recently, a Korean FRAX model has become available (http://www.shef.ac.uk/FRAX), but large prospective cohort studies, which are needed to validate the model, are still lacking, and there has been little effort to evaluate its usefulness.
The purpose of this study was to evaluate the clinical usefulness of the Korean FRAX model by comparing fracture probabilities calculated by the country-specific and surrogate models among Korean patients with hip fracture.
METHODS
This cross-sectional study included men and postmenopausal women who were admitted to Samsung Medical Center with a proximal femoral fracture between March 2005 and October 2010. Women were considered postmenopausal when the duration of amenorrhea was ≥12 months or the serum level of follicle-stimulating hormone was >40 IU/L. The clinical usefulness of the Korean FRAX model was indirectly assessed by comparing it with the Japanese model (web version 3.7). Only participants with no missing data for the calculation of 10-year predicted fracture risk with the FRAX model were included. The study protocol was approved by the Institutional Review Board of Samsung Medical Center (No. 2012-12-105).
The following clinical risk factors required for the FRAX model were collected from the participants' medical records: age, body mass index (BMI), history of a prior fragility fracture or parental hip fracture, smoking history, history of long-term oral glucocorticoid use, rheumatoid arthritis, daily alcohol consumption of three or more units daily, and other causes of secondary osteoporosis.[9] The BMD was measured at the femoral neck by dual energy X-ray absorptiometry (DXA; Delphi W, Hologic Inc., Bedford, MA, USA) and presented as g/cm2. The in vivo coefficient of variation using a densitometer was 1.4% for the hip. Only BMD measured within six months on the opposite side of the fracture was used for analyses.
Data are presented as mean±standard deviation (SD) or number (percentage). Chi-square tests or Fisher exact tests were used to compare frequencies. Student's t-test or Mann-Whitney tests were used to analyze differences between models. Differences in relation to age were assessed with analysis of variance or the Kruskal-Wallis test. P-values< 0.05 were considered statistically significant. All statistical calculations were performed with PASW Statistics 19 (SPSS Inc., Chicago, IL, USA).
RESULTS
After excluding thirty-two patients, a total of 544 participants were enrolled in this study. There were 405 women and 139 men. Table 1 summarizes the variables used in the FRAX model. The proportion of participants with a history of fragility fracture or long-term oral glucocorticoid use was significantly higher in women than men, while the proportion of participants who were current smokers, consumed ≥3 units of alcohol daily, or had other causes of secondary osteoporosis was higher in men than in women. Data on BMD at the femoral neck were available in 202 women (49.9%) and 40 men (28.8%). Femoral BMD was significantly lower and the prevalence of osteoporosis at the femur neck (76.2% vs. 42.5%) was significantly higher in women than men.
Table 1. Study subject variables included in the fracture-risk assessment tool model.
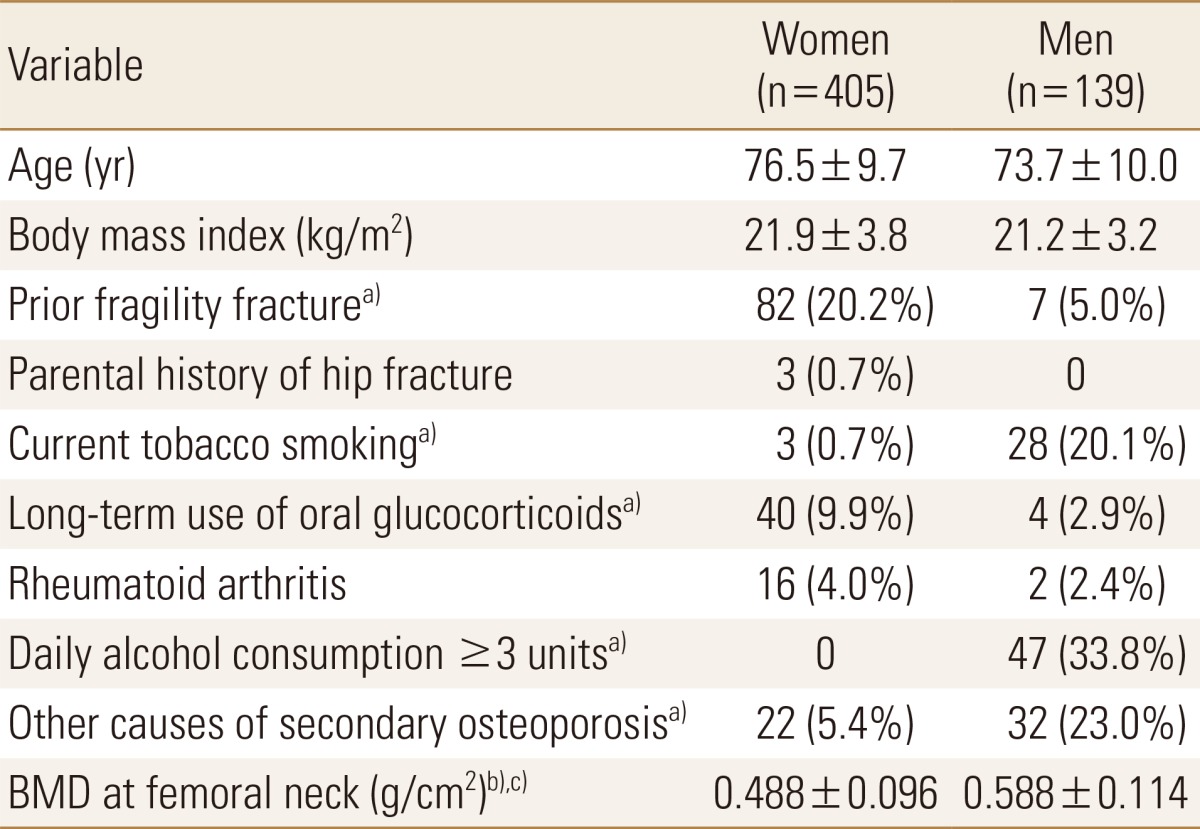
Data are presented as the mean±standard deviation (SD) or number (percentage).
a)P<0.05 between the sexes by the Fisher's exact or chi-square test, as indicated.
b)P<0.05 between sexes by t test.
c)n=202 for women, n=40 for men.
BMD, bone mineral density.
The 10-year probabilities of MOF and hip fracture without BMD are shown in Table 2. For both MOF and hip fracture, the probabilities calculated by the Korean model were significantly lower than those calculated by the Japanese model in both sexes.
Table 2. Ten-year fracture probabilities without bone mineral density calculated with two different fracture-risk assessment tool models.
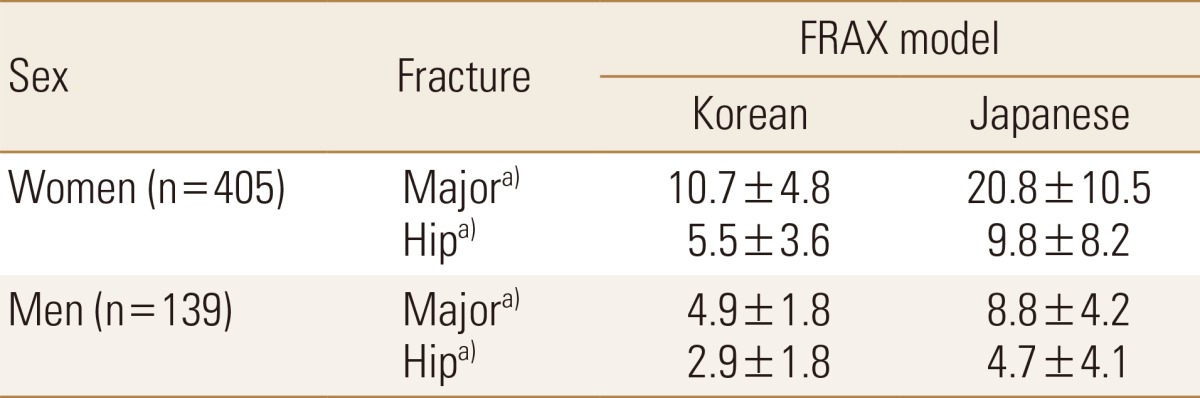
Data are presented as the mean±standard deviation (SD) (%).
a)P<0.05, between the two models.
FRAX, fracture-risk assessment tool.
Clinical usefulness of the Korean FRAX model was also examined in relation to age. Table 3 summarizes clinical risk factors in relation to age. BMI and BMD gradually decreased as age increased in women. Figure 1 illustrates fracture probabilities for different age groups. In women, the fracture probability increased significantly with age in both models after adjusting for BMI and BMD. However, there were significant differences between the two models: In contrast to the Japanese model, the probability of MOF (Fig. 1A) and hip fracture (Fig. 1B) did not continue to increase in the Korean model, but rather, they decreased after the age of 70 years, leading to substantial differences in fracture probabilities between the two models for elderly women. In men, similar patterns were observed between the two models for MOF (Fig. 1C) and hip fracture (Fig. 1D).
Table 3. Variables included in the fracture risk assessment tool model in relation to age and sex.
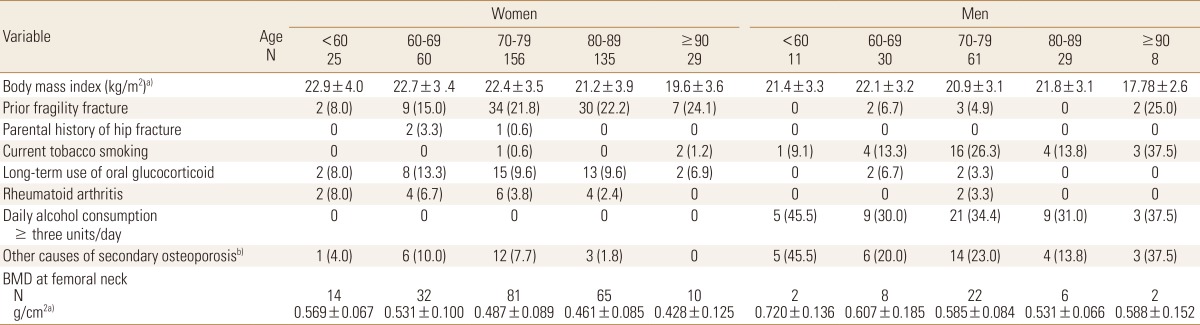
Data are presented as mean±standard deviation (SD) or number (percentage).
Others causes of secondary osteoporosis include type1 diabetes, osteogenesis imperfecta, hyperthyroidism, hypogonadism or premature menopause, chronic malnutrition or malabsorption, chronic disease, and etc.
a)P<0.05 in women by analysis of variance or the Kruskal-Wallis test, as indicated.
b)P<0.05 in women by Fisher's exact test.
BMD, bone mineral density.
Fig. 1. Mean 10-year fracture probabilities using the Korean and Japanese fracture-risk assessment tool (FRAX) models in relation to age in women and men. (A) Major osteoporotic fracture (MOF) and (B) hip fracture in women, (C) MOF and (D) hip fracture in men. In both models, the fracture probabilities increased significantly in relation to age in both sexes (P<0.001, ANOVA). KOR, Korean; JPN, Japanese; *P<0.05 by t-test or Mann-Whitney test, as indicated.

In addition, both fracture probabilities calculated with the Korean model in women were significantly higher when BMD values were included than when they were excluded (Fig. 2A). Probabilities for MOF, but not hip fracture, also rose after inclusion of BMD in the Japanese model (Fig. 2B).
Fig. 2. Mean 10-year fracture probabilities using (A) the Korean model and (B) the Japanese model with and without the inclusion of BMD values in women. The probabilities without BMD values were significantly lower for both major osteoporotic fracture and hip fracture. BMD, bone mineral density; *P<0.05, t-test.

DISCUSSION
This study evaluated the usefulness of the Korean FRAX model in a high risk group of patients with an established hip fracture. Our results revealed that the probabilities of both MOF and hip fracture were about 50% lower with the Korean model than the Japanese model, a difference that was statistically significant.
Our findings are in line with a previous study showing that probability of vertebral fracture by the Korean FRAX model might be underestimated compared to that by the Japanese model.[10] However, that study compared fracture and non-fracture group and used BMD at the lumbar spine instead of femoral neck BMD.
Since the age-standardized rates per 100,000 of hip fracture were similar in the two countries (Korean women, 268; Japanese women, 266; Korean men, 176; Japanese men, 165),[11,12] different probabilities might result from a difference in mortality between the two countries. For the Japanese model, the mortality estimates by the WHO for 1999 were used.[13] According to official national statistics, age-adjusted mortality rates (per 100,000) were higher in Korea (2004) than Japan (2000) for women (375 vs. 320) and men (721 vs. 630).
According to recent reports, the residual lifetime risk (RLR) of a hip fracture at age 50 was 12.3% in Korean women and 20% in Japanese women.[14,15] Similar to 10-year fracture probabilities, the RLR of fractures is dependent on mortality rates. In the current study, 10-year fracture probabilities were two times higher with the Japanese model than the Korean model, which is consistent with the difference in RLR between the two countries. These findings suggest that a country-specific model might yield fracture probabilities with greater clinical relevance than a surrogate model.
The most important risk factor for fracture independent of BMD is age.[16] The probabilities of MOF and hip fracture increased with age in both sexes with both models. Of note, fracture probabilities in study participants aged 70 years or older were remarkably lower with the Korean FRAX model than the Japanese FRAX model. Age-specific mortality rates for women aged 70 through 79 years were 3,520 in Japan (2000) and 5,711 in Korea (2004), and for women aged 80 through 89 years were 12,540 in Japan (2000) and 19,928 in Korea (2004).[17] This mortality difference might account, in part, for the difference in fracture probabilities for elderly patients. Furthermore, fracture probabilities using the country-specific model are consistent with a recent Korean study reporting that the RLR of overall osteoporosis-related fractures decreases after the age of 70 years.[13]
FRAX was developed mainly due to the low sensitivity of BMD in predicting fracture risk and the low accessibility of BMD worldwide.[18] Hence, fracture probabilities may not be affected by inclusion of BMD in an ideal FRAX model. In the current study, however, fracture probabilities were higher when BMD results were included. Recent analysis of Korean National Health and Nutrition Examination Survey also reported that the Korean FRAX model without BMD yielded lower fracture probabilities compared to those with BMD.[19] Although the effects of inclusion of BMD on the calculation of FRAX are still not clear,[20,21,22] this difference might be due to the high prevalence of osteoporosis of the hip in the current study (76.2%). The prevalence of osteoporosis in the spine or hip is 35.5% in Korean women aged 50 years older.[23]
Although FRAX is a useful tool, it also has a number of limitations.[7,16,24,25] For example, several variables, such as a history of falling, physical activity, vitamin D deficiency, or bone turnover marker, are excluded from the model. The model also does not account for dose-response relationships in terms of fracture, glucocorticoid use, alcohol, or smoking. It can only be used in an untreated population. In addition, BMD is limited to the femoral neck. Even though FRAX can account for racial or ethnic differences, validation of the computed country-specific model might still be needed.[26,27] Japanese model has been validated using a population-based cohort study.[20]
The current study had some limitations. First, participants were recruited from a tertiary care center, so the distribution of clinical risk factors might not represent that of the general Korean population. Moreover, only participants with an established hip fracture were included, so caution is needed before extrapolating our results to populations with a low risk of fracture. Second, the participants were elderly, and the prevalence of osteoporosis was high. Further studies that include younger women with osteopenia are necessary. In addition, the proportion of participants for whom we had BMD measurements was low. Finally, this study could not validate the Korean FRAX model, because study design was not longitudinal.
In summary, the 10-year fracture probabilities differed significantly between Korean and Japanese FRAX models when applied to patients with hip fracture. The differences between models might be largely explained by differences in mortality between countries. Caution is needed when clinical decisions are based on the results from a surrogate model. Moreover, a large prospective study, if available, is warranted for the validation of country-specific models in the general population.
Footnotes
No potential conflict of interest relevant to this article was reported.
This work was supported in part by the Samsung Medical Center Research Fund, PH01991081, PH01095291, and PH01095801-PHO1133361 and the IN-SUNG Foundation for Medical Research, C-A5-811-1.
References
- 1.Braithwaite RS, Col NF, Wong JB. Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc. 2003;51:364–370. doi: 10.1046/j.1532-5415.2003.51110.x. [DOI] [PubMed] [Google Scholar]
- 2.Miller PD, Zapalowski C, Kulak CA, et al. Bone densitometry: the best way to detect osteoporosis and to monitor therapy. J Clin Endocrinol Metab. 1999;84:1867–1871. doi: 10.1210/jcem.84.6.5710. [DOI] [PubMed] [Google Scholar]
- 3.Siris ES, Chen YT, Abbott TA, et al. Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med. 2004;164:1108–1112. doi: 10.1001/archinte.164.10.1108. [DOI] [PubMed] [Google Scholar]
- 4.Schuit SC, van der Klift M, Weel AE, et al. Fracture incidence and association with bone mineral density in elderly men and women: the Rotterdam Study. Bone. 2004;34:195–202. doi: 10.1016/j.bone.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 5.Kanis JA, Borgström F, De Laet C, et al. Assessment of fracture risk. Osteoporos Int. 2005;16:581–589. doi: 10.1007/s00198-004-1780-5. [DOI] [PubMed] [Google Scholar]
- 6.Kanis JA, Johnell O, De Laet C, et al. International variations in hip fracture probabilities: implications for risk assessment. J Bone Miner Res. 2002;17:1237–1244. doi: 10.1359/jbmr.2002.17.7.1237. [DOI] [PubMed] [Google Scholar]
- 7.Kanis JA, Oden A, Johansson H, et al. FRAX and its applications to clinical practice. Bone. 2009;44:734–743. doi: 10.1016/j.bone.2009.01.373. [DOI] [PubMed] [Google Scholar]
- 8.Kanis JA, Odén A, McCloskey EV, et al. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int. 2012;23:2239–2256. doi: 10.1007/s00198-012-1964-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kanis JA, Black D, Cooper C, et al. A new approach to the development of assessment guidelines for osteoporosis. Osteoporos Int. 2002;13:527–536. doi: 10.1007/s001980200069. [DOI] [PubMed] [Google Scholar]
- 10.So GY, Park KH, Yoon DH, et al. Feasibility of FRAX for Prediction of Osteoporotic Vertebral Fractures in Korea. Asian Spine J. 2012;6:22–28. doi: 10.4184/asj.2012.6.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lim S, Koo BK, Lee EJ, et al. Incidence of hip fractures in Korea. J Bone Miner Metab. 2008;26:400–405. doi: 10.1007/s00774-007-0835-z. [DOI] [PubMed] [Google Scholar]
- 12.Orimo H, Sakata K. The 4th nationwide survey for hip fracture in Japan. Jpn Med J. 2006;4180:25–30. [Google Scholar]
- 13.Fujiwara S, Nakamura T, Orimo H, et al. Development and application of a Japanese model of the WHO fracture risk assessment tool (FRAX) Osteoporos Int. 2008;19:429–435. doi: 10.1007/s00198-007-0544-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Park C, Ha YC, Jang S, et al. The incidence and residual lifetime risk of osteoporosis-related fractures in Korea. J Bone Miner Metab. 2011;29:744–751. doi: 10.1007/s00774-011-0279-3. [DOI] [PubMed] [Google Scholar]
- 15.Hagino H, Furukawa K, Fujiwara S, et al. Recent trends in the incidence and lifetime risk of hip fracture in Tottori, Japan. Osteoporos Int. 2009;20:543–548. doi: 10.1007/s00198-008-0685-0. [DOI] [PubMed] [Google Scholar]
- 16.Kanis JA, Johnell O, Oden A, et al. FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int. 2008;19:385–397. doi: 10.1007/s00198-007-0543-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Statistics Korea. Vital statistics: Age-specific death rate. 2005. [cited by 2015 Jan 12]. Available from http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B80A17&conn_path=I2.
- 18.Kanis JA, Johnell O, Oden A, et al. Ten-year risk of osteoporotic fracture and the effect of risk factors on screening strategies. Bone. 2002;30:251–258. doi: 10.1016/s8756-3282(01)00653-6. [DOI] [PubMed] [Google Scholar]
- 19.Kim JW, Koh JM, Park JH, et al. Validation of FRAX without BMD: an age-related analysis of the Fifth Korean National Health and Nutrition Examination Survey (KNHANES V-1, 2010) Bone. 2015;75:27–31. doi: 10.1016/j.bone.2015.02.013. [DOI] [PubMed] [Google Scholar]
- 20.Tamaki J, Iki M, Kadowaki E, et al. Fracture risk prediction using FRAX(R): a 10-year follow-up survey of the Japanese Population-Based Osteoporosis (JPOS) Cohort Study. Osteoporos Int. 2011;22:3037–3045. doi: 10.1007/s00198-011-1537-x. [DOI] [PubMed] [Google Scholar]
- 21.Ensrud KE, Lui LY, Taylor BC, et al. A comparison of prediction models for fractures in older women: is more better? Arch Intern Med. 2009;169:2087–2094. doi: 10.1001/archinternmed.2009.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Leslie WD, Lix LM. Comparison between various fracture risk assessment tools. Osteoporos Int. 2014;25:1–21. doi: 10.1007/s00198-013-2409-3. [DOI] [PubMed] [Google Scholar]
- 23.Choi YJ, Oh HJ, Kim DJ, et al. The prevalence of osteoporosis in Korean adults aged 50 years or older and the higher diagnosis rates in women who were beneficiaries of a national screening program: the Korea National Health and Nutrition Examination Survey 2008-2009. J Bone Miner Res. 2012;27:1879–1886. doi: 10.1002/jbmr.1635. [DOI] [PubMed] [Google Scholar]
- 24.Silverman SL, Calderon AD. The utility and limitations of FRAX: A US perspective. Curr Osteoporos Rep. 2010;8:192–197. doi: 10.1007/s11914-010-0032-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Watts NB, Ettinger B, LeBoff MS. FRAX facts. J Bone Miner Res. 2009;24:975–979. doi: 10.1359/jbmr.090402. [DOI] [PubMed] [Google Scholar]
- 26.González-Macías J, Marin F, Vila J, et al. Probability of fractures predicted by FRAX(R) and observed incidence in the Spanish ECOSAP Study cohort. Bone. 2012;50:373–377. doi: 10.1016/j.bone.2011.11.006. [DOI] [PubMed] [Google Scholar]
- 27.Ettinger B, Ensrud KE, Blackwell T, et al. Performance of FRAX in a cohort of community-dwelling, ambulatory older men: the Osteoporotic Fractures in Men (MrOS) study. Osteoporos Int. 2013;24:1185–1193. doi: 10.1007/s00198-012-2215-3. [DOI] [PMC free article] [PubMed] [Google Scholar]