An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
aLoyola University Medical Center, Maywood, Illinois, USA
bBoston Children's Hospital, Boston, Massachusetts, USA
✉
Address correspondence to Paul C. Schreckenberger, pschrecken@lumc.edu, or Alexander J. McAdam, alexander.mcadam@childrens.harvard.edu.
Citation Schreckenberger PC, McAdam AJ. 2015. Point-Counterpoint: Large multiplex PCR panels should be first-line tests for detection of respiratory and intestinal pathogens. J Clin Microbiol 53:3110–3115. doi:10.1128/JCM.00382-15.
The first FDA-approved multiplex PCR panel for a large number of respiratory pathogens was introduced in 2008. Since then, other PCR panels for detection of several respiratory and gastrointestinal pathogens have been approved by the FDA and are commercially available, and more such panels are likely to become available. These assays detect 12 to 20 pathogens, and some include pathogens that typically cause different manifestations of infection, although they infect the same organ system. Some of these tests are labor-intensive, while others require little labor, and all of them are expensive, both for the laboratory and for the patient or insurer. They include a bundle of tests with limited or no options for selecting which tests will be performed. Laboratories and hospitals have adopted different strategies for offering these assays. Some have implemented strategies to limit the use of the tests, such as limiting the frequency with which patients can be tested, restricting testing to specific groups of patients (e.g., immunocompromised patients), or providing education to encourage the use of less expensive tests before using large multiplex panels. Others have offered these assays without limiting their use, either relying on the ordering provider to exercise good judgment or because such assays are thought to be appropriate for first-line diagnostic testing. In this Point-Counterpoint, Paul Schreckenberger of Loyola University Medical Center explains why his laboratory offers these assays without restriction. Alex McAdam of Boston's Children Hospital explains the concerns about the use of these assays as first-line tests and why some limitations on their use might be appropriate.
With very few exceptions, infectious diseases present as a constellation of symptoms that collectively indicate or characterize a disease. Patients present with diarrhea or difficulty breathing, or they may have a fever accompanied by hypotension. The infectious causes are broad and diverse, and the infectious agents might be bacterial, viral, or fungal. The symptoms are rarely agent specific, and the empirical response is to treat for everything. Cocktails of antibiotics are given even when the cause may be viral or fungal. Gram-positive coverage is added even when the cause is Gram-negative bacteria or vice versa. It is called empirical therapy, but it is actually “guess” therapy because the causative agents are not symptom specific and the laboratory results will not be available for 2 to 3 days. In the clinical microbiology laboratory, we have always offered syndromic tests: i.e., stool culture, sputum culture, blood culture, urine culture, fungal culture, and viral culture, etc. Physicians are not asked to name the exact bacterium, fungus, or virus that should be tested for. The specimen is collected and submitted to the lab with the expectation that all pertinent pathogens will be isolated and identified. The development of molecular testing with agent-specific primers requires physicians to name which agents they want the laboratory to test for, and if they ask for too many, they get pushback from the lab.
Introduction of respiratory panels.
Our initial foray into multiplex PCR testing came with the Prodesse ProFlu+ assay (Hologic), which detects influenza A and B viruses and respiratory syncytial virus. However, this was a batch assay that was run only once per day, so it did not satisfy our emergency department (ED) physicians, who wanted a rapid turnaround for patient management decisions. Next we implemented a rapid 1-h influenza A/B virus PCR assay (FLUPCR) that was hugely popular but limited in terms of etiologic agents detected. When the microarray respiratory panel (RESPAN) was implemented in our laboratory, our physicians could test for the 20 most common (17 viral and 3 bacterial) agents causing acute respiratory infection, with results available in about 1 h at a total cost that was less than the cost of a single send-out PCR test. The test result provided the opportunity to limit the time in the ED, omit antibiotics if the agent was viral, and treat patients on an outpatient basis if the etiologic agent was known to cause a self-limited type of infection, thus avoiding the cost of a hospital admission. After introducing the RESPAN, the most frequent question I received from physicians was “when are we going to have these types of panels for other syndromes, like sepsis, meningitis, pneumonia, and gastrointestinal symptoms?”
Do physicians practice good laboratory stewardship?
At Loyola University Medical Center, we continue to offer two testing options for acute respiratory illness, RESPAN and FLUPCR. We ask our physicians to choose which test they want, and we advise them not to order both tests. I send our physicians an annual email at the beginning of each influenza season detailing four things: (i) the names and order codes for the two tests offered, (ii) a statement that testing is performed on demand with a 1.5-h turnaround time, (iii) a list of agents detected in each assay, and (iv) the cost to the laboratory and the patient charge for each assay. I remind them that they should not order FLUPCR as a screening test and then order RESPAN when the FLUPCR is negative, because this would drive up the cost of testing and third-party payers might consider the RESPAN to be a duplicate test and therefore deny payment. During our last flu season, which lasted 4 months, from December 2013 through March 2014, a combined 1,761 viral respiratory tests were performed, with only 241 (13%) positive for influenza A/B (227 influenza A, 14 influenza B). That means that 87% of the patients will test negative if only the influenza A/B test is ordered. I ask our physicians to consider this fact when deciding whether to order FLUPCR or RESPAN. In the 12-month period from October 2013 to September 2014, 87% of the tests ordered were RESPAN and 13% were FLUPCR (Table 1). During the months of high flu activity, physicians ordered more FLUPCR, and during the months of low flu activity, they ordered mostly RESPAN, which is as it should be. Of great interest are the positivity rates for the two tests. When influenza A/B only testing is ordered in our laboratory, the positivity rate averages 28%, ranging from 0 to 42% depending on the prevalence of flu in the area (Table 1). With our syndromic panel, the positivity rate is 39% (range, 28 to 48%) (Table 1). Inpatients and ED patients account for the majority of RESPAN orders, with 49% of orders coming from inpatients and 35% coming from ED patients (Table 1). I believe that our physicians are committed to laboratory stewardship and are prudent in making good choices about the use of syndromic test panels.
TABLE 1.
Monthly volume and percent positivity results for FLUPCR and RESPAN
Cost of molecular multiplex respiratory virus panels.
When people talk about the cost of performing large multiplex PCR panels, what I refer to as “syndromic panels” for diagnosis of respiratory infections, they should consider that cost with respect to the overall cost of acute respiratory illness. Acute respiratory tract infections accounted for 219 per 10,000 ED visits from 1996 to 2010 in the United States (1). Moreover, there were 1,550 per 10,000 physician office and hospital outpatient department visits from 2002 to 2010 (2). These visits are often associated with a total of 150 million days lost from work and more than $10 billion in costs for medical care (3).
Viral pathogens are the most common cause of respiratory tract infections. Seasonal influenza contributes to substantial morbidity and mortality each year in the United States. In the 2012-13 influenza season, the CDC estimates that there were approximately 380,000 influenza-associated hospitalizations (4). Therefore, rapid diagnosis is important for timely intervention, especially when treatment exists for the pathogen identified, such as with influenza virus (5).
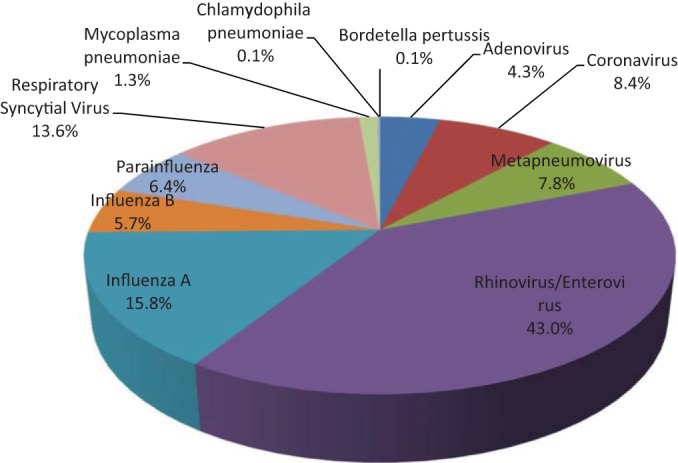
In a large proportion of patients with respiratory tract infections, other viruses and noncultivable bacteria have been found to cause substantial morbidity and mortality. In the period October 2013 through September 2014, our laboratory identified 1,528 positive specimens, of which only 242 (15.8%) were infections caused by influenza A virus (Fig. 1). An additional 1,286 respiratory pathogens were detected using our multiplex PCR assay. These known pathogens also contribute to the economic burden of health care; therefore, as for influenza virus, the rapid and accurate detection of these pathogens can greatly influence how physicians treat a respiratory infection. The difference in price between the two panels that we use at Loyola is $73.00. With our syndromic panel, the cost per analyte tested is $5.74. For our FLUPCR, the cost per analyte is $21.00. I would consider both of these tests to be great bargains. The additional $73.00 cost for performing the syndromic panel should not be considered a deterrent, given the additional information obtained and the fact that there is a 39% positivity rate, compared to 28% for FLUPCR. During the 8 months per year when influenza prevalence is low, syndromic panels should be offered as the only choice when respiratory illness testing is desired.
Incidence of viruses present in respiratory specimens at Loyola University Medical Center, 1 October 2013 to 27 September 2014. Note that the percentage total exceeds 100% because some samples contained multiple viruses.
Patient satisfaction.
Some will argue that detecting viruses other than influenza virus is not important because no treatment is available for the other viral agents. But a compelling reason for detecting other viruses is patient satisfaction. People do not go to the ED for a runny nose; they are usually sicker than they have ever been before from a respiratory illness, and to obtain a diagnosis in 1 to 2 h is a huge patient satisfier. Results of published satisfaction surveys can influence patients in the selection of a health care provider and can affect reimbursement from government and third-party payers. Providing continuity of care that is patient centered, efficient, and timely are the new goals of our medical center, and we believe these will have a major influence on patients in choosing a medical care provider. I would argue that a rapid diagnosis of the patient's illness goes a long way toward meeting our institution's goal of providing quality outcomes that lead directly to patient satisfaction.
Additional benefits of molecular multiplex respiratory virus panels.
Identifying noninfluenza respiratory viruses can provide epidemiologic tracking of local, regional, and national outbreaks. A recent example is the enterovirus D68 outbreak that occurred in late summer 2014. The increase in severe respiratory illness primarily in children could have been caused by many different viruses that are common during the late summer and fall. Hospitals in Missouri and Illinois were the first to document this increase, which was later identified to be caused predominantly by enterovirus D68 infection (6). The finding of Enterovirus in respiratory specimens was possible only because the sentinel hospitals were using molecular multiplex respiratory virus panels for routine testing in the clinical microbiology laboratory.
Once specific viruses are identified, appropriate infection control measures can be applied to admitted patients. Knowledge of the etiologic agent allows informed decisions about whether to use droplet and/or contact precautions and considerations for cohorting patients when isolation rooms become limited. As new pathogens emerge, the ability to exclude known viruses may help to more rapidly recognize and identify the presence of a new pathogen, such as Middle East respiratory syndrome coronavirus (MERS-CoV).
Cost analysis and silo mentality.
Decision-makers who are determining whether to allow or restrict the use of syndromic panels based on the individual test cost are thinking with a silo mentality. “Silo” refers to unit-based cost accounting and is the old way of managing hospital costs. If the business case for a new diagnostic test cannot be carved out of your department's budget, then it is not likely to be approved. Fortunately, the federal government via the Affordable Care Act is forcing medical executives to use outcome-based decision trees. Beginning in 2016, the Centers for Medicare & Medicaid Services (CMS) will move 40% of medical cost reimbursement to outcome-based payment. Outcome data will drive reimbursement in the future. The question to be asked is not how much does one test cost but rather how does the implementation of this test affect patient outcomes. When looking at patient outcomes in relationship to use of syndromic panels, several outcomes should be measured, as follows:
Quicker access to treatment
Shorter duration of symptoms
Less time out of work or school
Shorter emergency room times
Shorter hospital stay if admitted
Implementation of infection control measures, including cohorting of patients, the use or nonuse of isolation precautions based on the known etiologic agent
Reduction in pharmacy cost due to less antibiotic usage
Reduction in laboratory costs due to less need for additional follow-up tests, including additional diagnostic assays and determination of antibiotic peak and trough levels
Reduction in collateral side effects from antibiotics such as adverse drug reaction, Clostridium difficile infection, and adverse effects on the human microbiome such as intestinal dysbiosis
Reduction in total medical cost for the particular medical encounter
These types of outcome studies have not been done in the past and are difficult to perform because hospitals do not typically track these metrics (7). Such a study is under way at our facility, and the results will certainly influence our institution's decision going forward regarding the further implementation of syndrome-based molecular multiplex panels.
Conclusion.
My discussion has focused primarily on multiplex PCR respiratory virus panels, because that has been my experience to date. Our laboratory is currently gearing up to implement syndromic panels for the identification of bacteria and yeast species from positive blood culture bottles and panels for the identification of agents of gastrointestinal illness performed directly from stool samples. A future application that we eagerly await is the detection of infectious agents directly from cerebrospinal fluid (CSF). Syndromic, multiplex PCR panels offer the chance to have a definitive diagnosis in less than 2 h, allowing timely decisions about hospital admission, treatment, infection control, and patient return to work and family. They can be performed near the patient with minimal training and labor cost. Their use has the potential to reduce health care costs, and the rapidity of results is extremely satisfying to both patients and medical providers.
Paul C. Schreckenberger
ACKNOWLEDGMENTS
I have received research funding from BioFire Diagnostics and Cepheid and serve on the scientific advisory boards for Biofire Diagnostics, Cepheid, and GenMark Diagnostics.
3.Garibaldi RA.
1985.
Epidemiology of community-acquired respiratory tract infections in adults. Incidence, etiology, and impact. Am J Med
78(6B):32–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
4.Division of Emergency Operations, Office of Public Health Preparedness and Response, Centers for Disease Control and Prevention. 24
December
2013.
Note to clinicians: early reports of pH1N1-associated illnesses for the 2013-14 influenza season. CDC Health Advisory. http://emergency.cdc.gov/HAN/han00359.asp. [Google Scholar]
6.Centers for Disease Control and Prevention. 2014.
Severe respiratory illness associated with enterovirus D68–Missouri and Illinois, 2014. MMWR Morb Mortal Wkly Rep
63:798–799. [PMC free article] [PubMed] [Google Scholar]
7.Doern GV.
2014.
The value of outcomes data in the practice of clinical microbiology. J Clin Microbiol
52:1314–1316. doi: 10.1128/JCM.00712-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
In seeking continued “laboratory improvement” there is a great danger of establishing exhaustive microbiology as an end in itself…. This trend is discouraging to many microbiologists who recognize that the quality of their services will be more effectively improved through careful integration of what is technically feasible with what is clinically important.
—Raymond C. Bartlett, Medical Microbiology: Quality, Cost and Clinical Relevance (1)
Multiplex PCR panels that detect multiple pathogens that cause a common syndrome or are commonly found in a specific sample type are terrific. The ability to detect a large number of pathogens rapidly and with high sensitivity and specificity has the potential to transform clinical microbiology. But it is important that we carefully consider whether these tests should be front-line tests used for all patients with a syndrome or whether their use should be limited to specific patients. The primary issue related to this is which pathogens should be and are included in these panels. The point of this Counterpoint, then, is that the compositions of these panels should be appropriately linked to clinical syndromes and the pathogens that are likely to be present.
As laboratory leaders, many of us want to offer multiplex PCR panels, but we have limited control over which pathogens are included in the panels. Most laboratories lack the resources or expertise to design, troubleshoot, and validate multiplex PCRs to detect a large number of pathogens. Those labs that can undertake these tasks might consider that the FDA appears to be moving in the direction of limiting the clinical use of laboratory-developed tests (2). As a result of these factors, most of us are left choosing among commercial tests produced by a few companies, and therefore the composition of the panels we can offer is determined by the manufacturers that make them. These commercial panels are quite expensive for the patient or their payer, as well as for the laboratory. While we are not obliged to report (or even necessarily access) the results of testing for all the pathogens, it is wasteful of institutional resources to use an expensive panel that detects more than 20 pathogens and report only a few of them.
The fixed nature of the multiplex PCR panels raises the concern that they might include pathogens that cause infections different enough that simultaneous testing for those pathogens should be rare. Those differences might be in the clinical manifestations or epidemiology (risk factors) related to infection. Alternatively, the differences might be detectable by rapid, accurate, and inexpensive tests (e.g., the Gram stain) that are part of routine testing. Before I discuss the consequences of combining such pathogens into a single test, consider a few examples. Would you recommend routine, simultaneous testing for the following combinations of pathogens?
Stool samples for Clostridium difficile in combination with norovirus, Salmonella, Campylobacter species, and Shiga-toxin producing Escherichia coli
Nasopharyngeal samples for Chlamydophila pneumoniae in combination with rhinovirus, influenza viruses, and respiratory syncytial virus
Positive blood cultures with Gram-positive cocci in clusters seen microscopically for Staphylococcus aureus in combination with E. coli, Neisseria meningitidis, and Candida albicans
These combinations are currently available in large multiplex PCR panels from one or more manufacturers (3–7). These examples raise concerns about the routine use of these panels.
Testing for some pathogens should be guided by risk factors for infection.
Infection with C. difficile is associated with specific risk factors. Most important among these are exposure to antimicrobial agents, age, and hospital admission, but cancer chemotherapy, gastrointestinal surgery, and manipulation of the gastrointestinal tract are also risk factors for this infection (8). In contrast, the other pathogens mentioned are closely linked to foodborne transmission of infections; some of them are linked to specific foods (9, 10). In the majority of patients with diarrheal or related enteric disease, the history of risk factors for C. difficile infection can be used to determine whether testing for C. difficile is needed, and it will be a minority that will require simultaneous tests for C. difficile and the other infectious causes of enteric disease provided in the example (11). Furthermore, it is clear that colonization with C. difficile (including C. difficile with the toxin genes) occurs in some groups, such as young children and children with inflammatory bowel disease (12, 13). Interpretation of a positive result for C. difficile in a patient without risk factors for this infection can be difficult.
Testing for uncommon pathogens should usually follow testing for common pathogens.
Infection with Chlamydophila pneumoniae is uncommon enough that routine diagnostic testing is not recommended for community-acquired pneumonia in adults, although testing can be considered for patients with epidemiologic conditions or risk factors associated with the infection (14). Certainly there will be patients with specific risk factors who require testing for uncommon pathogens at the same time as testing for common pathogens. This might be most often the case for immunocompromised patients. But for most patients, negative test results for common pathogens should precede testing for uncommon pathogens in the interest of controlling the cost of testing for both the patient and the institution.
Tests should not be done when it is very, very unlikely that the pathogen is present.
It is hard to see a rationale behind performing a large, expensive multiplex panel that combines tests for Gram-positive bacteria, Gram-negative bacteria, and yeast species on blood culture broths when a Gram stain will indicate in which of these groups the culprit belongs. A focused PCR panel that is limited to organisms of similar Gram stain morphologies is more sensible (and at least one manufacturer offers such panels) (15, 16). One could argue that the large panel would be useful for detecting a second organism that is not seen in a Gram stain. Certainly there are a small percentage of cultures that have two species of organisms with one that is undetected by Gram staining, but culture with selective media can detect the second organism cheaply and usually within a day.
An additional concern is the modest sensitivities of the available large multiplex PCR panels for some pathogens. The sensitivity of two large multiplex PCR panels for respiratory viruses was approximately 85% for influenza A virus in one study, and one of the assays had a sensitivity of only 57% for adenovirus (5). One of the multiplex panels for gastrointestinal pathogens had a sensitivity of 48% for Yersinia enterocolitica in a recent study (4). This is nothing new to most of us: we dealt with similar challenges when using immunoassays to simultaneously test for multiple respiratory viruses (17). But it should remind us that we must consider whether to offer alternative tests for some pathogens when using multiplex tests and that we need to educate the clinical staff in the appropriate utilization of the test and interpretation of the results.
The effects of using large multiplex panels on laboratory costs and on overall cost of care are not yet clear. It is clear that the supply costs for large multiplex PCR panels are higher than those of conventional tests and that at least some of these assays significantly reduce labor costs; however, studies on the overall cost to laboratories have come to inconsistent conclusions (3, 18, 19). Although improvements in infection control and some associated cost savings could result from the reduced turnaround time of these tests and some studies have supported this (3), some have raised concern about whether the performance of the tests is adequate to guide infection control practices (20). There is real potential, I think, for the reduced turnaround time that these assays provide to result in reduced costs of care, but we need high-quality data to demonstrate or refute that.
I think we would be smart to follow Bartlett's concern (1) to its reasonable conclusion. The use of large multiplex panels for detection of an array of pathogens must be guided by careful consideration of which patients will benefit from the use of these tests. This requires discussion with clinical leadership, and that discussion should be primarily about patient care and outcomes. The cost of testing is an important concern as well, but it is secondary and should be taken in the context of the overall cost of the patient's care. Large multiplex PCR panels will be extremely useful in patient care, but it is important to make sure that we use them wisely.
Alexander J. McAdam
REFERENCES
1.Bartlett RC.
1974.
Medical microbiology: quality, cost and clinical relevance, p 4
Wiley Biomedical-Health, New York, NY. [Google Scholar]
2.Food and Drug Administration. 31
July
2014.
Anticipated details of the draft guidance for industry, Food and Drug Administration staff, and clinical laboratories on Framework for Regulatory Oversight of Laboratory Developed Tests (LDTs) and FDA Notification and Medical Device Reporting for Laboratory Developed Tests (LDTs). Food and Drug Administration, Silver Spring, MD:
http://www.fda.gov/downloads/MedicalDevices/ProductsandMedicalProcedures/InVitroDiagnostics/ucm407409.pdf. [Google Scholar]
3.Halligan E, Edgeworth J, Bisnauthsing K, Bible J, Cliff P, Aarons E, Klein J, Patel A, Goldenberg S.
2014.
Multiplex molecular testing for management of infectious gastroenteritis in a hospital setting: a comparative diagnostic and clinical utility study. Clin Microbiol Infect
20:O460–467. doi: 10.1111/1469-0691.12476. [DOI] [PubMed] [Google Scholar]
4.Khare R, Espy MJ, Cebelinski E, Boxrud D, Sloan LM, Cunningham SA, Pritt BS, Patel R, Binnicker MJ.
2014.
Comparative evaluation of two commercial multiplex panels for detection of gastrointestinal pathogens by use of clinical stool specimens. J Clin Microbiol
52:3667–3673. doi: 10.1128/JCM.01637-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
5.Popowitch EB, O'Neill SS, Miller MB.
2013.
Comparison of the Biofire FilmArray RP, Genmark eSensor RVP, Luminex xTAG RVPv1, and Luminex xTAG RVP fast multiplex assays for detection of respiratory viruses. J Clin Microbiol
51:1528–1533. doi: 10.1128/JCM.03368-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
6.Rand KH, Delano JP.
2014.
Direct identification of bacteria in positive blood cultures: comparison of two rapid methods, FilmArray and mass spectrometry. Diagn Microbiol Infect Dis
79:293–297. doi: 10.1016/j.diagmicrobio.2014.03.014. [DOI] [PubMed] [Google Scholar]
7.Altun O, Almuhayawi M, Ullberg M, Ozenci V.
2013.
Clinical evaluation of the FilmArray blood culture identification panel in identification of bacteria and yeasts from positive blood culture bottles. J Clin Microbiol
51:4130–4136. doi: 10.1128/JCM.01835-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
8.Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, Pepin J, Wilcox MH.
2010.
Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol
31:431–455. doi: 10.1086/651706. [DOI] [PubMed] [Google Scholar]
9.Gould LH, Walsh KA, Vieira AR, Herman K, Williams IT, Hall AJ, Cole D.
2013.
Surveillance for foodborne disease outbreaks—United States, 1998-2008. MMWR Surveill Summ
62:1–34. [PubMed] [Google Scholar]
10.Scallan E, Hoekstra RM, Angulo FJ, Tauxe RV, Widdowson MA, Roy SL, Jones JL, Griffin PM.
2011.
Foodborne illness acquired in the United States–major pathogens. Emerg Infect Dis
17:7–15. doi: 10.3201/eid1701.P11101. [DOI] [PMC free article] [PubMed] [Google Scholar]
11.DuPont HL.
2014.
Acute infectious diarrhea in immunocompetent adults. N Engl J Med
370:1532–1540. doi: 10.1056/NEJMra1301069. [DOI] [PubMed] [Google Scholar]
12.Lamouse-Smith ES, Weber S, Rossi RF, Neinstedt LJ, Mosammaparast N, Sandora TJ, McAdam AJ, Bousvaros A.
2013.
Polymerase chain reaction test for Clostridium difficile toxin B gene reveals similar prevalence rates in children with and without inflammatory bowel disease. J Pediatr Gastroenterol Nutr
57:293–297. doi: 10.1097/MPG.0b013e3182999990. [DOI] [PubMed] [Google Scholar]
14.Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM Jr, Musher DM, Niederman MS, Torres A, Whitney CG.
2007.
Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis
44(Suppl 2):S27–S72. doi: 10.1086/511159. [DOI] [PMC free article] [PubMed] [Google Scholar]
15.Martinez RM, Bauerle ER, Fang FC, Butler-Wu SM.
2014.
Evaluation of three rapid diagnostic methods for direct identification of microorganisms in positive blood cultures. J Clin Microbiol
52:2521–2529. doi: 10.1128/JCM.00529-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
16.Tojo M, Fujita T, Ainoda Y, Nagamatsu M, Hayakawa K, Mezaki K, Sakurai A, Masui Y, Yazaki H, Takahashi H, Miyoshi-Akiyama T, Totsuka K, Kirikae T, Ohmagari N.
2014.
Evaluation of an automated rapid diagnostic assay for detection of Gram-negative bacteria and their drug-resistance genes in positive blood cultures. PLoS One
9:e94064. doi: 10.1371/journal.pone.0094064. [DOI] [PMC free article] [PubMed] [Google Scholar]
17.Landry ML, Ferguson D.
2000.
SimulFluor respiratory screen for rapid detection of multiple respiratory viruses in clinical specimens by immunofluorescence staining. J Clin Microbiol
38:708–711. [DOI] [PMC free article] [PubMed] [Google Scholar]
18.Patel A, Navidad J, Bhattacharyya S.
2014.
Site-specific clinical evaluation of the Luminex xTAG gastrointestinal pathogen panel for detection of infectious gastroenteritis in fecal specimens. J Clin Microbiol
52:3068–3071. doi: 10.1128/JCM.01393-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
19.Dundas NE, Ziadie MS, Revell PA, Brock E, Mitui M, Leos NK, Rogers BB.
2011.
A lean laboratory: operational simplicity and cost effectiveness of the Luminex xTAG respiratory viral panel. J Mol Diagn
13:175–179. doi: 10.1016/j.jmoldx.2010.09.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
Highly multiplexed molecular tests have clinical value; they provide a syndromic approach to diagnostics, which is particularly useful for infections in which it is not possible to determine the etiologic agent based only on symptoms.
The use of highly multiplexed tests is more closely aligned with traditional culture methods, where clinicians do not need to identify a specific pathogen for testing but rather think in broad terms about whether there is a bacterial infection in the respiratory tract or the blood.
Rapid sensitive diagnostic tests have the potential to transform the medical management of patients with infectious diseases.
Multiplex tests should be developed in consultation with clinical microbiologists and clinicians so that the panel members reflect clinical reality.
Implementation of panel tests should be done in consultation with clinicians, so there is a clear understanding of the appropriate use and interpretation of test results.
Issues to be resolved
A rapid, accurate diagnosis of viral respiratory infection will likely decrease the use of antibiotics and allow for a more targeted approach to using antivirals, although outcome studies are needed in this area.
The value of using highly multiplexed tests as front-line diagnostics will depend on the clinical situation: while it is easier to justify panel testing for respiratory viruses, it is more difficult when the panel includes pathogens that are very rare, when all pathogens in the panel do not cause overlapping clinical syndromes, or when some pathogens are found only in specific patient populations (immunocompromised patients).
Understanding the performance characteristics of all members of the panel is essential, as the sensitivity and specificity for the detection of each pathogen may vary. The prevalence of the pathogen will greatly affect the positive and/or negative predictive value of the test.
Cost assessments of panel tests need to consider the overall cost or cost savings to the health care system, not just the cost of the test to the microbiology laboratory. Factors to consider include decreased use of antibiotics, decreased ancillary testing, decreased length of stay in the hospital or emergency department, and time off work.
Angela M. Caliendo, Editor, Journal of Clinical Microbiology