

Abstract
Background
Patient-centered communication is a core competency in modern health care and associated with higher levels of patient satisfaction, improved patient health outcomes, and lower levels of burnout among physicians. The objective of the present study was to develop a questionnaire assessing medical student and physician self-efficacy in patient-centeredness (SEPCQ) and explore its psychometric properties.
Methods
A preliminary 88-item questionnaire (SEPCQ-88) was developed based on a review of the literature and medical student portfolios and completed by 448 medical students from Aarhus University. Exploratory Principal Component analysis resulted in a 27-item version (SEPCQ-27) with three underlying self-efficacy factors: 1) Exploring the patient perspective, 2) Sharing information and power, and 3) Dealing with communicative challenges. The SEPCQ-27 was completed by an independent sample of 291 medical students from 2 medical schools and 101 hospital physicians.
Results
Internal consistencies of total and subscales were acceptable for both students and physicians (Cronbach’s alpha (range): 0.74–0.95). There were no overall indications of gender-related differential item function (DIF), and a Confirmatory Factor Analysis (CFA) indicated good fit (CFI = 0.98; NNFI = 0.98; RMSEA = 0.05; SRMR = 0.07). Responsiveness was indicated by increases in SEPCQ scores after a course in communication and peer-supervision (Cohen’s d (range): 0.21 to 0.73; p: 0.053 to 0.001). Furthermore, positive associations were found between increases in SEPCQ-scores and course-related motivation to learn (medical students) and between SEPCQ scores and years of clinical experience (physicians).
Conclusions
The final SEPCQ-27 showed satisfactory psychometric properties, and preliminary support was found for its construct validity, indicating that the SEPCQ-27 may be a valuable measure in future patient centered communication training and research.
Background
It is generally agreed that the quality of the patient-clinician relationship is important for providing and receiving excellent care, for the healing process, and for health-related outcomes [1–3], and that patient-centeredness is a central aspect of high quality health care [4]. Several terms, including “patient-centered communication”, “patient-centered care”, and “patient-centered medicine” are often used interchangeably, and it has been proposed that the term “patient-centeredness” should be reserved to describe a general moral philosophy of health care with three core attributes: a) consideration of patients’ needs, perspectives, and individual experiences, b) provision of opportunities to patients to participate in their care, and c) enhancement of the patient-clinician relationship [4, 5]. Patient-centered communication can be defined as the processes and communicative behaviors exhibited by clinicians that promote these core values. One operational definition includes: a) Eliciting and understanding the patient’s perspective – concerns, ideas, expectations, needs, feelings, and functioning, b) understanding the patient within his or her unique psychosocial context, c) reaching a shared understanding of the problem and its treatment with the patient that is concordant with his or her values, and d) helping patients to share power and responsibility by involving them in choices to the degree that they wish [5]. Other similar definitions are available [6, 7].
Over the years, a growing body of research has explored the possible influence of patient-centered communication on various patient outcomes. Several systematic reviews, both narrative [8–12] and quantitative, using either simple vote counting [13] or meta-analytic approaches [14–17] focusing on various types communicative behaviors, different types of clinicians, and a variety of patient populations have been published. The most frequently studied patient outcomes are patient satisfaction and adherence to treatment, with results of meta-analyses generally showing medium effect sizes. Associations with patient health outcomes, on the other hand, are less frequently studied. The available studies also provide support for the effectiveness of communication skills training in the form of improved communicative behaviors of clinicians [18] and higher patient satisfaction [19], whereas the effects in terms of patient outcomes [20–22] are mixed. While most of the studies have focused on physicians, there is also some research on the promotion of communicative skills among medical students, and the results of a meta-analysis [23] suggests that certain teaching methods, e.g. small group teaching, yield relative large effects. As the foundation of patient-centered approaches among future physician, including the attitude towards the physician-patient relationship and basic communicative skills, is likely to be laid in medical school, more research in this important areas is needed.
Patient-centered behaviors have also been found associated with physician well-being. It has, for example, been found that physicians with high levels of stress and burnout engage less in developing the relationship with the patient [24, 25] and that training physicians the skills of mindful practice reduce their level of burnout, improve their job satisfaction, and their levels of empathy; factors that are associated with the ability to engage with patients in a patient-centered manner [26]. These findings suggest that the mental health of physicians’ is associated with their communicative skills and their ability to focus effectively and empathically in their interactions with patients [27]. Taken together, the relatively sparse literature suggests a complex bi-directional relationship between physician burnout, communication skills, and patient satisfaction.
Concurrent with the growing evidence, the development and maintenance of skills in patient-centered communication has become an important element in medical education, making it increasingly relevant to assess different aspects of patient-centeredness, both as outcomes of communication training and as predictors of patient and physician outcomes. Although communication-related competencies are often assessed with interaction analysis systems evaluating observed verbal and nonverbal communicative behaviors [28], such assessments are complex and time consuming. There is therefore a need for practical and valid questionnaire-based methods to assess competencies in patient-centeredness.
With respect to the attainment of knowledge, attitudes, and skills, there is increasing attention towards the role that the person’s beliefs play in this process. Self-efficacy, a key term in social cognitive theory, has been defined as confidence or “beliefs in one’s capabilities to organize and execute the courses of action required to produce given attainments” [29, 30], and a growing body of research has confirmed that self-efficacy is likely to affect the individual’s behavior in such key aspects as the tasks and approaches they choose, their exertion, perseverance, and performances. In research of physician communication skills and communications skills training, outcomes have often been assessed as levels and changes in the physician’s confidence in various communication skills, e.g. general interviewing skills [31, 32], communicating bad news to oncology patients [33], behavioral counseling skills for multiple risk factor modification [34], and in dealing with mental health problems presented in general practice [35]. The outcomes, however, have usually been assessed with various ad-hoc-developed measures, including a frequently used 9-item measure [32], and - to the best of our knowledge - a validated and psychometrically sound instrument to measure self-efficacy in exhibiting all core aspects of patient centered behaviors and attitudes for use in medical education and physician-patient communication research has so far not been available. Our aim was therefore to develop a Self-Efficacy in Patient Centeredness Questionnaire and to provide preliminary evidence for its reliability and validity in medical students and physicians.
Methods
Procedure and participants
The development and preliminary validation of the Self-Efficacy in Patient Centeredness Questionnaire (SEPCQ) was guided by the quality criteria developed by the Scientific Advisory Committee of the Medical Outcomes Trust (MOT) [36] and conducted in seven steps involving five samples totaling 749 medical students and 108 physicians (Fig. 1).
Fig. 1.
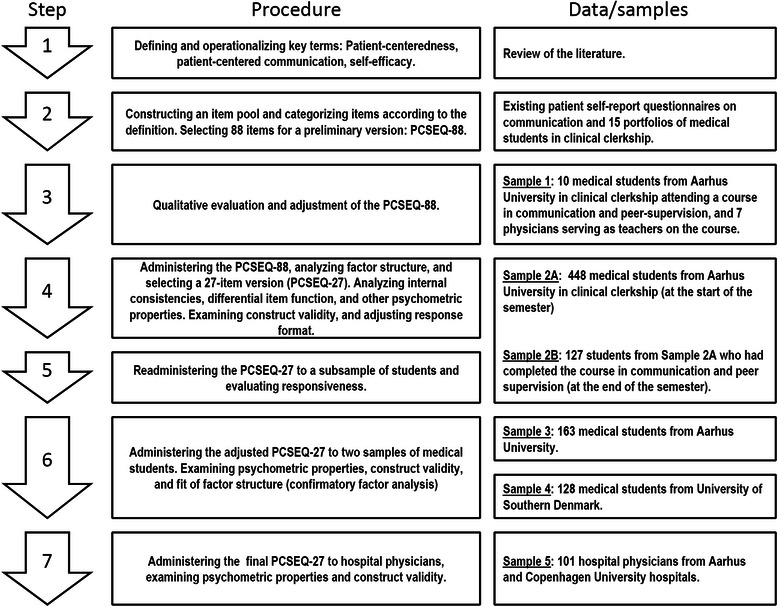
Overview of the development and validation procedure for the Patient-Centeredness Self-Efficacy Questionnaire (SEPCQ)
Step 1: defining patient-centeredness self-efficacy
Based on a review of the literature, we chose a general definition of patient-centeredness as exhibiting three core attributes: 1) “Considering the patients’ needs, wants, perspectives, and individual experiences”, 2) “offering patients opportunities to provide input into and participate in their care”, and 3) “enhancing the partnership and understanding in the patient-physician relationship” [5]. This definition was supplemented with definitions presented by Stewart and colleagues [6], which resulted in an operational definition of patient-centered communication as being characterized by the following five physician behaviors: 1) Eliciting, understanding, and validating the patient’s perspective (e.g. concerns, feelings, expectations, values). 2) Viewing the patient’s health status, disease, and symptoms from a bio-psycho-social perspective (e.g. life history, developmental issues, employment, community), 3) Reaching a shared understanding of the patient’s problem and its treatment, taking into consideration the patient’s priorities, the aims of treatment, and the roles of patient and physician, 4) Helping the patient share power by offering meaningful involvement in choices relating to his or her health. 5) Enhancing the patient-doctor relationship by focusing on compassion, healing, sharing power, quality-of-life, self-awareness, and transference.
Following Bandura’s definition [30], medical student or physician patient-centeredness self-efficacy was defined as his or her confidence in his or her ability to exert each particular behavior in a manner so that the patient would perceive it according to its underlying intention. Items would thus be worded as: “I am confident that I am able to make the patient experience me as (specific behavior covered by the item)”.
Step 2: constructing an item pool
A large initial item pool was then constructed based on: a) items from five available published patient questionnaires [37–41] and b) communication-related issues and behaviors described in 15 portfolios produced by medical students in clinical clerkship at university hospital clinics who attended a course on communication and peer-supervision. Four of the authors independently selected relevant behaviors and issues and categorized them according to the five behavioral characteristics listed above or – if needed – into additional categories. A preliminary pool of 88 items was then negotiated with items grouped into 6 initial domains: 1) Exploring the patient perspective (21 items), 2) Viewing the patient’s problem from a bio-psycho-social perspective (e.g. background, life situation) (9 items), 3) Establishing a shared understanding of the disease, examinations, and treatment (9 items), 4) Helping the patient to influence his/her care (15 items), 5) Enhancing the physician/medical student-patient relationship (20 items), and 6) Self-reflection and dealing with communicative challenges (14 items).
Step 3: SEPCQ construction and preliminary evaluation
The first 88-item version of the SEPCQ (SEPCQ-88) was then constructed. A 7-point Likert scale was used with “0” (to a very low degree) and “6” (To a very high degree) as endpoints. The middle score “3” was anchored with “Neither/nor”. A general instruction was developed emphasizing that the questions covered neither the actual behavior nor the desirability of the behavior but rather the respondent’s confidence in exhibiting each particular behavior so that patients will experience the described behavior as intended. (See instructions in Table 1). Two authors then evaluated the instructions, response categories, and wordings of items using the QAS-99 Question Appraisal System [42] leading to some minor adjustments. The SEPCQ-88 was then administered to 10 students and 7 physicians (Sample 1), who were interviewed about the relevance, acceptability, and understandability of the instructions and items, leading to some final adjustments.
Table 1.
The Self-Efficacy in Patient Centeredness Questionnaire (SEPCQ-27): Instructions, item wordings, factor loadings, and differential item function (DIF)
| Items: I am confident that I am able to … | Factor 1: Exploring the patient perspective | Factor 2: Sharing information and power | Factor 3: Dealing with communicative challenges | DIF-MH | DIF-IRT |
|---|---|---|---|---|---|
| ETC.-category c | K-index d | ||||
| 1. Make the patient feel that I am genuinely interested in knowing what he/she thinks about his/her situation | 0.69 | 0.18 | 0.21 | A | 0.15 |
| 2. Make the patient feel that I have time to listen | 0.66 | 0.28 | 0.21 | A | 0.13 |
| 3. Recognize the patient’s thoughts and feelings | 0.69 | 0.18 | 0.30 | A | 0.06 |
| 4. Be attentive and responsive | 0.74 | 0.25 | 0.15 | A | 0.13 |
| 5. Be aware of when the patient is scared or concerned | 0.62 | 0.26 | 0.32 | A | 0.14 |
| 6. Treat the patient in a caring manner | 0.77 | 0.26 | 0.08 | A | 0.04 |
| 7. Make the patient experience me as empathetic | 0.81 | 0.19 | 0.13 | A | 0.08 |
| 8. Make the patient feel that he/she can talk with me about confidential, personal issues | 0.64 | 0.28 | 0.27 | A | 0.04 |
| 9. Show a genuine interest in the patient and his/her situation | 0.80 | 0.23 | 0.18 | A | 0.10 |
| 10. Focus on compassion, care and symptomatic treatment, when there is no curative treatment | 0.71 | 0.25 | 0.18 | A | 0.06 |
| 11. Record a complete medical history | 0.19 | 0.56 | 0.15 | A | 0.13 |
| 12. Reach agreement with the patient about the treatment plan to be implemented | 0.27 | 0.60 | 0.24 | A | 0.14 |
| 13. Advise and support the patient in making decisions about his/her treatment b | 0.34 | 0.60 | 0.27 | A | 0.10 |
| 14. Ensure that the patient makes his/her decisions on an informed basis | 0.25 | 0.71 | 0.27 | A | 0.18 |
| 15. Explain the diagnosis and treatment plan to the patient so that he/she understands | 0.17 | 0.73 | 0.10 | A | 0.12 |
| 16. Explain things so that the patient feels well-informed | 0.35 | 0.76 | 0.15 | A | 0.07 |
| 17. Inform the patient about the expected side effects, so the patient understands them | 0.30 | 0.65 | 0.22 | A | 0.13 |
| 18. Explain how the treatment works or is expected to work | 0.12 | 0.82 | 0.13 | A | 0.10 |
| 19. Explain how the treatment is likely to affect the patient's condition, so that the patient understands | 0.25 | 0.79 | 0.16 | A | 0.06 |
| 20. Explain the treatment procedures, so that the patient understands them | 0.18 | 0.83 | 0.13 | A | 0.07 |
| 21. Accept when there is no longer curative treatment for the patient | 0.10 | 0.23 | 0.63 | A | 0.20 |
| 22. Be aware of when my own feelings affect my communication with the patient | 0.22 | 0.14 | 0.70 | A | 0.11 |
| 23. Deal with my own emotional reactions when the situation is difficult for me | 0.16 | 0.11 | 0.68 | A | 0.28 |
| 24. To maintain the relationship with the patient when he/she is angry | 0.22 | 0.14 | 0.65 | A | 0.11 |
| 25. To stay focused on what is best for the patient if there is a professional disagreement about the diagnosis and treatment b, c, d | 0.10 | 0.34 | 0.62 | B | 0.34 |
| 26. Avoid letting myself be influenced by preconceptions about the patient d | 0.25 | 0.10 | 0.68 | A | 0.32 |
| 27. Separate my personal views from my approach in the professional situation | 0.21 | 0.11 | 0.69 | A | 0.03 |
Instructions: In the following, a number of statements describing different aspects of how physicians and medical students can relate to and communicate with patients are presented. Please read each statement carefully and judge how confident you are in your ability to relate to and communicate with patients in the manner described in the statement. Please answer all questions and provide your best assessment of how confident you are that you will be able to behave in the way described in the statement. Please answer as honestly and sincerely as possible. Remember that each question must be answered based on how confident you are that you will be able to make the patient experience the particular behavior - not the extent to which you would like to be able to engage in the behaviora
a)English translation-backtranslation: The original Danish item wordings were translated independently into English by two English-speaking persons, and following a backtranslation, a final English version was negotiated
b)Two items (13 and 25) did not meet the primary criterion (difference between the highest and second highest loading ≥ 0.30), but were retained in the model on the basis of content analysis. The remaining 25 items met both criteria: Loading ≥ 0.50; difference between highest and second highest loading ≥ 0.30
c)Mantel-Haenszel Chi-Square Differential item function (DIF) analysis: Negligible gender-related DIF (A) for all items except item 25 (moderate DIF = B) in favor of men (Zieky, 1993)
d)IRT DIF-analysis: K-index (Kumagai, 2012) for item 25 and 26 exceeded the criterion of 0.30 with possible gender-bias in favor of men (item 25) and women (item 26)
Step 4–7: psychometric evaluation procedure
The SEPCQ-88 was first completed by Sample 2A (see Fig. 1 for brief description of samples) and completed again a second time by Sample 2B. The psychometric properties of the full SEPCQ-88 were evaluated, leading to a revised 27-item version (SEPCQ-27) with changes made to the scoring format (from a 7-point to a 5-point Likert scale) (see Results for further details). The SEPCQ-27 was then administered to two new student samples (Sample 3 and 4) and a sample of hospital physicians (Sample 5) and subjected to further evaluation.
Additional measures
All students were asked to report age, gender, and current semester. Physicians were asked to report age, gender, department, current position, year of graduation from medical school, and whether they had attended the standard patient-communication training course offered by the Danish Medical Association (DMA).
All students completed the Medical Student Well-Being Index (MSWBI) [43], a 7-item measure of medical student distress.
Students from Sample 2A who were scheduled to attend the course in communication and peer-supervision also completed a Course-Related Motivation to Learn questionnaire (CRMTL) (10 items) and a Course-related Self-Efficacy questionnaire (CRSE) (5 items), both adapted from the Motivated Strategies for Learning Questionnaire (MSLQ) [44]. The CRMTL assessed the students’ motivation to take the course. Sample item: “In a course like this, I prefer exercises that really challenge me, so that I can learn new things”, and the CRSE measured expectancy regarding how well he/she would do on the course. Sample item: “I expect to do exceptionally well on this course”. Internal consistencies (Cronbach’s Alpha) in the present sample were 0.86 (CRMTL) and 0.84 (CRSE).
Sample 3 and 4 also completed a 12-item version of the Marlowe Crowne Social Desirability Scale (MCSDS) [45] as a measure of possible response bias, i.e., the likelihood of reporting behaviors and responses that are culturally sanctioned but relatively unlikely. The MCSD-12 has previously displayed moderate, but acceptable, internal consistencies (KR-20: 0.69-0.71) in Danish university students (N = 457) (unpublished data) and showed satisfactory internal consistency in the present sample (KR-20: 0.73).
Analytical strategy
Identifying the factor structure
The possible underlying factor structure was explored as recommended [46] with a series of Principal Components Analyses with Varimax rotation and Eigenvalues >1 as criterion. Factor loadings were required to be >0.50 and the difference between the highest and second-highest factor loading at least 0.30. Items with differences in factor loadings between 0.20 and 0.29 were reviewed as possible items. A subsequent series of Principal Components analyses restricted to extract 7, 6, 5, 4, and 3 factors (fixed factor analyses) were then conducted. The factors were identified using the following criteria: a) Consistency in factor loadings across the six analyses and b) the item content should consistently reflect the same underlying factor. A final Principal Component Analysis with the selected items was then conducted to verify the model.
Reliability
Score distributions, ranges, means, and standard deviations of each item, the sum scores of the three derived subscales, and the total score were reviewed. Internal consistencies (Cronbach’s alpha) were calculated together with the baseline to14-16 weeks test-retest correlation for students who had completed the SEPCQ both before and after a course in communication and peer-supervision (Sample 2B).
Differential Item Function (DIF)
If DIF is present for an item, this could indicate measurement bias, i.e. that individuals from different groups with the same underlying ability (latent trait) differ in their likelihood to respond in a certain way to an item [47]. DIF analysis was used to evaluate possible gender-related measurement bias of the 27 selected items using both the Mantel-Haenszel (MH) Chi-Square [48] and an Item-Response-Theory (IRT)-based approach [49, 50]. The MH approach was based on the following criteria: 1) The MH Chi-Square (MH-CHI), 2) the MH Common Log-Odds Ratio (MH-LOR), 3) The standard error of MH-LOR (LOR SE), 4) the Standardized MH Log-Odds Ratio (LOR Z), and 5) the Breslow-Day Chi-Square (BD) (critical values: 3.84; p < 0.05). The Combined Decision Rule (CDR) suggests acceptable results if none of the above parameters reach statistical significance. The ETS Categorization Scheme represents consensus about DIF size (A = negligible, B = moderate, C = large) [51]. The IRT-based approach was based on the K-index for polytomous data [52]. If K > ((N categories–1) × 0.1), a large DIF is assumed. The lowest response categories (0–3) had many instances of “0” frequency, and as IRT does not allow “0” frequency, the scores were recoded: 0-3 = 1, 4 = 2, 5 = 3, and 6 = 4. The K-index cutoff was therefore ((4–1) × 0.1) = 0.3. Items with a K-index > 0.3 were assumed to have DIF.
Confirmatory factor analysis (CFA)
The fit of the three-factor SEPCQ-27 version was evaluated with CFA of the data collected from the independent Sample 4 from a different medical school. Five commonly used goodness-of-fit indices were used to evaluate the model with Robust Maximum Likelihood estimation: The Satorra-Bentler Scaled Chi-Square (S-B-Chi-Square), the Comparative Fit Index (CFI), the Non-Normed Fit Index (NNFI), the Root Mean Square Error of Approximation (RMSEA), and the Standardized Root Mean Square Residual (SRMR) [53, 54]. The model was interpreted as providing a reasonable good fit given a statistically significant S-B chi-square, CFI and NNFI > 0.95, RMSEA < 0.06, and SRMR < 0.08.
Construct validity was explored by examining associations with background variables (age, gender, experience) and scores on the CRMTL, CRSE, and MSWBI. SEPCQ scores were expected to be positively correlated with: a) Older age and female gender (students) and b) older age, more experience, and previous communication training (physicians). We also expected c) that higher levels of distress (MSWBI) would be associated with lower SEPCQ-scores, and d) that physicians would present higher scores than students. Testing responsiveness, we expected e) that completing the course in communication and peer-supervision would be associated with increased post-course SEPCQ scores. We also expected f) that higher pre-course CRMTL and CRSE scores would be independently associated with greater increases in SEPCQ scores.
Ethics
All data were collected anonymously. In Denmark, studies involving questionnaire-based data only are not subjective to ethical approval by the Regional Ethics Committees.
Statistical software
The majority of the analyses were conducted with IBM SPSS Statistics version 21. The confirmatory Factor analysis (CFA) was conducted with LISREL, version 8.80. Mantel-Haenszel Chi-Square DIF analyses were conducted with DIFAS version 4.0. [48], and IRT-based DIF analyses with EasyDIF version 0.1.6 [52].
Results
Step 4 and 5
A total of 520 out of approximately 660 7th to 10th semester students (Sample 2A) were present at the lectures where the SEPCQ-88 was handed out. A total of 448 (86.2 %) questionnaires with complete or almost complete data were returned. Number of missing items ranged from 2.2 % to 2.8 %.
Factor structure
The first Principal Components analysis converged after 17 iterations with 14 factors explaining 64.2 % of the variation. A Scree plot indicated a flattening of the slope with more than 3 factors, and the subsequent (fixed factor) Principal Component Analyses (data not shown) resulted in a preliminary 27-item 3-factor model, which was then subjected to a final Principal Components analysis. The model converged after 5 iterations explaining 58.9 % of the variation. A content analysis suggested the following three underlying dimensions of Self-Efficacy in Patient Centeredness: Factor 1: Exploring the patient perspective (10 items from the initial domains 1 and 5), Factor 2: Sharing information and power (10 items from domains 3 and 4), and Factor 3: Dealing with communicative challenges (7 items from domain 6). Only one item from the initial domain 2 was included (in Factor 2). Mean factor loadings for Factor 1–3 were 0.71, 0.71, and 0.66 respectively, and the average differences between the highest and second highest loadings were 0.46, 0.46, and 0.44. The final 3-factor model is shown in Table 1. Sample characteristics are shown in Table 2.
Table 2.
The Self-Efficacy in Patient Centeredness Questionnaire. First 88-item version (SEPCQ-88) and final 27-item (SEPCQ-27): Sample characteristics and descriptive data
| Total N: 857 | Score range | Sample 1 | Sample 2A | Sample 2B | Sample 3 | Sample 4 | Sample 5 |
|---|---|---|---|---|---|---|---|
| Participants | Medical students + physicians | Medical students | Physicians | ||||
| N | - | 10 + 7 | 448 | (127) | 163 | 128 | 101 |
| Questionnaires: | - | SEPCQ-88 | SEPCQ-88, MSWBI, CRMTL, CRSE | SEPCQ-88a | SEPCQ-27, MCSD-12, CRMTL, CRSE | SEPCQ-27, MCSD-12 | SEPCQ-27 |
| Semester | - | 8 | Mixed | 8 | 8 | Mixed | NA |
| Men, N (%) | - | 5 (29.4 %) | 90 (29.7 %) | 38 (30.0 %) | 52 (31.9 %) | 31 (24.2 %) | 32 (31.7 %) |
| Age, Mean (SD) | - | - | 24.8 (2.1) | 24.6 (1.8) | 24.7 (1.6) | 25.6 (3.9) | 41.7 (10.4) |
| Years of experience, Mean (SD) | - | - | - | - | - | - | 13.9 (10.8) |
| SEPCQ-Factor 1, Mean (SD) | 0-40 | - | 27.8 (7.4) | 29.0 (6.3) | 18.6 (4.2) | 21.3 (5.4) | 32.4 (4.5) |
| SEPCQ-Factor 2, Mean (SD) | 0-40 | - | 23.9 (7.9) | 26.8 (6.5) | 15.2 (5.1) | 15.6 (6.3) | 31.9 (4.9) |
| SEPCQ-Factor 3, Mean (SD) | 0-28 | - | 12.6 (6.0) | 14.3 (5.4) | 7.0 (4.0) | 8.3 (4.0) | 19.7 (3.7) |
| SEPCQ-27 Total, Mean (SD) | 0-108 | - | 64.2 (18.0) | 70.1 (15.0) | 40.9 (10.6) | 45.1 (13.5) | 83.9 (11.4) |
| MCSD-12, Mean (SD) | 0-12 | - | - | - | 1.5 (0.1) | 2.2 (0.2) | - |
| CRMTL, Mean (SD) | 10-70 | - | 49.2 (9.6) | - | 47.6 (10.4) | - | - |
| CRSE, Mean (SD) | 5-35 | - | 22.9 (5.1) | - | 22.0 (4.9) | - | - |
| MSWBI, Mean (SD) | 0-7 | - | 1.6 (2.1) | - | 1.3 (1.6) | - | - |
SEPCQ- Factor 1 (Exploring the patient perspective); SEPCQ- Factor 2 (Sharing information and power); SEPCQ- Factor 3 (Dealing with communicative challenges); MCSD-12 (Marlowe-Crowne Social Desirability Scale, 12-item Short Version); CRMTL (Course-Related Motivation to Learn); CRSE (Course-Related Self-Efficacy); MSWBI (Medical Student Well-Being Index)
a)SEPCQ data recoded from the original 7-point Likert scale format (0–6) into a 5-point Likert scale format (0–4) to allow for comparison of SEPCQ-88 and SEPCQ-27 data
Psychometric properties of SEPCQ-27
The score distributions of each item, each factor, and the total scale were inspected. Item response frequencies for the three lowest scoring categories (0–2) were low with average cumulative item response frequencies (scoring category 0 + 1 + 2) of 2.9 %, 5.7 %, and 17.6 % for Factor 1, 2, and 3 respectively. Furthermore, when inspecting the score distributions of the factors and total scales, Factor 1 and 2 appeared relatively skewed in the positive direction.
Internal consistencies (Cronbach’s Alpha) ranged between 0.83 and 0.94 (see Table 3), correlations between subscales ranged between 0.50 and 0.60, and subscale-to-total scale correlations ranged between 0.78 – 0.86 (see Table 4). The 14–16 week retest correlations for Factor 1, 2, 3, and total SEPCQ-27 were 0.62, 0.47, 0.69, and 0.87 respectively (p < 0.01) (Sample 2B).
Table 3.
The Self-Efficacy in Patient Centeredness Questionnaire (SEPCQ-27). Internal consistencies (Cronbach’s Alpha)
| Medical students | Physicians | |||
|---|---|---|---|---|
| Items | Sample 2A | Sample 3 + 4 | Sample 5 | |
| N | 448 | 291 | 101 | |
| SEPCQ- Factor 1 | 10 | 0.93 | 0.85 | 0.90 |
| SEPCQ- Factor 2 | 10 | 0.92 | 0.90 | 0.93 |
| SEPCQ- Factor 3 | 7 | 0.83 | 0.74 | 0.84 |
| SEPCQ-27 Total | 27 | 0.94 | 0.92 | 0.95 |
SEPCQ- Factor 1 (Exploring the patient perspective); Factor 2 (Sharing information and power); Factor 3 (Dealing with communicative challenges)
Table 4.
The Self-Efficacy in Patient Centeredness Questionnaire (SEPCQ-27). Factor inter-correlations and correlations with age, course-related motivation to learn (CRMTL), course-related self-efficacy (CRSE), social desirability (MCSD-12), and age and years of experience (physicians)
| SEPCQ - factor 1 | SEPCQ - factor 2 | SEPCQ - factor 3 | SEPCQ-27 total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical students | Phys. | Medical students | Phys. | Medical students | Phys. | Medical students | Phys. | |||||
| Sample | 2Aa | 3 + 4 | 5 | 2Aa | 3 + 4 | 5 | 2Aa | 3 + 4 | 5 | 2Aa | 3 + 4 | 5 |
| SEPCQ-Factor 2 | 0.60** | 0.59** | 0.65** | - | - | - | - | - | - | - | - | - |
| SEPCQ- Factor 3 | 0.54** | 0.55** | 0.52** | 0.50** | 0.58** | 0.74** | - | - | - | - | - | - |
| SEPCQ-27 Total | 0.86** | 0.85** | 0.84** | 0.86** | 0.88** | 0.92** | 0.78** | 0.80** | 0.84** | - | - | - |
| CRMTLb | 0.53** | - | - | 0.21 | - | - | 0.40** | - | - | 0.49** | - | - |
| CRSEb | 0.55** | - | - | 0.34** | - | - | 0.46** | - | - | 0.58** | - | - |
| MSWBI | −0.14** | - | - | −0.18** | - | - | −0.25** | - | - | −0.22** | - | - |
| MCSD-12 | - | 0.27** - | - | - | 0.06 | - | - | 0.20** - | - | - | 0.20** - | - |
| Agec | 0.07 | 0.15* | 0.14 | 0.08 | 0.17** | 0.36** | 0.16** | 0.21** | 0.49** | 0.12* | 0.18** | 0.36** |
| Experience (yrs) | - | - | 0.20* | - | - | 0.40** | - | - | 0.50** | - | - | 0.36** |
| Age (yrs) (Adjusted for experience)d | - | - | −0.09 | - | - | −0.01 | - | - | 0.09 | - | - | −0.01 |
| Experience (yrs) (Age adjusted)d | - | - | 0.17 | - | - | 0.19 | - | - | 0.16 | - | - | 0.41** |
SEPCQ-Factor 1: Exploring the patient perspective; SEPCQ-Factor 2: Sharing information and power; SEPCQ-Factor 3: Dealing with communicative challenges; MCSD-12: Marlowe-Crowne Social Desirability Scale, 12-item short version; CRMTL: Course-Related Motivation to Learn; CRSE: Course-Related Self-Efficacy; MSWBI: Medical Student Well-Being Index
a)Correlations for Sample 2A (N = 463) calculated with recoded (0–4) response categories to increase comparability with Sample 3 + 4 (N = 291)
b)CRMTL, CRSE: Results only for 8th semester students prior to taking the course in communication and peer-supervision
c)Wider age distribution in Sample 3 + 4 than 2A
d)Partial correlations
*)p < 0.05; ** p < 0.01
DIF analysis was conducted with women (N = 358) as reference group and men (N = 90) as focal group using the MH Chi-Square approach. Based on the Combined Decision Rule (CDR) and the ETS Categorization Scheme [51], almost all items had negligible gender-related DIF (category A). The exception was item 25 (“I am confident that I am able to stay focused on what is best for the patient if there is a professional disagreement about the diagnosis and treatment”) which showed moderate item bias (B) in favor in men, i.e. the item was “easier” for men than women. The IRT-based DIF analysis generally confirmed the results of the MH Chi-Square approach. No K-index values for any items in Factor 1 and 2 exceeded the criterion of 0.3. Two items in Factor 3: item 25 (see above) and item 26 (“I am confident that I am able to avoid letting myself be influenced by preconceptions about the patient”) showed indications of DIF with values slightly exceeding 0.30 (K = 0.34 and 0.32). The Item Characteristic Curves of men and women indicated that item 25 showed a tendency towards favoring men, while item 26 appeared to favor women. The average K-index values for factors 1, 2, and 3 were 0.09, 0.11, and 0.20 respectively. The results of the DIF analyses are shown in Table 1.
Construct validity
One-way ANOVA’s showed that 10th semester students (Sample 2A), who had not had any communication training, had lower scores than the remaining students. A total of 41 students (10.0 %) with non-Danish ethnicity exhibited lower scores than Ethnic Danish students (statistically non-significant). T-tests for independent samples indicated that men (N = 90) had slightly higher scores than women (p < 0.05) for Factor 2, Factor 3, and the Total scale, but not Factor 1 (mean differences: 2.4 to 4.6) (data not shown).
As seen in Table 4, small, but positive, correlations were found between age and SEPCQ scores (r = 0.07 – 0.16), with correlations with Factor 3 and SEPCQ total scores reaching statistical significance (p < 0.05). Students with higher levels of psychological distress (MSWBI) tended to have lower SEPCQ scores. In students, who were scheduled to take the course in communication and peer-supervision, both CRMTL and CRSE were positively associated with higher scores on the SEPCQ at the beginning of the semester. SEPCQ-scores increased for students who also completed the SEPCQ after completing the course, with changes corresponding to small-to-medium effect sizes (Cohen’s d) [55] of 0.21, 0.38, 0.45, and 0.73 for Factor 1, 2, 3, and Total scores respectively. Changes reached statistical significance (p < 0.001) for Factor 2, 3, and Total scores but not Factor 1 (p = 0.053).
Multiple linear regression analyses with post-course SEPCQ scores as dependent variables and CRMTL or CRSE as predictors, while adjusting for pre-course SEPCQ-scores, showed that pre-course CRMTL was a statistical significant predictor of post-course SEPCQ-scores for Factor 1 (Beta:0.21; p = 0.02); Factor 2 (Beta:0.21; p = 0.02), and SEPCQ Total scores (Beta:0.25; p = 0.005). A near-significant trend was found for Factor 3 (Beta:0.16; p = 0.052). None of the results for CRSE reached statistical significance (Beta: 0.07–0.18; p:0.06–0.40).
Adjustments
Although the Principal Component and DIF analyses indicated that item 25 might be problematic, the item was retained as the values (factor loading difference, the ETS, and K-index) only slightly exceeded the criteria, and the content appeared to reflect an important issue related to patient-communication-related challenges. The major concern was that for several items, primarily in factor 1 and 2, only very few responders chose the lowest scoring categories (0–2). The low item difficulties were hypothesized to be due to a) the high number of response categories and b) the mid-point anchor of 3 = “neither/nor”, which risked being interpreted as “indifference”. The response format was therefore changed to a 5-point Likert scale (0–4) with no mid-point anchor and endpoints anchored as “To a very low degree” and “To a very high degree”.
Step 6
The results obtained for the revised SEPCQ-27 when administered to Sample 3 and 4 are shown in Table 2. Both subscale and total scores now appeared normally distributed with similar means and medians (Means: 19.7, 15.4, 7.5, 42.7; Medians: 19, 16, 7, 43) and low skewness (−0.09, −0.12, 0.51, 0.12) and kurtosis (−0.16, 0.016, 0.41, 0.34) for the combined Sample 3 and 4. Internal consistencies, between-subscale correlations, and correlations between subscales and SEPCQ-27 total scores were generally similar to those found for Sample 2A (Tables 3 and 4). Small, but statistically significant, positive correlations were found with age. In Sample 3 and 4, women scored slightly higher than men on Factor 1 (mean difference = 2.0; p < 0.02) and SEPCQ-27 Total (3.0; p < 0.05). No gender differences were found for Factor 2 and 3. When exploring the possibility of response bias with the MCSD-12, small, but significant, positive correlations with social desirability were found for Factor 1, 3, and total SEPCQ scores (Table 4).
Confirmatory Factor Analysis (CFA)
When conducting a CFA with the SEPCQ-27 data from the independent sample of SDU students, the results for the chosen fit indices were: S-B Chi Square (441.2; p < 0.001); CFI = 0.98 (criterion > 0.95); NNFI = 0.98 (criterion > 0.95); RMSEA = 0.05 (90 % CI: 0.04 – 0.06) (criterion: < 0.06), and SRMR = 0.07 (criterion: 0.08). As a significant S-B Chi Square was expected, and the remaining 4 indices indicated good fit [53], no attempts were made to explore the fit of alternative models.
Step 7
A convenience sample of 101 physicians (response rate: 44 %) (Sample 5) also completed the SEPCQ-27. Gender, age, years of experience, and mean SEPCQ-27 scores are shown in Table 2. Internal consistencies were acceptable (0.84 – 0.95) (Table 3) and correlations between subscales and between subscales and SEPCQ-27 total scores were generally similar to those found for medical students (Table 4). Scores on Factor 2, 3, and total SEPCQ-27 - but not Factor 1 - showed statistical significant correlations with both age and years of experience. Years of experience correlated with age (r = 0.90), but when adjusting for years of experience, the correlations between SEPCQ scores and age (−0.09 to 0.09) no longer reached statistical significance. In contrast, when adjusting for age, all correlations with years of experience remained positive and reached statistical significance for SEPCQ-27 total scores (Table 4). Physicians exhibited statistically significantly higher scores than medical students on all SEPCQ scores (p < 0.001) (data not shown), and physicians who had participated in the DMA communication course had statistically significant higher scores on Factor 1, 2, and SEPCQ total (Cohen’s d: 0.55, 0.45, 0.48; p: 0.007, 0.03, 0.02), but not Factor 3 (d = 0.19; p = 0.30). No gender differences were found (data not shown).
Discussion
After having defined the concepts and possible categories of patient-centeredness self-efficacy, having developed an initial item pool, and evaluated items and instructions on the basis of established quality criteria, the first 88-item and the revised 27-item version of the SEPCQ was completed by a total of 749 medical students from two medical schools and 101 physicians from two university hospitals. The SEPCQ was evaluated in several stages involving several of the commonly recommended analytical approaches [56], and the results indicated sound psychometric properties.
Factor structure
Exploring the possible underlying factor structure, we identified three preliminary factors consisting of a total of 27 items: 1) Exploring the patient perspective, 2) Sharing information and power, and 3) Dealing with communicative challenges. From both a statistical and a content-based perspective, the three factors appeared to be valid subscales covering core aspects of patient-centeredness self-efficacy. The initially defined domain of “viewing the patient’s problem from a bio-psycho-social context” was the only domain, which was only sparsely covered (1 item in Factor 2). Using data from an independent sample, the identified 3-factor model was supported by the confirmatory factor analysis (CFA) showing good fit for the included commonly recommended fit indices. Furthermore, the internal consistencies were generally high across different samples of students and physicians. The main adjustment made to the final SEPCQ-27 was changing the original 7-point Likert scale format with the mid-point of “neither/nor”, which seemed to result in low item difficulties and somewhat positively skewed distributions of Factor 1 and 2, to a 5-point Likert scale. This adjustment appeared to solve this issue and resulted in normally distributed factor scores in subsequent samples.
Measurement and response bias
Differential item function (DIF) [47] for an item could indicate measurement bias, i.e., that individuals from different groups with the same underlying ability (latent trait) differ in their likelihood to respond in a certain way to the item. Studies suggest that female physicians engage in more patient-centered communication than male physicians [57], and as it would be important to know whether such differences stem from measurement bias or true gender differences in patient-centeredness self-efficacy, we therefore chose to evaluate possible gender-related measurement bias. Using two different approaches, there seemed to be no signs of DIF for items in Factor 1 and 2. Only two items from Factor 3 showed some indications of DIF with item 25 favoring men (“I am confident that I am able to stay focused on what is best for the patient if there is a professional disagreement about the diagnosis and treatment”) and item 26 favoring women (“I am confident that I am able to avoid letting myself be influenced by preconceptions about the patient”). However, as the content of both items appeared to be of importance to patient-centeredness self-efficacy and the values only just exceeded the criteria for DIF, we retained the two items in Factor 3. Response bias is the tendency to respond in an anticipated (socially desirable) manner to certain items [58]. Although our results suggested some degree of social desirability for Factor 1 and 3, but not for Factor 2, it is not clear to which degree this reflects the susceptibility of items to self-deception or impression management among the respondents [59]. The risk of response bias applies to many types of questionnaires, and that some of the attitudes and beliefs concerning patient-centeredness may be somewhat susceptible to social desirability, does not necessarily challenge the validity of the instrument.
Construct validity
To provide preliminary evidence for the validity of the SEPCQ, we had, prior to the data collection, stated several hypotheses concerning associations between SEPCQ scores and a number of background variables and additional measures.
Our results generally supported the hypothesized positive associations between SEPCQ scores and age and experience. Older students and physicians had higher scores and years of experience were, independently of age, associated with higher patient-centeredness self-efficacy. The association with age and experience was weakest for Factor 1 (Exploring the patient perspective) and strongest for Factor 3 (Dealing with communicative challenges), suggesting that insight and confidence in dealing with the emotional challenges and conflicts (e.g., item 23 and 24) and disagreement with colleagues (item 25) requires more experience than does confidence in the ability to establish a constructive relationship with the patient (e.g., item 2).
Female medical students have been found to value patient-orientation and communication more than male students [60] and, based on previous studies of physicians [57], we therefore expected that women would score higher than men. Our data, however, did not support any robust association with gender. The lack of an association may reflect a true finding, rather than lack of gender sensitivity of the instrument, as supported by a more recent meta-analysis [61] failing to show clear gender differences in communicative style.
As stress and burnout in residents has been associated with reduced empathy and lower reported patient-centeredness [25], we expected lower levels of medical student well-being, i.e., symptoms of distress and burnout, to be associated with lower SEPCQ scores. This was confirmed by the inverse correlations found between medical student well-being and SEPCQ scores. Well-being scores did, however, not predict pre-post course changes in SEPCQ scores, and the associations between well-being and patient-centeredness are likely to be complex and bi-directional [26].
Self-regulated learning theory predicts that motivational factors such as intrinsic motivation and self-efficacy for learning are important predictors of learning outcomes [62]. Based on previous findings [63–65], we therefore expected that the students’ motivation to learn (CRMTL) and their pre-course self-efficacy (CRSE) with respect to their ability to learn the skills taught in a course in peer-supervision and communication would predict the learning outcome, i.e. changes in their scores on the SEPCQ. In accordance with our hypotheses, level of motivation to learn the skills taught in the course was a significant, independent predictor of SEPCQ change-scores after the course. This suggests the importance of intrinsic motivation for learning patient-centeredness-related skills and, indirectly, provides further support for the construct validity of the SEPCQ.
Finally, the responsiveness of the SEPCQ was supported by increased scores from before to after completing the course in peer supervision and communication. As the effects of the course were not evaluated in a controlled trial, we cannot be certain to which degree the changes are directly related to participating in the course. However, this interpretation finds support in the results showing that physicians who previously had participated in a standard course in communication had higher SEPCQ scores than physicians who had not.
Conclusions
Taken together, our results indicate that the SEPCQ-27 is a reliable and valid instrument for assessing patient-centeredness self-efficacy in both medical students and physicians. The SEPCQ-27 could be a useful instrument for evaluating patient-centeredness self-efficacy in various contexts, e.g., when evaluating outcomes of communication training courses for medical students and physicians and when studying associations with physician well-being and job-satisfaction. The predictive validity of the SEPCQ remains to be evaluated in future research, e.g., in prospective studies of whether patient-centeredness self-efficacy can predict actual medical student or physician communicative behaviors and patient outcomes such as satisfaction and mental and physical health outcomes.
Acknowledgements
The authors wish to thank professor, MD, Hans von der Maase, for assisting with the acquisition of data from the Department of Oncology, Copenhagen University Hospital and all medical students and hospital physicians who participated in the study.
Abbreviations
- CDR
Combined Decision Rule
- CFA
Confirmatory Factor Analysis
- CFI
Comparative Fit Index
- CRMTL
Course-Related Motivation to Learn Questionnaire
- CRSE
Course-Related Self-Efficacy Questionnaire
- DIF
Differential Item Function
- DMA
Danish Medical Association
- ETS
Educational Testing Service
- IRT
Item-Response Theory
- KR-20
Kuder-Richardson Formula 20
- MCSDS
Marlowe Crowne Social Desirability Scale
- MH
Mantel-Haenszel
- MOT
Medical Outcomes Trust
- MSLQ
Motivated Strategies for Learning Questionnaire
- MSWBI
Medical Student Well-Being Index
- NNFI
Non-Normed Fit Index
- SEPCQ
The Patient-Centeredness Self-Efficacy Questionnaire
- QAS
Question Appraisal System
- RMSEA
Root Mean Square Error of Approximation
- S-B-Chi Square
Satorra-Bentler Scaled Chi-Square
- SRMR
Standardized Root Mean Square Residual
Footnotes
Competing interests
The author(s) declare that they have no competing interests.
Authors’ contributions
RZ conceived of the study, participated in the design and coordination of the study, construction of the initial item pool and categorizing of items, qualitative evaluation of the first 88-item version of the SEPCQ, administered the SEPCQ-27 to hospital physicians, conducted data-analyses, and drafted the manuscript. MOC participated in the design and coordination of the study, construction of the initial item pool and categorizing of items, qualitative evaluation of the first 88-item version of the SEPCQ, and administered the SEPCQ to student samples 1, 2, and 3. BL participated in the design and coordination of the study, construction of the initial item pool and categorizing of items, qualitative evaluation of the first 88-item version of the SEPCQ. LBK contributed to the design of the study, construction of the initial item pool and categorizing of items, qualitative evaluation of the first 88-item version of the SEPCQ. MO contributed with CFA analyses. MT participated in the coordination of the study and administered the SEPCQ to student sample 4. AMM participated in the design of the study, construction of the initial item pool and categorizing of items, and qualitative evaluation of the first 88-item version of the SEPCQ. All authors read and approved the final manuscript.
Contributor Information
Robert Zachariae, Email: bzach@aarhus.rm.dk.
Maja O’Connor, Email: maja@psy.au.dk.
Berit Lassesen, Email: belas@au.dk.
Martin Olesen, Email: psykmh@gmail.com.
Louise Binow Kjær, Email: louise@cesu.au.dk.
Marianne Thygesen, Email: mthygesen@health.sdu.dk.
Anne Mette Mørcke, Email: amm@cesu.au.dk.
References
- 1.Brunett PH, Campbell TL, Cole-Kelly K, Danoff D, Frymier R, Goldstein MG, Gordon GH, Klass DJ, Kurtz S, Laidlaw J, Lang F, MacLellan AM, Makoul G, Miller S, Novack D, Rider EA, Simon FA, Sluyter D, Swing S, Weston W, Whelan GP. Essential elements of communication in medical encounters: the Kalamazoo consensus statement. Acad Med. 2001;76:390–393. doi: 10.1097/00001888-200104000-00021. [DOI] [PubMed] [Google Scholar]
- 2.Committee on Quality of Health Care in America IoM . Crossing the quality chasm: A new health system for the 21st century. Washington D.C: National Academy Press; 2001. [Google Scholar]
- 3.Hopkins J, Healthways A. Consensus report - defining the patient-physician relationship for the 21st century. Dis Manag. 2004;7:161–179. doi: 10.1089/1093507042264827. [DOI] [PubMed] [Google Scholar]
- 4.Epstein RM, Street RL. Patient-centered communication in cancer care - Promoting healing and reducing suffering. Bethesda, MD: National Cancer Institute;NIH Pub lication No. 07–6225; 2007. [Google Scholar]
- 5.Epstein RM, Franks P, Fiscella K, Shields CG, Meldrum SC, Kravitz RL, Duberstein PR. Measuring patient-centered communication in patient-physician consultations: theoretical and practical issues. Soc Sci Med. 2005;61:1516–1528. doi: 10.1016/j.socscimed.2005.02.001. [DOI] [PubMed] [Google Scholar]
- 6.Stewart M, Brown JB, Weston WW, McWhinney IR, McWilliam CL, Freeman TR. Patient-centered medicine - Transforming the clinical method. 2. Abingdon, UK: Radcliffe Medical Press; 2003. [Google Scholar]
- 7.McCormack LA, Treiman K, Rupert D, Williams-Piehota P, Nadler E, Arora NK, Lawrence W, Street RL., Jr Measuring patient-centered communication in cancer care: a literature review and the development of a systematic approach. Soc Sci Med. 2011;72:1085–1095. doi: 10.1016/j.socscimed.2011.01.020. [DOI] [PubMed] [Google Scholar]
- 8.Stewart MA. Effective physician-patient communication and health outcomes - a review. Can Med Assoc J. 1995;152:1423–1433. [PMC free article] [PubMed] [Google Scholar]
- 9.Beck RS, Daughtridge R, Sloane PD. Physician-patient communication in the primary care office: a systematic review. J Am Board Fam Pract. 2002;15:25–38. [PubMed] [Google Scholar]
- 10.Arora NK. Interacting with cancer patients: the significance of physicians' communication behavior. Soc Sci Med. 2003;57:791–806. doi: 10.1016/S0277-9536(02)00449-5. [DOI] [PubMed] [Google Scholar]
- 11.Michie S, Miles J, Weinman J. Patient-centredness in chronic illness: what is it and does it matter? Patient Educ Couns. 2003;51:197–206. doi: 10.1016/S0738-3991(02)00194-5. [DOI] [PubMed] [Google Scholar]
- 12.Levinson W, Hudak P, Tricco AC. A systematic review of surgeon-patient communication: strengths and opportunities for improvement. Patient Educ Couns. 2013;93:3–17. doi: 10.1016/j.pec.2013.03.023. [DOI] [PubMed] [Google Scholar]
- 13.Griffin SJ, Kinmonth AL, Veltman MW, Gillard S, Grant J, Stewart M. Effect on health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trials. Ann Fam Med. 2004;2:595–608. doi: 10.1370/afm.142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Venetis MK, Robinson JD, Turkiewicz KL, Allen M. An evidence base for patient-centered cancer care: a meta-analysis of studies of observed communication between cancer specialists and their patients. Patient Educ Couns. 2009;77:379–383. doi: 10.1016/j.pec.2009.09.015. [DOI] [PubMed] [Google Scholar]
- 15.Henry SG, Fuhrel-Forbis A, Rogers MA, Eggly S. Association between nonverbal communication during clinical interactions and outcomes: a systematic review and meta-analysis. Patient Educ Couns. 2012;86:297–315. doi: 10.1016/j.pec.2011.07.006. [DOI] [PubMed] [Google Scholar]
- 16.Oliveira VC, Refshauge KM, Ferreira ML, Pinto RZ, Beckenkamp PR, Negrao Filho RF, Ferreira PH. Communication that values patient autonomy is associated with satisfaction with care: a systematic review. J Physiother. 2012;58:215–229. doi: 10.1016/S1836-9553(12)70123-6. [DOI] [PubMed] [Google Scholar]
- 17.Pinto RZ, Ferreira ML, Oliveira VC, Franco MR, Adams R, Maher CG, Ferreira PH. Patient-centred communication is associated with positive therapeutic alliance: a systematic review. J Geophys Res. 2012;58:77–87. doi: 10.1016/S1836-9553(12)70087-5. [DOI] [PubMed] [Google Scholar]
- 18.Stiefel F, Favre N, Despland JN. Communication skills training in oncology: it works! Recent Results Cancer Res. 2006;168:113–119. doi: 10.1007/3-540-30758-3_11. [DOI] [PubMed] [Google Scholar]
- 19.Dwamena F, Holmes-Rovner M, Gaulden CM, Jorgenson S, Sadigh G, Sikorskii A, Lewin S, Smith RC, Coffey J, Olomu A. Interventions for providers to promote a patient-centred approach in clinical consultations. Cochrane Database Syst Rev. 2012;12 doi: 10.1002/14651858.CD003267.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Uitterhoeve RJ, Bensing JM, Grol RP, Demulder PH, Van Achterberg T. The effect of communication skills training on patient outcomes in cancer care: a systematic review of the literature. Eur J Cancer Care (Engl) 2010;19:442–457. doi: 10.1111/j.1365-2354.2009.01082.x. [DOI] [PubMed] [Google Scholar]
- 21.Barth J, Lannen P. Efficacy of communication skills training courses in oncology: a systematic review and meta-analysis. Ann Oncol. 2011;22:1030–1040. doi: 10.1093/annonc/mdq441. [DOI] [PubMed] [Google Scholar]
- 22.Moore PM, Rivera MS, Grez AM, Lawrie TA. Communication skills training for healthcare professionals working with people who have cancer. Cochrane Database Syst Rev. 2013;3 doi: 10.1002/14651858.CD003751.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Smith S, Hanson JL, Tewksbury LR, Christy C, Talib NJ, Harris MA, Beck GL, Wolf FM. Teaching patient communication skills to medical students: a review of randomized controlled trials. Eval Health Prof. 2007;30:3–21. doi: 10.1177/0163278706297333. [DOI] [PubMed] [Google Scholar]
- 24.Ratanawongsa N, Roter D, Beach MC, Laird SL, Larson SM, Carson KA, Cooper LA. Physician burnout and patient-physician communication during primary care encounters. J Gen Intern Med. 2008;23:1581–1588. doi: 10.1007/s11606-008-0702-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Passalacqua SA, Segrin C. The effect of resident physician stress, burnout, and empathy on patient-centered communication during the long-call shift. Health Commun. 2012;27:449–456. doi: 10.1080/10410236.2011.606527. [DOI] [PubMed] [Google Scholar]
- 26.Krasner MS, Epstein RM, Beckman H, Suchman AL, Chapman B, Mooney CJ, Quill TE. Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA. 2009;302:1284–1293. doi: 10.1001/jama.2009.1384. [DOI] [PubMed] [Google Scholar]
- 27.Shanafelt TD. Enhancing meaning in work: a prescription for preventing physician burnout and promoting patient-centered care. JAMA. 2009;302:1338–1340. doi: 10.1001/jama.2009.1385. [DOI] [PubMed] [Google Scholar]
- 28.Ong LM, de Haes JC, Hoos AM, Lammes FB. Doctor-patient communication: a review of the literature. Soc Sci Med. 1995;40:903–918. doi: 10.1016/0277-9536(94)00155-M. [DOI] [PubMed] [Google Scholar]
- 29.Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84:191–215. doi: 10.1037/0033-295X.84.2.191. [DOI] [PubMed] [Google Scholar]
- 30.Bandura A. Self-efficacy - The exercise of control. New York: Freeman and Company; 1997. [Google Scholar]
- 31.Maguire P, Booth K, Elliott C, Jones B. Helping health professionals involved in cancer care acquire key interviewing skills--the impact of workshops. Eur J Cancer. 1996;32A:1486–1489. doi: 10.1016/0959-8049(96)00059-7. [DOI] [PubMed] [Google Scholar]
- 32.Parle M, Maguire P, Heaven C. The development of a training model to improve health professionals' skills, self-efficacy and outcome expectancies when communicating with cancer patients. Soc Sci Med. 1997;44:231–240. doi: 10.1016/S0277-9536(96)00148-7. [DOI] [PubMed] [Google Scholar]
- 33.Baile WF, Kudelka AP, Beale EA, Glober GA, Myers EG, Greisinger AJ, Bast RC, Jr, Goldstein MG, Novack D, Lenzi R. Communication skills training in oncology. Description and preliminary outcomes of workshops on breaking bad news and managing patient reactions to illness. Cancer. 1999;86:887–897. doi: 10.1002/(SICI)1097-0142(19990901)86:5<887::AID-CNCR27>3.0.CO;2-X. [DOI] [PubMed] [Google Scholar]
- 34.Pololi LH, Potter S. Behavioral change in preventive medicine. An efficacy assessment of a physician education module. J Gen Intern Med. 1996;11:545–547. doi: 10.1007/BF02599603. [DOI] [PubMed] [Google Scholar]
- 35.Stensrud TL, Mjaaland TA, Finset A. Communication and mental health in general practice: physicians' self-perceived learning needs and self-efficacy. Ment Health Fam Med. 2012;9:201–209. [PMC free article] [PubMed] [Google Scholar]
- 36.Scientific Advisory Committee of the Medical Outcomes Trust Assessing health status and quality-of-life instruments: attributes and review criteria. Qual Life Res. 2002;11:193–205. doi: 10.1023/A:1015291021312. [DOI] [PubMed] [Google Scholar]
- 37.Little P, Everitt H, Williamson I, Warner G, Moore M, Gould C, Ferrier K, Payne S. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323:908–911. doi: 10.1136/bmj.323.7318.908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Flocke SA, Stange KC, Zyzanski SJ. The association of attributes of primary care with the delivery of clinical preventive services. Med Care. 1998;36:AS21–AS30. doi: 10.1097/00005650-199808001-00004. [DOI] [PubMed] [Google Scholar]
- 39.Safran DG, Kosinski M, Tarlov AR, Rogers WH, Taira DH, Lieberman N, Ware JE. The primary care assessment survey: tests of data quality and measurement performance. Med Care. 1998;36:728–739. doi: 10.1097/00005650-199805000-00012. [DOI] [PubMed] [Google Scholar]
- 40.Galassi JP, Schanberg R, Ware WB. The Pra - a brief measure of perceived quality of the patient-provider medical relationship. Int J Psychol. 1992;27:639. [Google Scholar]
- 41.Lerman CE, Brody DS, Caputo GC, Smith DG, Lazaro CG, Wolfson HG. Patients' perceived involvement in care scale: relationship to attitudes about illness and medical care. J Gen Intern Med. 1990;5:29–33. doi: 10.1007/BF02602306. [DOI] [PubMed] [Google Scholar]
- 42.Willis GB, Lessler JT. Question Appraisal System - QAS-99. 1999. [Google Scholar]
- 43.Dyrbye LN, Szydlo DW, Downing SM, Sloan JA, Shanafelt TD. Development and preliminary psychometric properties of a well-being index for medical students. BMC Med Educ. 2010;10:8. doi: 10.1186/1472-6920-10-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Pintrich PR. Special issue - current issues and New directions in motivational theory and research - comment. Educ Psychol. 1991;26:199–205.
- 45.Crowne DP, Marlowe D: A new scale of social desirability independent of psychopathology. J Consult Psychol 1960;24:349-354. [DOI] [PubMed]
- 46.Tabachnick BG, Fidell LS. Using multivariate statistics. 4. Needham Heights, MA: Allyn & Bacon; 2007. [Google Scholar]
- 47.Camilli G, Shepard LA. Methods for identifying biased test items. Thousand Oaks, CA: Sage Publications; 1994. [Google Scholar]
- 48.Penfield RD. DIFAS: Differential Item Functioning Analysis System. Appl Psychol Meas. 2005;29:150–151. doi: 10.1177/0146621603260686. [DOI] [Google Scholar]
- 49.Thissen D, Steinberg L, Wainer H. Detection of differential item functioning using the parameters of item response models. In: Holland P, Wainer H, editors. Differential item functioning. Hillsdale,NJ: Lawrence Erlbaum; 1993. pp. 67–113. [Google Scholar]
- 50.Edelen MO, Reeve BB. Applying item response theory (IRT) modeling to questionnaire development, evaluation, and refinement. Qual Life Res. 2007;16(Suppl 1):5–18. doi: 10.1007/s11136-007-9198-0. [DOI] [PubMed] [Google Scholar]
- 51.Zieky M. Practical questions in the use of DIF statistics in test development. In: Holland P, Wainer H, editors. Differential item functioning. Hillsdale, NJ: Erlbaum; 1993. pp. 337–348. [Google Scholar]
- 52.Kumagai R. A new method for estimating differential item functioning (DIF) for multiple groups and polytomous items: Development of index K and the computer program "EasyDIF". Japanese J Psychol. 2012;83:35–43. doi: 10.4992/jjpsy.83.35. [DOI] [PubMed] [Google Scholar]
- 53.Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6:1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- 54.Marsh HW, Hau K-T, Wen Z. In search of golden rules: comments on hypothesis testing approaches to setting cutoff values for fit indexes and danghers in overgeneralising Hu & bentler (1999) Struct Equ Model. 2004;11:320–341. doi: 10.1207/s15328007sem1103_2. [DOI] [Google Scholar]
- 55.Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale, N.J.: Lawrence Erlbaum Associates; 1988. [Google Scholar]
- 56.Rust J, Golombok S. Modern psychometrics: the science of psychological assessment. 3. New York: Taylor & Francis; 2009. [Google Scholar]
- 57.Roter DL, Hall JA. Physician gender and patient-centered communication: a critical review of empirical research. Annu Rev Public Health. 2004;25:497–519. doi: 10.1146/annurev.publhealth.25.101802.123134. [DOI] [PubMed] [Google Scholar]
- 58.Crowne D, Marlowe D. The approval motive - studies in evaluative dependence. New York: John Wiley & Sons; 1964. [Google Scholar]
- 59.Paulhus DL. Two-component models of socially desirable responding. J Pers Soc Psychol. 1984;46:598–609. doi: 10.1037/0022-3514.46.3.598. [DOI] [Google Scholar]
- 60.Kruschinski C, Wiese B, Hummers-Pradier E. Attitudes towards general practice: a comparative cross-sectional survey of 1st and 5th year medical students. GMS Z Med Ausbild. 2012;29:Doc71. doi: 10.3205/zma000841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Jefferson L, Bloor K, Birks Y, Hewitt C, Bland M. Effect of physicians' gender on communication and consultation length: a systematic review and meta-analysis. J Health Serv Res Policy. 2013;18:242–248. doi: 10.1177/1355819613486465. [DOI] [PubMed] [Google Scholar]
- 62.van Dinther M, Dochy F, Segers M. Factors affecting students' self-efficacy in higher education. Educ Res Rev. 2011;6:95–108. doi: 10.1016/j.edurev.2010.10.003. [DOI] [Google Scholar]
- 63.Stegers-Jager KM, Cohen-Schotanus J, Themmen AP. Motivation, learning strategies, participation and medical school performance. Med Educ. 2012;46:678–688. doi: 10.1111/j.1365-2923.2012.04284.x. [DOI] [PubMed] [Google Scholar]
- 64.Turan S, Konan A. Self-regulated learning strategies used in surgical clerkship and the relationship with clinical achievement. J Surg Educ. 2012;69:218–225. doi: 10.1016/j.jsurg.2011.09.003. [DOI] [PubMed] [Google Scholar]
- 65.Cook DA, Thompson WG, Thomas KG. The motivated strategies for learning questionnaire: score validity among medicine residents. Med Educ. 2011;45:1230–1240. doi: 10.1111/j.1365-2923.2011.04077.x. [DOI] [PubMed] [Google Scholar]