

Highlights
-
•
We report a false aneurysm of the deep femoral artery after uneventful stabilization of a hip fracture.
-
•
Plain X-ray showed displaced lesser trochanter in close proximity to the deep femoral artery as this was calcified.
-
•
CT scan confirmed an arterial lesion due to displaced lesser trochanter.
-
•
The bony spike was removed surgically and the deep femoral artery was repaired using a vein patch.
Keywords: Lesser trochanter, Arterial injury, Deep femoral artery, Pseudoaneurysm, Hip fracture
Abstract
Introduction
Vascular complications after hip fracture are rare but can be life-threatening, especially in the elderly and if diagnosed late.
Presentation of the case
We report a false aneurysm of the calcified deep femoral artery after hip fracture and uneventful stabilization with a gamma nail, in an 85 year old woman. Three weeks after surgery there was swelling of the proximal thigh. Ultrasound scan revealed a false aneurysm of the deep femoral artery and plain X-ray showed a lesser trochanter fragment spiking the calcified deep femoral artery. Open repair of the pseudo-aneurysm with a vein patch was performed.
Discussion
Nowadays the preferred imaging of false aneurysms is by computed tomographic (CT) angiography but this involves high radiation and nephrotoxic contrast agents and may delay diagnosis. What made this a special case was the post-operative plain X-ray which showed a displaced fragment of the lesser trochanter spiking the calcified deep femoral artery, as confirmed on CT scanning.
Conclusion
Surgeons should pay attention to any displaced bone fragments close to calcified vessels, especially in the evaluation of routine x-rays following surgical treatment of fractures. This could minimize the potential life-threatening risk of delayed diagnosis, especially because it represents a routine image following surgical fracture treatments.
1. Introduction
Pertrochanteric fractures happens frequently in the elderly. In a quarter of cases fractures are unstable with a displaced lesser trochanter [1]. The dynamic hip screw system as well as the intramedullar gamma nail is the preffered method of stabilization [2]. The complication rate of vascular injuries after hip fracture is rare between 0.2 and 0.3% [3] and was first described in the year 1964 [4]. In most of the cases vascular damage resulted from screws, cement spiculae or Hohmann retractors [5].
In the case presented even plain X-ray reveals the direct trauma of calcified deep femoral artery by the displaced lesser trochanter after hip fracture.
2. Presentation of the case
A 85-year-old female with left-sided pertrochanteric unstable femur fracture underwent a gamma nail fixation. Three weeks after surgery a large swelling in the left groin occurred requiring a referral to the department of vascular surgery.
Clinical examination showed a pulsating mass in the left groin. She was hemodynamically stable and hemoglobin level was 10.2 g/dl. Ultrasound scan revealed a false aneurysm of the deep femoral artery with a maximum diameter of 5 cm and a total length of 8 cm. The pseudoaneurysmal neck was not identified. Due to elevated creatinine levels no further invasive vascular imaging was initiated.
Interestingly, however, X-ray image indicated a displaced fragment of the lesser trochanter in immediate vicinity of a calcified deep femoral artery (Fig. 1).
Fig. 1.
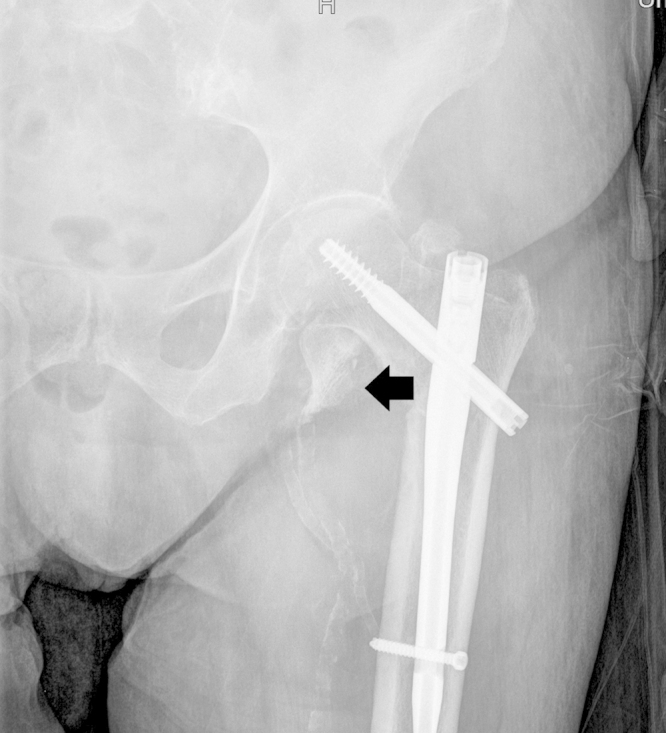
X-ray image of the hip ad admission. X-ray image showing displaced lesser trochanter and calcified femoral arteries. Arrow: tip end of the displaced lesser trochanter.
CT scan without contrast medium confirmed a large hematoma around the deep femoral artery (Fig. 2). Finally a direct spiking of the deep femoral artery by the fractured lesser trochanter was visible (Fig. 3).
Fig. 2.

CT scan of the hip. CT scan without contrast medium of the hip and proximal femur demonstrating calcified femoral artery and big surrounding hematoma. Arrow: hematoma around femoral artery.
Fig. 3.
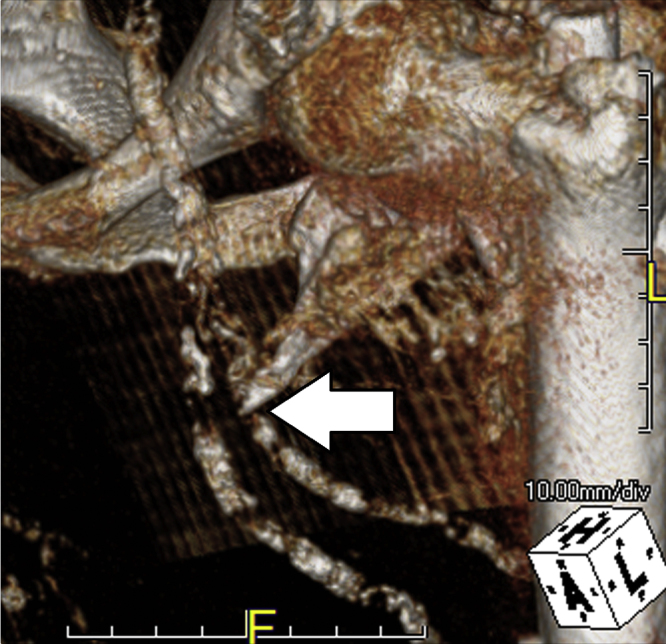
CT reconstruction of the proximal femur. 3D illustration of the hip with displaced lesser trochanter and tip end spiking the calcified femoral artery. Arrow: femoral artery spiking by tip end of lesser trochanter.
After longitudinal groin incision the tip of the lesser trochanter was removed and reconstruction of the vessel wall by using a vein patch was done (Fig. 4). Due to significant arterial wall calcification, vascular control was performed using intraluminal balloon catheters proximal and distal to the arteriotomy.
Fig. 4.
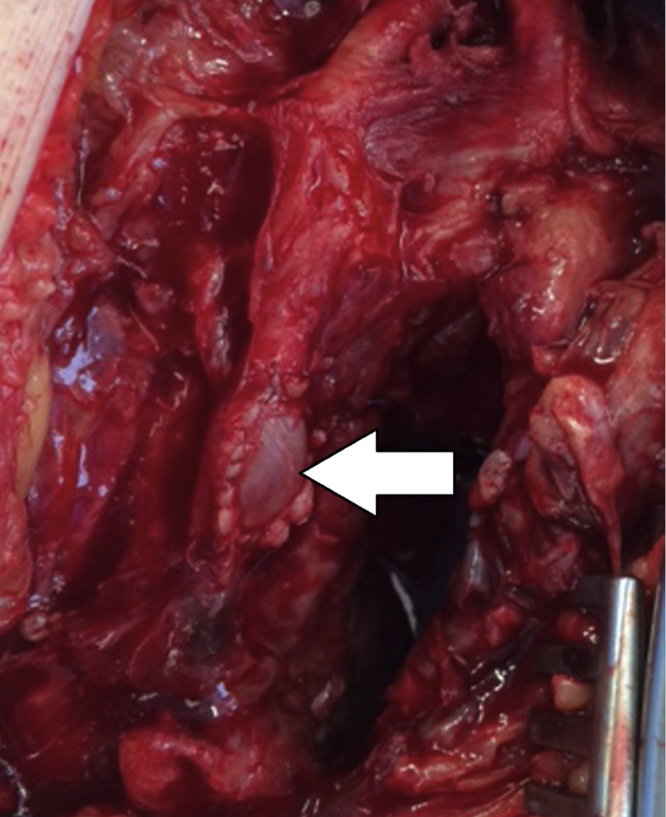
Reconstruction of the deep femoral artery. After resection of the lesser trochanter the deep femoral artery was reconstructed with a vein patch. Arrow: vein patch of the deep femoral artery.
The culture of the excised arterial wall and scrape of the hematoma showed no growth after two weeks. The histological examination confirmed advanced atherosclerotic changes in vessels wall and puncture lesions causing the pseudoaneurysm. There were no postoperative complications and the patient was discharged after 9 days.
3. Discussion
Fracture of the proximal femur is common among the elderly, the incidence increasing with age and degree of osteoporosis [6]. The incidence of atherosclerosis also increases, with resulting fragile vessels [7].
False aneurysm of femoral artery in a 72-years old man due to a dislocated bone fragment was first described by Abraham in the year 1975 [8]. Subsequently more cases of groin vessel injury due to hip fracture treatment have been reported, and in approximately 80% the deep femoral artery was affected [9]. This can be explained by the dorsolateral course of the deep femoral artery with its proximity to the proximal femur. The lesser trochanteric fragments move mediocranial due to the function of the attached iliopsoas and firstly crosses over the deep femoral artery.
In almost 25% of pertrochanteric fractures the lesser trochanter is involved [10]. Thus, it is surprising that the vascular complication rate is only between 0.2 and 0.3% [3]. A possible explanation for the infrequent vascular injury during hip fracture and following osteosynthetic treatment can be vessels elasticity. However, proximal femur fractures are common in elderly. These patients have also an increased risk for atherosclerosis [7].
False aneurysms are best diagnosed on arterial duplex or CT-angiogram, which is less invasive than conventional angiography [11]. Plain X-ray is only helpful if vessels are calcified.
The main focus of attention on the plain X-ray after orthopedic fracture stabilization is usually on the osteosynthesis equipment and bone fragments, though in the case presented calcification of the femoral arteries made them visible even in plain X-ray.
The time interval reported between hip fracture and clinical manifestation of false aneurysm has varied between 3 days and 14 years [12]. In cases of dislocated lesser trochanter being responsible for vascular lesion, the period from fracture to appearance of false aneurysm was between 18 and 36 days [13]. One possible explanation for the time lag can be movement of bone fragments, induced by mobilization after successful orthopedic surgery. In the case presented the period between gamma nail fixation and referral to department of vascular surgery was 4 weeks, corresponding to the average time interval as previously reported.
Therapeutic options in acute treatment of false aneurysms after trauma are interventional or surgical to stop bleeding. However, if the arterial lesion is induced by displacement of bone fragments or osteosythesis equipment, immediate surgical removal is necessary. Open repair of the artery can be done by a plain suture or by a more complex reconstruction with the use of vein or prosthetic graft.
In the case presented a bony spike of the displaced lesser trochanter was removed and perforation of deep femoral artery was repaired by vein patch.
4. Conclusion
A false aneurysm of the deep femoral artery after femur fracture and orthopedic surgery is rare, but can be life-threatening. It is sometimes difficult to diagnose, especially as a false aneurysm after hip trauma can take weeks, months or even years before becoming clinically apparent. This case is unique because calcification in the arterial wall provided “vascular imaging” on plain X-ray even without the use of contrast media. When assessing the X-ray, surgeons should pay attention not only to bone fragments but particularly to adjacent calcified vessels. Further imaging and appropriate intervention can reduce potential complications (which including death) from a fracture-induced traumatic pseudoaneurysm.
Conflict of interests
None declared.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this Journal.
Author contributions
All authors drafted and designed the manuscript and participated in surgery; All authors read and approved the final manuscript.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Guarantor
Susanne Regus.
References
- 1.Lindskog D.M., Baumgaertner M.R. Unstable intertrochanteric hip fractures in the elderly. J. Am. Acad. Orthop. Surg. 2004;12:179–190. doi: 10.5435/00124635-200405000-00006. [DOI] [PubMed] [Google Scholar]
- 2.Hesse B., Gachter A. Complications following the treatment of trochanteric fractures with the gamma nail. Arch. Orthop. Trauma Surg. 2004;124:692–698. doi: 10.1007/s00402-004-0744-8. [DOI] [PubMed] [Google Scholar]
- 3.Fruhwirth J., Koch G., Mischinger H.J., Werkgartner G., Tesch N.P. Vascular complications in minimally invasive surgery. Surg. Laparosc. Endosc. 1997;7:251–254. [PubMed] [Google Scholar]
- 4.Dameron T.B., Jr. False aneurysm of femoral profundus artery resulting from internal-fixation device (Screw) J. Bone Joint Surg. Am. Vol. 1964;46:577–580. [PubMed] [Google Scholar]
- 5.Nachbur B., Meyer R.P., Verkkala K., Zurcher R. The mechanisms of severe arterial injury in surgery of the hip joint. Clin. Orthop. Relat. Res. 1979:122–133. [PubMed] [Google Scholar]
- 6.Newman E.D., Ayoub W.T., Starkey R.H., Diehl J.M., Wood G.C. Osteoporosis disease management in a rural health care population: hip fracture reduction and reduced costs in postmenopausal women after 5 years. Osteoporos. Int. 2003;14:146–151. doi: 10.1007/s00198-002-1336-5. A journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. [DOI] [PubMed] [Google Scholar]
- 7.Benetos A., Waeber B., Izzo J. Influence of age, risk factors, and cardiovascular and renal disease on arterial stiffness: clinical applications. Am. J. Hypertens. 2002;15:1101–1108. doi: 10.1016/s0895-7061(02)03029-7. [DOI] [PubMed] [Google Scholar]
- 8.Abraham E., Pankovich A.M., Jansey F. False aneurysm of the profunda femoris artery resulting from intertrochanteric fracture. A case report. J. Bone Joint Surg. Am. Vol. 1975;57:871. [PubMed] [Google Scholar]
- 9.Whitehill R., Wang G.J., Edwards J.R., Stamp W.G. Late injuries to femoral vessels after fracture of the hip. Case report. J. Bone Joint Surg. Am. Vol. 1978;60:541–542. [PubMed] [Google Scholar]
- 10.Mauerhan D.R., Maurer R.C., Effeney D. Profunda femoris arterial laceration secondary to intertrochanteric hip fracture fragments: a case report. Clin. Orthop. Relat. Res. 1981:215–219. [PubMed] [Google Scholar]
- 11.Wixon C.L., Philpott J.M., Bogey W.M., Jr., Powell C.S. Duplex-directed thrombin injection as a method to treat femoral artery pseudoaneurysms. J. Am. Coll. Surg. 1998;187:464–466. doi: 10.1016/s1072-7515(98)00204-x. [DOI] [PubMed] [Google Scholar]
- 12.Molfetta L., Chiapale D., Caldo D., Leonardi F. False aneurysm of the superficial femoral artery after total hip arthroplasty: a case report. Hip Int.: J. Clin. Exp. Res. Hip Pathol. Ther. 2007;17:234–236. doi: 10.1177/112070000701700408. [DOI] [PubMed] [Google Scholar]
- 13.Lohmann H., Esenwein S., Geier B., Vogel T., Kleinert H. [False aneurysm of the deep femoral artery due to pertochanteric fracture of the hip with displaced fragment of the lesser trochanter] Zeitschrift fur Orthop. Unfallrchirurgie. 2009;147:23–25. doi: 10.1055/s-2008-1039115. [DOI] [PubMed] [Google Scholar]