

Highlights
-
•
PCNSL is increasing observed in immunocompetent patients with no known etiology or risk factors.
-
•
An isolated PCNSL in the fourth ventricle in an immunocompetent patient is reported.
-
•
PCNSL should be considered with homogenous lesions of the fourth ventricle.
-
•
Aggressive surgical resection in this surgically accessible location is rational.
Keywords: Lymphoma, Intraventricular tumor, CNS
Abstract
Introduction
Primary central nervous lymphoma(PCNSL) is a rare form of non-Hodgkin lymphoma confined to the central nervous system. Most of the lesions are supratentorial and periventricular, often involving deep structures such as corpus callosum and basal ganglion. Isolated intraventricular lymphoma is rare and only a few case reports. We report, to the best of our knowledge, the seventh case of isolated PCNSL in the fourth ventricle in an immunocompetent patient.
Presentation of case
A 61-year-old male presenting with 3 months of headache and dizziness followed with unsteady gait for days. The MR imaging of brain revealed a homogeneously enhancing lesion occupying almost the whole 4th ventricle.The tumor was removed subtotally via suboccipital craniotomy. Histopathology revealed the lesion be a diffuse large B-cell lymphoma.
Discussion
PCNSL is an important consideration in the differential diagnosis of intracranial mass lesion. The unusual location in surgically accessible fourth ventricle in posterior fossa, the isolation of the tumor may present a compelling indication for surgical resection.
Conclusion
We suggest that primary lymphoma should be considered with homogenous lesions of the 4th ventricle. Also aggressive surgical resection in this surgically accessible location, instead of biopsy only, is rational.
1. Introduction
Primary central nervous lymphoma (PCNSL) is a rare form of non-Hodgkin lymphoma accounting for 1–4% of all brain neoplasms [1–6]. It is usually associated with immunodeficiency(most commonly HIV) but is increasingly observed in immunocompetent patients with no known etiology or risk factors [4]. Therefore, it is an important consideration in the differential diagnosis of intracranial mass lesion. PCNSL almost always presents as a cerebral parenchyma lesion whereas secondary CNS lymphoma tends to present as leptomeningeal metastasis [7]. Isolated intraventricular lymphoma is rare. Herein, we report a case of primary isolated lymphoma of the fourth ventricle in an immunocompetent patient.
2. Presentation of case
A 61-year-old man presented with a 3-month history of headache, dizziness and progressively unsteady gait. He also had medical history of hypertension and diabetes mellitus under regular control.
On examination, he was found to have mild cerebellar ataxia. Magnetic resonance imaging (MRI) of his brain showed a homogeneously enhancing, well defined mass lesion occupying almost the entire fourth ventricle (Fig. 1). The mass lesion was homogeneously enhanced and lack of necrosis or hemorrhage. Neither cystic appearance nor calcifications was found. The radiologist’s impression was that of a lymphoma or ependymoma. Initial blood testing was unremarkable. An additional work-up with HIV testing and computed tomography (CT) scans of the neck, chest, abdomen, and pelvis showed negative results.
Fig. 1.
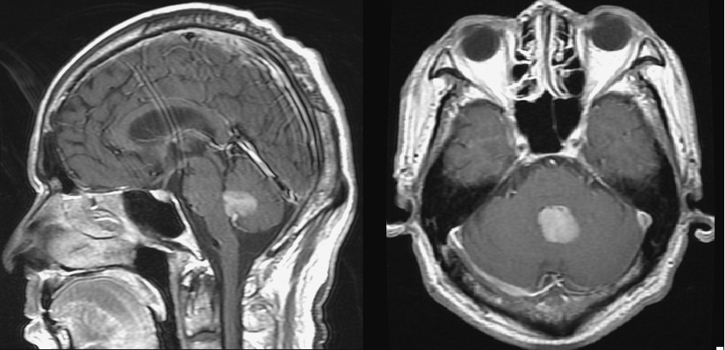
T1-weighted, gadolinium-enhanced sagittal magnetic resonance image (left) and axial MRI (right), showing a well-demarcated intensely enhancing lesion occupied almost the entire fourth ventricle.
We performed a suboccipital craniotomy and the tumor was accessed through a transvermian approach. The tumor was exophytic,grayish in color, soft and slightly vascularized. Clear tumor- brainstem interface but invasion of left vermis was noted intraoperatively. Complete resection of the intraventricular lesion was achieved. The frozen section showed tumor cells of unknown origin. The permanent section showed diffuse infiltration of a typical lymphocytes with irregular nuclei. Immunohistochemistry stains showed that the cells were positive for CD20 and CD10. The morphology and immunohistochemistry profile were consistent with a diffuse large B-cell lymphoma (Fig. 2).
Fig. 2.

The Hematoxylin-eosin stain revealed diffuse infiltration of atypical lymphocytes with irregular nuclei (a). Immunohistochemistry stains show the cells positive for CD20 (b) and CD10 (c).
The patient has a smooth postoperative course without neurological deficit and his headache and gait disturbance had markedly improved.
The patient was commenced on 6 cycles of chemotherapy with Rituximab and Methotrexate. The patient remains well at three months from diagnosis.
3. Discussion
PCNSL is a rare tumor, and only a few case reports have addressed PCNSL in fourth ventricule [2–6,8]. Since the brain is an immunologically privileged site which does not contain lymphatics or lymphoid tissue. The origin of such a primary tumor is unclear. Hochberg et al. [9] suggested that the clone of malignant systemic lymphocytes which displaying specific adhesion molecules and bind to the specific proteins only presented in the CNS might be pathogenesis. Significant risk factor is acquired or congenital immunodeficiency [6]. However, It has increased incidence in immunocompetent patients over the past few decades. This increase is independent of advances in neuroimaging or the general aging of the population [10]. Therefore, it is an important consideration in the differential diagnosis of intracranial mass lesions.
Despite the image diagnosis of PCNSL is challenging, there are several key imaging characteristics of CNS lymphoma. PCNSL typically shows intermediate to low signal intensity on T1-weighted images and a isointense or hyperintense signal on T2-weighted images. Contrast uptake is usually avid and homogenous. Because of its high cellularity, it tends to be hyperintense on a diffuse weighed image and hypointense on apparent diffusion coefficient images. MR spectroscopy may show a high choline-to-creatine ratio [11]. The diagnosis of lymphoma in our case serves to reinforce the previous reports-to include it in the differential diagnosis of an homogenously enhanced lesion in the fourth ventricle.
Given the good responsiveness of CNS lymphoma to chemoradiation, the PCNSL are considered non-surgical tumors and attempt to resection or decompression has been shown of no benefit due to its diffuse infiltration and often deep seated locations [12]. The surgical consensus is minimally invasive biopsy for tissue diagnosis. However, survival outcomes mentioned for PCNSL have been uniformly disappointing despite recent advanced and the often initial dramatic response to chemoradiation. Recent investigators are challenging this conservative surgical manner [13,14]. The German Primary CNS Lymphoma Study Group 1 (G-PCNSL-SG-1) found that the overall survival and progression-free-survival were significant shorter in the biopsied group compared with subtotal and total resection group [13]. There are also reports suggested that surgical debulking may provide not only significant clinical benefit but also elimination the cell populations with drug resistance potential. It is also correlated with better progression-free survival and overall survival [14]. In addition, the unusual location in surgically accessible fourth ventricle in posterior fossa, the isolation of the tumor may present a compelling indication for surgical resection [15]. It can provide the possibility for the patient to be shunt independent and also prevent from intraabdominal tumor seeding.
4. Conclusion
We suggest that PCNSL should be considered with homogenous lesions of the fourth ventricle. Also aggressive surgical resection in this surgically accessible location, instead of biopsy only, is rational.
Conflict of interest
None.
Funding
None.
Ethical approval
Not applicable.
Author contributions
HIH wrote the manuscript. HIH, SSH, PHL participated in the diagnosis and treatment of present case. HHT carried out pathological analysis. All authors approved the final manuscript.
Consent
We have obtained written consent from patient and can provide a copy if needed.
Contributor Information
Huang-I Hsu, Email: mccoyhsu@gmail.com.
Ping-Hong Lai, Email: phlai@vghks.gov.tw.
Hui-Hwa Tseng, Email: hhtseng@vghks.gov.tw.
Shu-Shong Hsu, Email: sshsu59@yahoo.com.
References
- 1.Rubenstein J., Ferreri A.J., Pittaluga S. Primary lymphoma of the central nervous system: epidemiology, pathology and current approaches to diagnosis, prognosis and treatment. Leuk. Lymphoma. 2008;49(Suppl. 1):43–51. doi: 10.1080/10428190802311441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Haegelen C., Riffaud L., Bernard M., Morandi X. Primary isolated lymphoma of the fourth ventricle: case report. J. Neurooncol. 2001;51:129–131. doi: 10.1023/a:1010790325692. http://www.ncbi.nlm.nih.gov/pubmed/11386409 [DOI] [PubMed] [Google Scholar]
- 3.Hill C.S., Khan A.F., Bloom S., McCartney S., Choi D. A rare case of vomiting: fourth ventricular B-cell lymphoma. J. Neurooncol. 2009;93:261–262. doi: 10.1007/s11060-008-9765-4. [DOI] [PubMed] [Google Scholar]
- 4.Bokhari R., Ghanem A., Alahwal M., Baeesa S. Primary isolated lymphoma of the fourth ventricle in an immunocompetent patient. Case Rep. Oncol. Med. 2013;2013:4. doi: 10.1155/2013/614658. Article ID 614658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Liao C.-H., Lin S.-C., Hung S.-C., Hsu S.P.C., Ho D.M.-T., Shih Y.-H. Primary large B-cell lymphoma of the fourth ventricle. J. Clin. Neurosci. 2014;21:180–183. doi: 10.1016/j.jocn.2013.02.036. [DOI] [PubMed] [Google Scholar]
- 6.Alabdulsalam A., Zaidi S.Z.A., Tailor I., Orz Y., Al-Dandan S. Primary burkitt lymphoma of the fourth ventricle in an immunocompetent young patient. Case Rep. Pathol. 2014;2014:6. doi: 10.1155/2014/630954. Article ID 630954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Erdag N., Bhorade R.M., Alberico R.A., Yousuf N., Patel M.R. Primary lymphoma of the central nervous system: typical and atypical CT and MR imaging appearances. Am. J. Roentgenol. 2001;176:1319–1326. doi: 10.2214/ajr.176.5.1761319. [DOI] [PubMed] [Google Scholar]
- 8.Werneck L.C., Hatsbach Z., Mora A.H., Novak E.M. Meningite por linfoma primitivo do sistema nervoso central. Arq. Neuro-Psiquiat. (São Paulo) 1977;35:366. doi: 10.1590/s0004-282x1977000400010. [DOI] [PubMed] [Google Scholar]
- 9.Hochberg F.H., Baehring J.M., Hochberg E.P. Primary CNS lymphoma. Nat. Clin. Pract. Neurol. 2007;3:24–35. doi: 10.1038/ncpneuro0395. [DOI] [PubMed] [Google Scholar]
- 10.Nakamura M., Shimada K., Ishida E., Konishi N. Histopathology, pathogenesis and molecular genetics in primary central nervous system lymphomas. Histol. Histopathol. 2004;19:211–219. doi: 10.14670/HH-19.211. [DOI] [PubMed] [Google Scholar]
- 11.Yap K.K., Sutherland T., Liew E., Tartaglia C.J., Pang M., Trost N. Magnetic resonance features of primary central nervous system lymphoma in the immunocompetent patient: a pictorial essay. J. Med. Imaging Radiat. Oncol. 2012;56:179–186. doi: 10.1111/j.1754-9485.2012.02345.x. [DOI] [PubMed] [Google Scholar]
- 12.Bataille B., Delwail V., Menet E., Vandermarcq P., Ingrand P., Wager M. Primary intracerebral malignant lymphoma: report of 248 cases. J. Neurosurg. 2000;92:261–266. doi: 10.3171/jns.2000.92.2.0261. [DOI] [PubMed] [Google Scholar]
- 13.Bierman P.J. Surgery for primary central nervous system lymphoma: is it time for reevaluation? Oncol. (Willist. Park NY) 2014;28:632–637. [PubMed] [Google Scholar]
- 14.Weller M., Martus P., Roth P., Thiel E., Korfel A. Surgery for primary CNS lymphoma? Challenging a paradigm. Neuro. Oncol. 2012;14:1481–1484. doi: 10.1093/neuonc/nos159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Brastianos P.K., Batchelor T.T. Primary central nervous system lymphoma: overview of current treatment strategies. Hematol. Oncol. Clin. North Am. 2012;26:897–916. doi: 10.1016/j.hoc.2012.05.003. [DOI] [PubMed] [Google Scholar]