

Highlights
-
•
The first case of isolated rupture of vastus intermedius tendon in the literature.
-
•
Partial quadriceps tendon rupture can be treated by conservative therapy.
Keywords: Quadriceps, Partial rupture, Extensor, Vastus intermedius
Abstract
Introduction
Quadriceps tendon injuries are rare. There is a limited number of studies in the literature, reporting partial quadriceps tendon ruptures. We did not find any study reporting an isolated vastus intermedius tendon injury in the literature.
Presentation of case
A 22 years old professional rugby player with the complaints of pain in the right lower limb, decreased range of motion in right knee and a mass in the mid-anterior of the right thigh applied following an overloading on his hyperflexed knee during a rugby match. T2 sequence magnetic resonance images revealed discontinuity in the vastus intermedius tendon and intramuscular hematoma. The patient has been conservatively treated.
Discussion
Quadriceps tendon ruptures generally occur after the 4th decade in the presence of degenerative changes. Our case is a young professional rugby player. Isolated vastus intermedius tendon rupture is unusual. Conservative treatment is performed as the intermedius tendon is in the deepest layer of the quadriceps muscle.
Conclusion
We report the first case of isolated rupture of the vastus intermedius tendon in the literature and we claim that disorder may be succesfully treated with conservative treatment and adequate physiotheraphy.
1. Introduction
It has been previously demonstrated that quadriceps tendon consisted of layers [1–3]. These trilaminar layers; the superficial rectus femoris tendon and muscle, the deeply located vastus intermedius muscle and tendon, and the muscles and tendons of the vastus medialis and vastus lateralis that flank the superficial and deep layers of the extensor mechanism [2]. Quadriceps tendon injuries are rare and generally occur after the 4th decade [4,5]. These are usually full thickness injuries. There is a limited number of studies in the literature, reporting partial quadriceps tendon ruptures [6–9]. Also we did not find any study reporting an isolated vastus intermedius tendon injury in the literature.
2. Presentation of case
A 22 years old professional rugby player applied with the complaints of pain in the right lower limb, decreased range of motion in right knee and a mass in the mid-anterior of the right thigh, that started after an overloading on his hyperflexed knee during a rugby match. The patient has consented for the case report. The patient claimed that he could not continue playing. There was no history of comobidity or medical treatment. Tenderness was present in the anterior of the suprapatellar region in the right thigh. Passive flexion of the right knee was measured as 100° and passive extension was full. Active knee extension was not present. The patient was unable to straight leg raise right leg. No osseous pathology was observed in plain radiographies (Fig. 1). T2 sequence magnetic resonance images revealed discontinuity in the vastus intermedius tendon and intramuscular hematoma (Fig. 2). A hinged knee brace was applied for 2 weeks. The patient was let controlled weight bearing as the brace was locked in full extension in the first week and 90° of flexion was let in the second week. In the 3rd and the 4th weeks, full flexion and full weight bearing were let. Then the brace was removed. In the 5th and the 6th weeks range of motion exercises, stretching and proprioception exercise programme were performed by the sports medicine specialist. The patient started technical workout and training with the team, after the muscle strength was found to be proximate with that of the contralateral limb according to isokinetic test evaluation at the 5th month.
Fig. 1.

AP and lateral plain radiographs of the injured extremity.
Fig. 2.
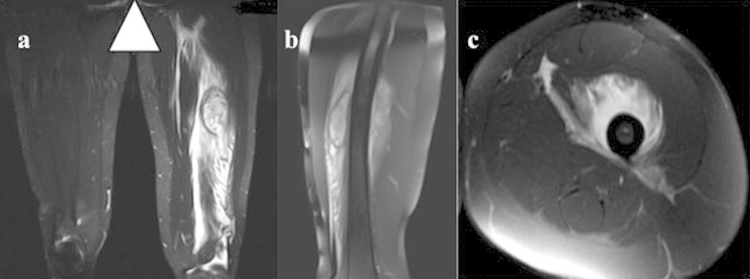
T2 sequence reveals the rupture of the tendon on coronal, (a) sagittal (b) and axial (c) planes.
3. Discussion
Quadriceps tendon ruptures generally occur after the 4th decade in the presence of degenerative changes [7]. Systemic or local steroids, statins, fluoroquinolons may lead to these [10–13]. Also, disorders such as renal insufficiency, hyperparathyroidism, romatoid arthritis, obesity, gout and systemic lupus erythematosus may induce ruptures [14–16]. On the other hand, trauma is the main etiology in the young population [6,8,17]. The most common mechanism for this injury is eccentric overloading of the extensor mechanism when the knee is flexed with plantar flexion of the foot [4]. The mechanism was also similar in our case. There was no history of comorbidity or medical treatment that might lead the rupture.
The components of the quadriceps tendon (rectus femoris, vastus medialis, vastus lateralis and vastus intermedius) may be attached to patella as a whole, whereas there are also some anatomical studies demonstrating that they can be attached seperately [2,18]. This diversity can explain why the quadriceps tendon is ruptured sometimes totally and sometimes partially. Some studies performed with MRI also demonstrated that T1 and T2 sequences may reveal the tendon to consist of different layers [2,19]. We have used MRI as the imaging tool for the evaluation. MRI revealed isolated rupture of vastus intermedius tendon. This structure is in the deepest layer. Thus, we have preferred conservative treatment. Similarly, Aydemir et al. claimed that they had good results with conservative treatment by keeping the injured extremity in cast for 3 weeks [8], Weber et al. also reported that they have conservatively treated a patient with isolated distal rectus femoris tendon rupture and had good functional outcome [7].
In conclusion, we report the first case of isolated rupture of the vastus intermedius tendon in the literature and we claim that disorder may be succesfully treated with conservative treatment and adequate physiotheraphy.
Funding
None.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
EÇ, CGA, YEA, MG, YA, OEA and YSK were involved in the conception, design and interpretation. EÇ, CGA and YEA wrote the manuscript. MG, YA, OEA and YSK collected data, reviewed relevant published reports and provided the images. All authors read and approved the final manuscript.
Guarantor
Engin Çetinkaya M.D.
Conflict of interest statement
None.
References
- 1.Mink J., Deutsch A. Raven; Newyork: 1989. MRI of the Musculoskeletal System. [Google Scholar]
- 2.Zeiss J., Saddemi S.R., Ebraheim N.A. MR imaging of the quadriceps tendon: normal layered configuration and its importance in cases of tendon rupture. AJR Am. J. Roentgenol. 1992;159.5:1031–1034. doi: 10.2214/ajr.159.5.1414770. [DOI] [PubMed] [Google Scholar]
- 3.Jane I. Churchill Livingstone; 1984. Anatomy of the Knee; p. 17. [Google Scholar]
- 4.Rasul T., Fischer David A. Primary repair of quadriceps tendon ruptures: results of treatment Abraham. Clin. Orthop. Relat. Res. 1993;289:205–207. [PubMed] [Google Scholar]
- 5.Siwek Christpher W., Rao J.P. Ruptures of the extensor mechanism of the knee joint. J. Bone Joint Surg. 1981;63.6:932–937. [PubMed] [Google Scholar]
- 6.Martin Boublik. Quadriceps tendon injuries in national football league players. Am. J. Sports Med. 2013;41.8:1841–1846. doi: 10.1177/0363546513490655. [DOI] [PubMed] [Google Scholar]
- 7.Martin Weber. Nonoperative treatment of a complete distal rectus femoris muscle tear. Clin. J. Sport Med. 2010;20.6:493–494. doi: 10.1097/JSM.0b013e3181fb5385. [DOI] [PubMed] [Google Scholar]
- 8.Aydemir Gokhan, Cakmak Selami, Aydinoz Secil. Partial rupture of the quadriceps muscle in a child. BMC Musculoskelet. Disord. 2010;11.1:214. doi: 10.1186/1471-2474-11-214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Majeed Haroon. Prepatellar continuation rupture: report of an unusual case. Knee. 2014;21.5:979–981. doi: 10.1016/j.knee.2014.07.002. [DOI] [PubMed] [Google Scholar]
- 10.Battista Vincent, Combs Jan, Warme Winston J. Asynchronous bilateral achilles tendon ruptures and androstenediol use. Am. J. Sports Med. 2003;31.6:1007–1009. doi: 10.1177/03635465030310060201. [DOI] [PubMed] [Google Scholar]
- 11.Casparian J. Michael. Quinolones and tendon ruptures. Southern medical journal. 2000;93.5:488–491. [PubMed] [Google Scholar]
- 12.Celik Enrim Coskun. Simultaneous and spontaneous bilateral quadriceps tendons rupture. Am. J. Phys. Med. Rehabil. 2012;91.7:631–634. doi: 10.1097/PHM.0b013e3182555dbb. [DOI] [PubMed] [Google Scholar]
- 13.David H.G. Simultaneous bilateral quadriceps rupture: a complication of anabolic steroid abuse. J. Bone Joint Surg. 1995;77:159. [PubMed] [Google Scholar]
- 14.Bhole R., Johnson J.C. Bilateral simultaneous spontaneous rupture of quadriceps tendons in a diabetic patient. South. Med. J. 1985;78.4:486. doi: 10.1097/00007611-198504000-00033. [DOI] [PubMed] [Google Scholar]
- 15.Konrath Gregory A. Outcomes following repair of quadriceps tendon ruptures. J. Orthop. Trauma. 1998;12.4:273–279. doi: 10.1097/00005131-199805000-00010. [DOI] [PubMed] [Google Scholar]
- 16.Lombardi L.J., Cleri D.J., Epstein E. Bilateral spontaneous quadriceps tendon rupture in a patient with renal failure. Orthopedics. 1995;18.2:187. doi: 10.3928/0147-7447-19950201-18. [DOI] [PubMed] [Google Scholar]
- 17.Gamradt Seth C. Nonoperative treatment for proximal avulsion of the rectus femoris in professional American football. Am. J. Sports Med. 2009;37.7:1370–1374. doi: 10.1177/0363546509333477. [DOI] [PubMed] [Google Scholar]
- 18.Andrikoula Sofia. The extensor mechanism of the knee joint: an anatomical study. Knee Surg. Sports Traumatol. Arthrosc. 2006;14.3:214–220. doi: 10.1007/s00167-005-0680-3. [DOI] [PubMed] [Google Scholar]
- 19.Yu Joseph S. MR imaging of injuries of the extensor mechanism of the knee. Radiographics. 1994;14.3:541–551. doi: 10.1148/radiographics.14.3.8066269. [DOI] [PubMed] [Google Scholar]