

Abstract
Purpose
This study was performed to compare the metal artifacts from common metal orthodontic brackets in magnetic resonance imaging.
Materials and Methods
A dry mandible with 12 intact premolars was prepared, and was scanned ten times with various types of brackets: American, 3M, Dentaurum, and Masel orthodontic brackets were used, together with either stainless steel (SS) or nickel titanium (NiTi) wires. Subsequently, three different sequences of coronal and axial images were obtained: spin-echo T1-weighted images, fast spin-echo T2-weighted images, and fluid-attenuated inversion recovery images. In each sequence, the two sequential axial and coronal images with the largest signal-void area were selected. The largest diameters of the signal voids in the direction of the X-, Y-, and Z-axes were then measured twice. Finally, the mean linear values associated with different orthodontic brackets were analyzed using one-way analysis of variation, and the results were compared using the independent t-test to assess whether the use of SS or NiTi wires had a significant effect on the images.
Results
Statistically significant differences were only observed along the Z-axis among the four different brands of orthodontic brackets with SS wires. A statistically significant difference was observed along all axes among the brackets with NiTi wires. A statistically significant difference was found only along the Z-axis between nickel-free and nickel-containing brackets.
Conclusion
With respect to all axes, the 3M bracket was associated with smaller signal-void areas. Overall, the 3M and Dentaurum brackets with NiTi wires induced smaller artifacts along all axes than those with SS wires.
Keywords: Magnetic Resonance Imaging, Orthodontic Brackets, Artifacts, Orthodontic Wires
Introduction
Magnetic resonance imaging (MRI) is an important diagnostic method that has the ability to improve soft tissue contrast without using ionizing radiation.1,2
Artifacts are one of the most important features of MRI images. An artifact is defined as a distortion in MRI signal intensity with no identifiable anatomical source in the imaging field.3 MRI artifacts include motion artifacts caused by patient movement, saturation artifacts resulting from blood flow, chemical artifacts due to changes in the chemical bonding of molecules under a strong magnetic field, and metal artifacts.4
In dentistry, the loss of signal and distortion of MRI images of the head and neck can be caused by dental alloys, and is considered to be a major problem.5 These artifacts can be seen as a 'black hole' in the form of an area of low signal intensity that is surrounded by a zone of high signal intensity, which may have an adverse effect on the diagnostic accuracy of MRI findings.6,7,8
In recent years, the number of orthodontic patients treated with fixed orthodontic appliances who have been referred for MRI has increased. Although MRI is not a routine imaging technique in dentistry, orthodontic patients with a previous pathological lesion need to have MRI scans performed at regular intervals. This presents a challenge for orthodontists to help radiologists eliminate or reduce the artifacts caused by orthodontic brackets, because any kind of orthodontic treatment should not interfere with the patient's medical treatment.
Since an insufficient number of studies have evaluated the artifacts caused by brackets made of different materials, fixed orthodontic treatment is widespread among the general population, and it is important to arrive at a decision about whether to remove a bracket before performing MRI, the aim of this basic study was to compare the effects that orthodontic metal brackets have on signal void reduction within a magnetic field. This study focused on the quantitative effect of metal brackets of different brands on the severity of metal artifacts.
Materials and Methods
In this experimental in vitro study, a dry human mandible was used, in which 12 intact premolar teeth were set in prepared sockets from the right first molar to the left first molar. The premolar teeth were kept in a 1% thymol solution after removing the soft tissue by scalpel to prevent drying. Before the teeth were set in the dry mandible, they were polished with pumice paste.
In this study, we used four different kinds of brackets that are commonly used in practice: Dentaurum (Ispringen, Germany), Masel (Carlsbad, CA, USA), American (Sheboygan, WI, USA), and 3M Unitek (Monrovia, CA, USA).
We also used two types of orthodontic wires: nickel titanium (NiTi) (G&H Orthodontics, Franklin, IN, USA) and stainless steel (SS) (G&H Orthodontics, Franklin, IN, USA). Both types of wires were 0.41 mm in diameter, and were used with each kind of bracket. On the last tooth on each side, a buccal tube was bonded and fixed. The brackets were bonded with composite onto the teeth (Fig. 1).
Fig. 1. The brackets are bonded with composite onto the teeth for performing magnetic resonance imaging.

The prepared model was placed in a plastic cylindrical chamber containing starch. The plastic cylindrical container had no effect on the magnetic field. Corn starch was then dissolved in water (4 : 1) and was poured into the cylindrical chamber up to one quarter of the height of the container.
During the hardening of the starch solution, the prepared model was placed in the center of the container, the chamber was filled with a starch solution, and the mandible was embedded in the starch (Figs. 2A and B). This process was repeated for each imaging session after changing the bracket or the wire. It should be noted that during the first step, MRI images were taken from the prepared mandible before any brackets were applied, and we did not find metal artifacts in the image sequences.
Fig. 2. A and B. The mandible is fixed in the starch mixture.

In order to minimize the effect of other variables, the mandible and the dental arch were the same; and the imaging model was therefore unchanged. Only the brackets or wires were changed for each scan.
A 1.5-T MRI device (Phillips Co., Eindhoven, Netherlands) was used for MRI scanning. Overall, the prepared sample was imaged eight times, with the following combinations of brackets (American, 3M, Dentaurum, and Masel) and wires (SS and NiTi): American SS, American NiTi, 3M SS, 3M NiTi, Dentaurum SS, Dentaurum NiTi, Masel SS, and Masel NiTi.
We also imaged one bracket type that contained nickel (Dentaurum) and another that was nickel-free (Masel) without applying wires. Two sets of MRI images were subsequently taken from these brackets without wires. We obtained the mean signal-void areas that were induced by these brackets without wires and compared them with the corresponding brackets with NiTi wires.
The container holding the mandible was put into a head and neck coil chamber, in the same way that the patient's head is routinely placed in the apparatus. Three different sequences of coronal and axial images were prepared: spin-echo T1-weighted (SET1) images, fast spin-echo T2-weighted (FSET2) images, and fluid-attenuated inversion recovery (FLAIR) images. Most of these imaging sequences are generally used for the maxillofacial, head, and neck regions. The scanning parameters of the different sequences are presented in Table 1.
Table 1. The scanning parameters of the different sequences of magnetic resonance imaging.
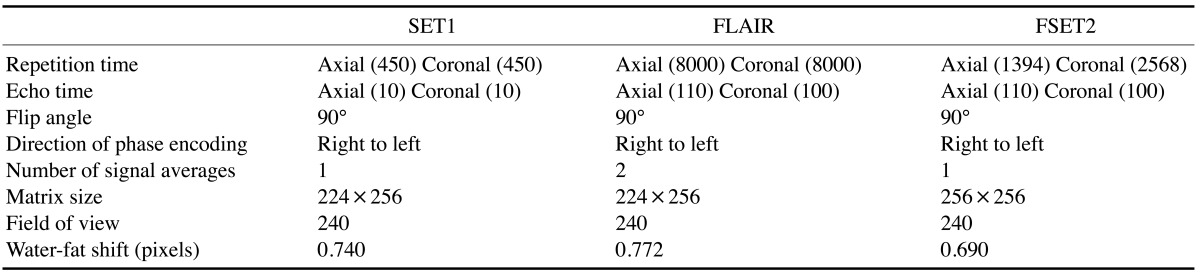
SET1: spin-echo T1-weighted, FSET2: fast spin-echo T2-weighted, FLAIR: fluid-attenuated inversion recovery.
All MRI images that were captured in the three sequences were evaluated in iQ-view version 2.6, 2009 (IMAGE Information Systems Ltd., London, UK). Then, in each sequence of axial images, the two sequential axial images that had the most signal-free zones were chosen. The maximum diameter of the signal void detected along the X- and Y-axes was measured twice semi-automatically on each axial cut by using the measurement tool of the iQ-view software. Similarly, when using two selected coronal images, the maximum height of the signal-free zone was measured along the Z-axis. (Figs. 3, 4, 5). Subsequently, the mean values of the four measurements (two times each for two cuts) taken along the X-, Y-, and Z-axes in each sequence were calculated. New mean values were then determined from the above-described mean values of the three sequences.
Fig. 3. Axial (A) and coronal (B) images reveal various measurements of signal-void areas along the X-, Y-, and Z-axes detected in the different imaging sequences for American-brand brackets with NiTi wire.

Fig. 4. Axial (A) and coronal (B) views reveal the various measurements of the signal-void areas along the X-, Y-, and Z-axes in the different imaging sequences for Dentaurum-brand brackets with nickel titanium wires.

Fig. 5. Axial (A) and coronal (B) views show the various measurements of the signal-void areas found along the X-, Y-, and Z-axes in the different imaging sequences for Masel-brand brackets with stainless steel wires.

In the mid-sagittal area of the SET1 sequence, we also measured the height (H) of the signal-free zones caused by metal artifacts.
Finally, the measured quantitative values from the different sequences of MRI imaging were assessed by one-way analysis of variation (ANOVA) among the different bracket brands with SS or NiTi wires, and also between the brackets that contained nickel (Dentaurum, 3M, America) and those that were nickel-free (Masel). Moreover, the measured values of the signal-void diameters calculated in the different MRI sequences were compared between the SS and NiTi wires for each brand using the independent t-test. The level of significance was set at P<0.05. A post hoc test was performed to characterize the differences that occurred between the groups.
Results
After stabilizing the various orthodontic brackets on the dental arch of the dry mandible, ten sets of MRI scans were obtained. The quantitative values of the signal-free areas associated with the different types of orthodontic brackets were evaluated as follows.
First, the mean quantitative values of the signal-free zones caused by metal artifacts were assessed in the three sequences (SET1, FSET2, and FLAIR) along the X-, Y-, and Z-axes for four orthodontic brands (American, 3M, Dentaurum, and Masel); a significant difference among these brands was only found along the Z-axis (P=0.001). The American brand of bracket had the highest level and the Dentaurum type had the lowest level of signal-free zones occurring along all axes (Table 2).
Table 2. Comparison of the mean signal void values measured along the X-, Y-, and Z-axes for four brands of orthodontic brackets with either SS or NiTi wires.
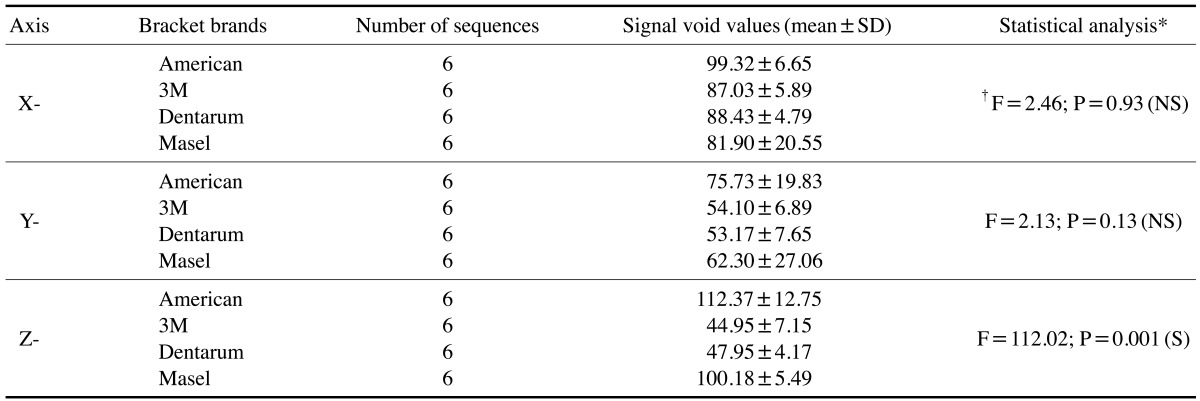
*One-way analysis of variation, †Degrees of freedom, SS: stainless steel, NiTi: nickel titanium, SD: standard deviation, NS: not significant, S: significant.
Tukey's post hoc test showed that significant differences existed between the American and the 3M brackets (P=0.001) as well as between the American and the Dentaurum brackets (P=0.001). In addition, significant differences were observed between the Masel and the Dentaurum brackets (P=0.001) and the Masel and the 3M brackets (P=0.001) with regard to the mean quantitative values of signal-free zones caused by metal artifacts along the Z-axis.
Likewise, the mean quantitative values of signal-free zone values (reflecting six values; two values for each of the three imaging sequences) were studied along the X-, Y-, and Z-axes for the four orthodontic brands (American, 3M, Dentaurum and Masel) with SS wires, as presented in Table 3.
Table 3. Comparison of the mean signal void values measured along the X-, Y-, and Z-axes for four brands of orthodontic brackets with SS wires.
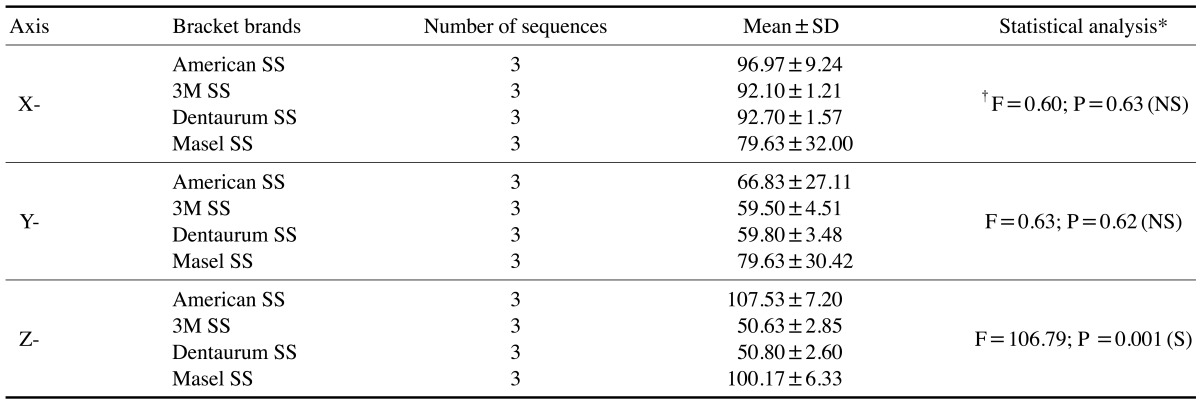
*One-way analysis of variation, †Degrees of freedom, SS: stainless steel. SD: standard deviation, NS: not significant, S: significant.
Table 4 displays a comparison of the mean quantitative signal void values along the X-, Y- and Z-axes in the three imaging sequences for the four different orthodontic brands (American, 3M, Dentaurum, and Masel) with NiTi wires.
Table 4. Comparison of the mean signal void values measured along the X-, Y-, and Z-axes for four brands of orthodontic brackets with NiTi wires.
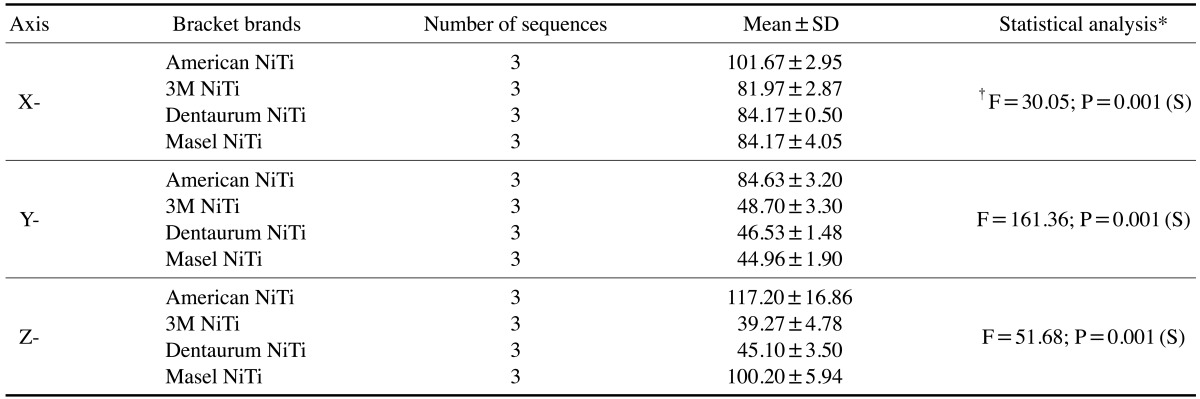
*One-way analysis of variation, †Degrees of freedom, NiTi: nickel titanium, SD: standard deviation, NS: not significant, S: significant.
In the evaluation of the differences of the mean quantitative values of signal-free zones caused by metal artifacts along the Z-axis that occurred between the groups, the results of the post hoc test for the four orthodontic brands studied with SS and NiTi wires were the same as the overall comparison of the four types of orthodontic brackets.
However, the post-hoc test found significant differences between the American and the 3M brackets with NiTi wires (P=0.001), the Dentaurum brackets with NiTi wires (P=0.001), and the Masel brackets with NiTi wires (P=0.001), in terms of the mean quantitative values of signal-free zones caused by metal artifacts along the X- and Y-axes.
The mean values of the signal void zones found along the X-, Y-, and Z-axes based on a comparison of the bracket types with SS and NiTi wires are presented in Table 5.
Table 5. The mean values of signal-free zones measured along the X-, Y-, and Z-axes depending on whether SS or NiTi wires were used with a given orthodontic bracket.
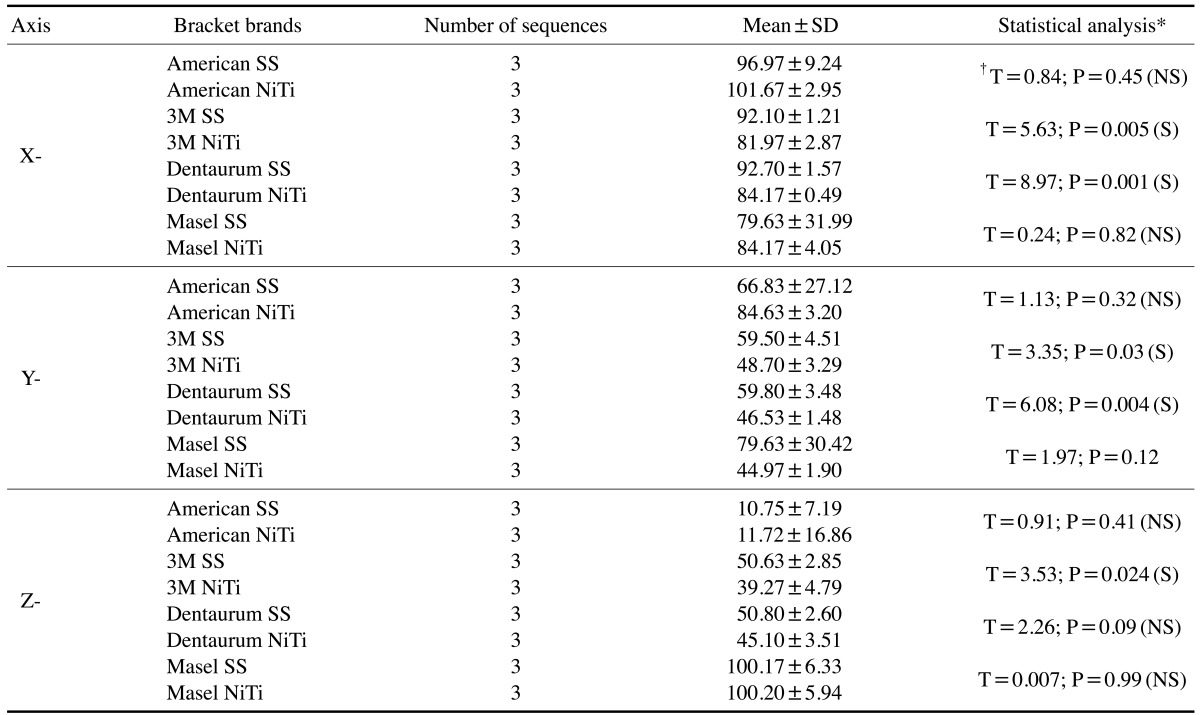
*Independent t-test, †T-value, SS: stainless steel, NiTi, nickel titanium, SD: standard deviation, NS: not significant, S: significant.
Nickel-containing and nickel-free brackets were matched to their corresponding signal-void area values in three different sequences without considering the type of wires used, as shown in Table 6. In Table 6, the results from the images of all three nickel-containing brackets with both types of wires are compared with those of one nickel-free bracket with both types of wires.
Table 6. Comparison of the mean values of signal-free zones between the nickel-containing brackets (Dentaurum, 3M and American) and those that were nickel-free (Masel).
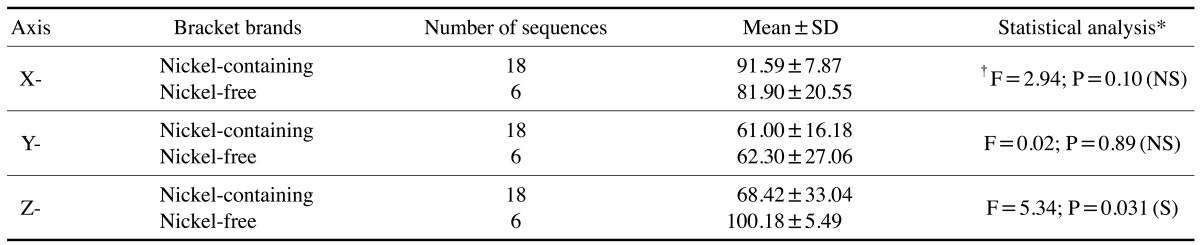
*One-way analysis of variation, †Degrees of freedom, SD: standard deviation, NS: not significant, S: significant.
In the mid-sagittal area of the SET1 sequence, we also measured the height (H) of signal-free zones caused by metal artifacts. The maximum H value was detected in the Masel brackets with SS wires (136.7 mm).
Overall, the Masel brand (SS, NiTi) showed the maximum H values (136.7 and 127.9 mm, respectively), and the American brand with SS wires showed the third highest value (126.9 mm). The minimum H value was found in the Dentaurum bracket with NiTi wires (48.9 mm). In general, higher H values were found with SS wires than with NiTi wires.
The mean quantitative signal void values along the X-, Y-, and Z-axes in the three imaging sequences for the Dentaurum brackets without wire were 80.3±2.15, 43.1±2.49, and 44.7±5.1, respectively. The corresponding values from the Dentaurum orthodontic brackets with NiTi wires were not significantly different. The mean quantitative signal void values along the X-, Y-, and Z-axes determined in the three imaging sequences of the Masel brackets without wires were 82.7±0.85, 98.4±8.19, and 48.8±2.30, respectively. Likewise, the corresponding values for the Masel brackets with NiTi wires were not significantly different.
Discussion
In MRI of the head and neck areas, the presence of ferromagnetic metals in some dental materials causes a nonhomogeneous magnetic field.9 Metal-based materials create individualized magnetic fields and dramatically alter the precession frequencies of protons in adjacent tissues. This inhibits the generation of useful signals and may prevent proper diagnosis.10
In the FLAIR sequence, a long echo time produces very heavy T2 weighting, and a long inversion time suppresses the signal from fluids and reduces flow artifacts. Thus, anatomical details are seen well.11
Costa et al.12 concluded that major metal orthodontic devices create artifacts in brain MRI scans. In their study, imaged metal artifacts and their origins were determined and the level of artifacts in each image was scored from 0 to 1. They found 70 MRI images with artifacts over a four-year period. Orthodontic devices were associated with the highest levels of artifact production. Several studies13,14,15 have also suggested that orthodontic devices interfere with MRI.
In this investigation, we found a statistically significant difference in the signal-void areas created by the four different orthodontic bracket brands along the Z-axis. The American brand was associated with the highest amount of signal-free zones, while the Dentaurum brand had the lowest amount of signal-free zones.
We then compared the mean quantitative values of signal-free zones along the X-, Y-, Z-axes in three imaging sequences for the four previously mentioned orthodontic brands with SS wires. No significant statistical differences were observed along the X- and Y-axes, but significant differences were observed along the Z-axis. The American SS type had the highest level of signal-free zones, while the Dentaurum SS was associated with the lowest level of signal-free zones. Consequently, in MRI images of patients who are undergoing orthodontic treatment and who have these specific orthodontic brackets with SS wires, the location of the lesion and the area under study in the vertical dimension is especially important.
In our study, the mean quantitative values of signal-free zones were evaluated for four different orthodontic brands with NiTi wires. We found that NiTi wires had a significant negative effect on the intensity of the magnetic field, decreasing the size of the signal-void area in comparison with SS wires. In all three axes, the American NiTi type had the highest level of signal-free zones, while the 3M NiTi type had the lowest level.
Overall, we found that the 3M and Dentaurum orthodontic brackets with SS wires induced more signal-free zones than the corresponding brackets with NiTi wires. Thus, changing the orthodontic wires from SS to NiTi did not affect the outcomes of the Masel and American brands, but did have an impact on the outcomes of the 3M and Dentaurum brackets.
Shellock et al.16 reviewed various studies related to the safety of performing MRI with respect to 16 tested dental materials and devices containing ferromagnetic materials, and found that only three samples (SS, amalgam, and silver point) caused a problem for patients during MRI scanning, as these materials are magnetically activated.
In another study, Okano et al.17 suggested that ceramic brackets applied to the anterior teeth and metal bonded tubes on the molar teeth do not have a direct effect on the diagnostic quality of MRI or on temporomandibular joint imaging. SS materials and other metals that are used in dentures created a considerable number of artifacts that tended to obscure the details of MRI images in the facial area.
Morikuni et al.18 conducted a study to examine the production of metal artifacts by multibracket devices while performing MRI of the oral cavity when brackets having different arch wires are present. The SS wires that were used in their study contained 98% ferromagnetic and paramagnetic materials, and therefore had a considerable capacity to interfere with magnetic field gradients. Similarly, in the present study, we found that brackets with SS wires induced more metal artifacts.
Patel et al.19 concluded that SS arch wires, removable orthodontic appliances, palatal bars, and removable lingual arches should be removed before MRI scanning.
The results of several studies15,16,17,18,19,20 have likewise underscored the ability of SS wires to create metal artifacts in MRI.
Nickel is a ferromagnetic material, and this kind of material leads to major distortions of magnetic fields and the loss of MRI signals. However, our study did not show a significant statistical difference in artifacts along the X- and Y-axes between the nickel-free brackets and the brackets that contained nickel.
Hasegawa et al.13 conducted a study to estimate the risk of injury secondary to the heating of orthodontic metal devices caused by the radiofrequency signals found in 3-T MRI. They estimated this potential risk and found that a higher maximum temperature and, correspondingly, a higher level of risk was associated with orthodontic appliances that showed radiofrequency heating above the standard industrial level. Therefore, they suggested that the orthodontic wires should be removed from the brackets or that a spacer should be placed between the appliance and the oral mucosa during MRI.
It would seem that orthodontic brackets with NiTi wires are preferable, due to the negative effect of SS wires on magnetic fields in our study and the categorization of the SS alloy as an unsafe material in another MRI investigative report.20 However, in our study, the presence or absence of NiTi wires was not associated with significant differences in the extent of artifacts in two types of orthodontic brackets (Dentaurum and Masel).
The details of the metal content of the brackets and wires used herein were not clear, because this information was not available due to industrial security concerns. This was, therefore, one of the limitations of our study. It should be kept in mind that this study is a relatively simple study of the effects of wires and brackets on magnetic fields and was performed under routine conditions. When making decisions about whether to remove the brackets or wires, variables such as radiofrequency heating and the location of the lesion are important.
In conclusion, the 3M orthodontic brackets seemed to cause smaller signal-free zones, especially in combination with NiTi wires. Overall, the 3M and Dentaurum orthodontic brackets with NiTi wires induced fewer artifacts than the same brackets with SS wires. The effects of nickel-free orthodontic brands compared to nickel-containing brands on the magnitude of signal-free zones were not major.
Acknowledgements
We would like to thank Ms. Julie Monti Safari for her dedication in editing the present article. In addition, we wish to express our gratitude to Mr. Abdollah Namkkar for his constant assistance in taking MRI scans of samples that were brought to the Radiology Department of Poursina Hospital in Rasht, Iran.
References
- 1.Shafiei F, Honda E, Takahashi H, Sasaki T. Artifacts from dental casting alloys in magnetic resonance imaging. J Dent Res. 2003;82:602–606. doi: 10.1177/154405910308200806. [DOI] [PubMed] [Google Scholar]
- 2.Idiyatullin D, Corum C, Moeller S, Prasad HS, Garwood M, Nixdorf DR. Dental magnetic resonance imaging: making the invisible visible. J Endod. 2011;37:745–752. doi: 10.1016/j.joen.2011.02.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Behr M, Fellner C, Bayreuther G, Leibrock A, Held P, Fellner F, et al. MR-imaging of the TMJ: artefacts caused by dental alloys. Eur J Prosthodont Restor Dent. 1996;4:111–115. [PubMed] [Google Scholar]
- 4.Hargreaves BA, Worters PW, Pauly KB, Pauly JM, Koch KM, Gold GE. Metal-induced artifacts in MRI. AJR Am J Roentgenol. 2011;197:547–555. doi: 10.2214/AJR.11.7364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bennett LH, Wang PS, Donahue MJ. Artifacts in magnetic resonance imaging from metals. J Appl Phys. 1996;79:4712–4714. [Google Scholar]
- 6.Bui FM, Bott K, Mintchev MP. A quantitative study of the pixel-shifting, blurring and nonlinear distortions in MRI images caused by the presence of metal implants. J Med Eng Technol. 2000;24:20–27. doi: 10.1080/030919000294003. [DOI] [PubMed] [Google Scholar]
- 7.Sadowsky PL, Bernreuter W, Lakshminarayanan AV, Kenney P. Orthodontic appliances and magnetic resonance imaging of the brain and temporomandibular joint. Angle Orthod. 1988;58:9–20. doi: 10.1043/0003-3219(1988)058<0009:OAAMRI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Pusey E, Lufkin RB, Brown RK, Solomon MA, Stark DD, Tarr RW, et al. Magnetic resonance imaging artifacts: mechanism and clinical significance. Radiographics. 1986;6:891–911. doi: 10.1148/radiographics.6.5.3685515. [DOI] [PubMed] [Google Scholar]
- 9.Hopper TA, Vasilic B, Pope JM, Jones CE, Epstein CL, Song HK, et al. Experimental and computational analyses of the effects of slice distortion from a metallic sphere in an MRI phantom. Magn Reson Imaging. 2006;24:1077–1085. doi: 10.1016/j.mri.2006.04.019. [DOI] [PubMed] [Google Scholar]
- 10.Klinke T, Daboul A, Maron J, Gredes T, Puls R, Jaghsi A, et al. Artifacts in magnetic resonance imaging and computed tomography caused by dental material. PLoS One. 2012;7:e31766. doi: 10.1371/journal.pone.0031766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hajnal JV, Bryant DJ, Kasuboski L, Pattany PM, De Coene B, Lewis PD, et al. Use of fluid attenuated inversion recovery (FLAIR) pulse sequences in MRI of the brain. J Comput Assist Tomogr. 1992;16:841–844. doi: 10.1097/00004728-199211000-00001. [DOI] [PubMed] [Google Scholar]
- 12.Costa AL, Appenzeller S, Yasuda CL, Pereira FR, Zanardi VA, Cendes F. Artifacts in brain magnetic resonance imaging due to metallic dental objects. Med Oral Patol Oral Cir Bucal. 2009;14:E278–E282. [PubMed] [Google Scholar]
- 13.Hasegawa M, Miyata K, Abe Y, Ishigami T. Radiofrequency heating of metallic dental devices during 3.0 T MRI. Dentomaxillofac Radiol. 2013;42:20120234. doi: 10.1259/dmfr.20120234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Farahani K, Sinha U, Sinha S, Chiu LC, Lufkin RB. Effect of field strength on susceptibility artifacts in magnetic resonance imaging. Comput Med Imaging Graph. 1990;14:409–413. doi: 10.1016/0895-6111(90)90040-i. [DOI] [PubMed] [Google Scholar]
- 15.Harris TM, Faridrad MR, Dickson JA. The benefits of aesthetic orthodontic brackets in patients requiring multiple MRI scanning. J Orthod. 2006;33:90–94. doi: 10.1179/146531205225021465. [DOI] [PubMed] [Google Scholar]
- 16.Shellock FG, Kanal E. Aneurysm clips: evaluation of MR imaging artifacts at 1.5 T. Radiology. 1998;209:563–566. doi: 10.1148/radiology.209.2.9807590. [DOI] [PubMed] [Google Scholar]
- 17.Okano Y, Yamashiro M, Kaneda T, Kasai K. Magnetic resonance imaging diagnosis of the temporomandibular joint in patients with orthodontic appliances. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95:255–263. doi: 10.1067/moe.2003.37. [DOI] [PubMed] [Google Scholar]
- 18.Morikuni H, Koseki T, Yotsui Y, Matsumoto N. Metallic artifacts on magnetic resonance images caused by multibracket appliances. J Osaka Dent Univ. 2010;44:13–21. [Google Scholar]
- 19.Patel A, Bhavra GS, O'Neill JR. MRI scanning and orthodontics. J Orthod. 2006;33:246–249. doi: 10.1179/146531205225021726. [DOI] [PubMed] [Google Scholar]
- 20.Kemper J, Priest AN, Schulze D, Kahl-Nieke B, Adam G, Klocke A. Orthodontic springs and auxilliary appliance: assessment of magnetic field interactions associated with 1.5 T and 3 T magnetic resonance systems. Eur Radiol. 2007;17:533–540. doi: 10.1007/s00330-006-0335-x. [DOI] [PubMed] [Google Scholar]