

Abstract
Background:
Noise-induced hearing loss (NIHL) is usually one of the main problems in industrial settings. The aim of this study was to determine whether changes in the signal-to-noise ratio (SNR) in different DPOAE are caused by exposure to different levels of noise at different time intervals among workers exposed to noise.
Methods:
This case-control study was conducted in the autumn of 2014 on 45 workers at Gol Gohar Mining and Industrial Company, which is located in Sirjan in southeast Iran. The workers were divided into three groups based on their noise exposure, i.e., 1) 15 office workers as a control group with exposure to low levels of noise, 2) 15 workers from manufacturing departments who were exposed to a medium level of noise, and 3) 15 workers from manufacturing departments who were exposed to high levels of noise. The SNRs at the frequencies of 1000, 2000, 3000, 4000, and 6000 Hz were measured in both ears at three different time intervals during the shift work. SNRs of 6 or greater were considered as inclusion criterion. Repeated measures, the Spearman rank-order correlation test, and paired t-test analyses were used with α = 0.05 being the level of significance.
Results:
For all frequencies in the right and left ears, the SNR values were more than 6, thus all SNR values were considered as acceptable responses. The effects of time and sound pressure level (SPL) on SNR were significant for the right and left ears (p = 0.027 and < 0.001, respectively). There was a statistically significant correlation between the SNR values in the right and left ears for the time intervals 7:30–8:00 A.M. and 13:30–14:00 P.M., which implied that an increase in the duration of exposure led to reduced SNR values (p = 0.024, r = 0.948).
Conclusions:
The comparison of the SNR values in the right and left ears (for all frequencies and the three different SPLs) indicated that the values decreased during the shift work.
Keywords: hearing loss, noise-induced, otoacoustic emissions, signal-to-noise ratio
1. Introduction
Noise is considered to be the most common occupational hazard in industries in developed and developing countries (1). More than 60 million people in the world are exposed to excessive noise levels (> 85 dBA) in their work environments (2). Harmful effects of noise have been identified (3), and when the noise level exceeds a certain threshold, it can have harmful effects on various aspects of the human body, such as hearing, circulation of the blood, the functioning of the mind, and work performance (4). The most important and certain effect of noise is hearing loss, and this is one of the most significant occupational hazards. Therefore, the damage to hearing that results from excessive noise has been reported to be one of top 10 harmful work-related factors (5, 6). Various studies have indicated that 7.4 to 10.2 million people in the U.S. and 30 to 50 million industrial workers in Europe have incurred hearing loss caused by excessive noise. According to the estimates of the World Health Organization (WHO), noise-induced hearing loss (NIHL) has imposed a financial burden of about four million U.S. Dollars (7, 8). Loss of hearing results from the damage caused to hair cells (HCs) by excessive noise. This damage generally causes hearing loss and sometimes causes other defects in hearing (9).
Several studies have been conducted that used industrial approaches and pure tone testing to determine the effects of noise on hearing loss and the likely mechanisms involved. However, since such tests have some significant limitations, including their non-objectivity, low sensitivity in the diagnosis of defects, and failure to provide detailed information about the changes that result from exposures to noise, there is a need for more accurate tests. The initial steps that cause early damage to the hearing system cannot be diagnosed by pure-tone audiometry; rather, this technique can measure damage only after the onset of irreparable damage to the hearing system (10). Otoacoustic emissions (OAEs) that result from DPOAE reflect the performance of the outer hair cells (OHCs), and they serve as a valid test and are useful in assessing changes in cochlea (11, 12).
Otoacoustic emissions are the result of the microscopic biomechanical activities of healthy OHCs. These activities produce mechanical movements in the cochlea that are transferred from the tympanum to the outer ear and are reflected in the auditory canal (13). The cochlea phenomena that create these emissions are called pre-neural phenomena (14), because they occur before a signal is transferred to the auditory nerve. Auditory emissions are very useful in exploring the OHCs of the cochlea (15). Auditory emissions include automotive auditory emissions and evoked otoacoustic emissions (transient otoacoustic, distortion product otoacoustic emission (DPOAE), and motive frequency otoacoustic emissions) (11). Medical tests of otoacoustic emissions have significant advantages over other otoacoustic tests because they are objective, do not require a special acoustic environment, have high precision, and can be performed quickly (16). In this study, the DPOAE test was used to check the otoacoustic performance of the cochlea. DPOAE is one of features of different types of OAEs. The method used to measure DPOAE is to record the emissions made and reinforced in the cochlea by certain frequencies, i.e., f1 and f2 (17). The DPOAE test is an objective and non-aggressive test that uses the properties of frequency sensitivity to determine otoacoustic damage (18). DPOAE is a valid test for detecting otoacoustic damage because it does not require the listener’s cooperation, and, in addition to studying people in the workplace, it can be used to study animals, infants, and older people.
The distinction between the measured OAE emission and the background noise level can be shown by the SNR; hence, when SNR is positive, it can indicate a measurable response over the background noise (19, 20).
However, to date there has been little discussion about the effects of exposure to various sound pressure levels based on SNR. The specific objectives of the study were:
To determine SNRs at three time intervals for frequencies of 1000, 2000, 3000, 4000, and 6000 Hz in the right and left ears of the workers exposed to different levels of noise.
To assess the effects of various noise levels on the values of the SNR in the right and left ears.
To assess the effects of the duration of exposure to noise on values of the SNR in the right and left ears.
2. Material and Methods
2.1. Participants
This case-control study was performed in the autumn of 2014 on 45 workers at Gol Gohar Mining and Industrial Company in Sirjan, which is situated in southeast Iran. The hearing status of each of the subjects was tested prior to conducting the study. Their general health conditions in terms of cardiovascular and mental conditions also were determined by reviewing their medical records, which ultimately led to the selection of the healthiest individuals. To control the potential confounding effects of shift work, only day shift workers were enrolled in the study.
2.2. Industry selection
Gol Gohar Mining and Industrial Company was selected as an industrial setting for this investigation. The workers are not exposed to thermal stress and vibration in the workplace.
2.3. Sampling method
This case-control study included a control group and two case groups; hence, the participants were selected so that the same number of participants could be place in each of the three groups. Based on previous studies, with a power of 80% and first-type error of 0.05 (α = 0.05), the appropriate number of participants was determined to be 45. The formula used to estimate the number of participants was based on the differences between the studied groups; as a result, the number of participants in each group was determined to be 15.
2.4. Study design
Prior to beginning the experiment, the participants were informed about the aim of the study. A written informed consent form was obtained from each participant indicating her or his willingness to participate in the study. The participants also completed a form that was used to collect demographic data, and their body mass indexes (BMIs) were calculated. A total of 45 workers were enrolled in the study on the basis of noise exposure, 15 office workers as a control group with exposure to low levels of noise, 15 workers from manufacturing departments as a case group exposed to a medium noise level (88 dBA), and 15 workers from manufacturing departments as a case group exposed to high levels of noise (103 dBA). The workers selected for the exposed groups (cases) did not use any hearing protection devices and normally performed light work (based on ISO 8996) (21). The intensities of the SPLs, as the environmental variables, were measured at different locations in the industrial facility. An experienced audiologist conducted the DPOAE test for all of the participants in the control group and in both case groups at three different time intervals, i.e., at the beginning of the shift before any exposure to noise (7:30–8:00 A.M.), during exposure to noise at frequencies of 1000, 2000, 3000, 4000, and 6000 Hz at 10:30–11:00 A.M. and 13:30–14:00 P.M.
Prior to the DPOAE tests, the following requirements were evaluated: 1) Ear canals were free of any blockage, 2) The ear-probe was fitted to the ear canal, 3) The probe was placed correctly in the ear canal, 4) Middle ear disorder was considered, 5) The subjects were calm, and 6) A noise-free environment was provided. (There was no need to perform the test in a sound-proof room) (22).
2.5. Measurement
2.5.1. Noise
Ambient noise was measured (ISO 9612) at each workstation using a sound-level meter (CEL-440) that was calibrated immediately before the measurements were taken using a CEL-282 calibrator (23).
2.5.2. SNR
The DPOAE test device (Vivosonic 2.5.2: Vivosonic, Toronto, Canada) was used to measure SNRs at frequencies of 1000, 2000, 3000, 4000, and 6000 Hz. The main reason for selecting the DPOAE test was its frequency-selective nature. During the test, all of the subjects were in sedentary positions. The f2/f1 was set as 1.22, and the levels of the signals were L1 = 65 dB and L2 = 55 dB. Using small probes, the outer ear channel audio frequencies were sent to the tympanic membrane, and it received the reflected sounds, which were delayed slightly by a microphone that was embedded in the probe.
The test procedures and recordings were performed in a silent room. In this study, the 2f11–f2 SNR was considered and evaluated separately in the subjects’ tight and left ears as a response to DPOAEs at 1000, 2000, 3000, 4000, and 6000 Hz. This range of frequencies was selected due to the susceptibility of the ears to hearing loss within this range. DP-NF also was used to calculate SNRs in studied groups. The SNR of 6 or greater was considered as the inclusion criterion (24, 25).
2.6. Statistical analysis
SPSS version 18 (SPSS, Inc., Chicago, Illinois, United States of America) was used to analyze the collected data using statistical tests, such as the paired t-test, Spearman rank-order correlation test, and repeated measures analysis of variance. The results were considered as significant at p < 0.05.
2.7. Ethical Considerations
Ethical approval was obtained from the Ethics Committee of Tehran University of Medical Sciences (ID: 1394.51). Informed consent was obtained before beginning the study. The data were reported on a confidential basis.
3. Results
3.1. Analysis of demographic characteristics
Table 1 presents the mean age and body mass index of the participants in the three groups that were studied.
Table 1.
Demographic characteristics of the participants
| Variables | Control group exposed to low noise level | Case group exposed to medium noise level | Case group exposed to high noise level |
|---|---|---|---|
| Mean± SD | Mean± SD | Mean± SD | |
| Age (years) | 28.8±2.05 | 30.1±2.37 | 29.4±2.63 |
| BMI (kg/m2) | 25.1±2.28 | 25.5±3.25 | 25.5±2.97 |
3.2. Noise measurement
Having measured the SPLs in the identified locations, the control group was exposed to a maximum level of 72 dBA SPL. The two case groups were exposed to medium and high noise levels of 88 and 103 dBA SPL, respectively.
3.3. Changers in the SNRs in the right and left ears at the frequencies that were studied
In this study, SNR ≥ 6 was considered as the inclusion criterion. After the evaluation of SNRs, it was found that the SNR values were > 6 at all of the frequencies, so all of the SNR values were considered as acceptable responses. Table 2 provides the means and standard deviations of the SNRs at the frequencies of 1000, 2000, 3000, 4000, and 6000 Hz in the right ear at different SPLs and time intervals.
Table 2.
Means and standard deviations of the SNRs at different frequencies in the right ear
| SPL (dB) | Time (h) | Frequency (Hz) | |||||
|---|---|---|---|---|---|---|---|
| 1000 | 2000 | 3000 | 4000 | 6000 | |||
| 72 (Control group) | 7:30–8 A.M. | Mean | 18.45 | 22.45 | 20.80 | 20.95 | 16.15 |
| SD | 1.343 | 3.88 | 1.69 | 5.02 | 8.27 | ||
| 10:30–11 A.M. | Mean | 16.80 | 21.00 | 19.10 | 17.90 | 16.10 | |
| SD | 1.97 | 2.40 | 1.97 | 5.79 | 7.91 | ||
| 13:30–14 P.M. | Mean | 14.90 | 19.05 | 16.80 | 14.70 | 14.75 | |
| SD | 5.51 | 1.767 | 4.66 | 8.76 | 4.31 | ||
| 88 (Case group) | 7:30–8 A.M. | Mean | 23.53 | 20.60 | 21.80 | 20.76 | 18.93 |
| SD | 1.42 | .264 | 2.56 | 2.79 | 6.72 | ||
| 10:30–11 A.M. | Mean | 20.70 | 19.50 | 19.73 | 21.06 | 18.26 | |
| SD | 0.86 | 0.96 | 0.90 | 1.62 | 6.05 | ||
| 13:30–14 P.M. | Mean | 19.23 | 18.70 | 17.66 | 20.16 | 17.33 | |
| SD | 0.30 | 1.56 | 2.34 | 1.50 | 4.29 | ||
| 103 (Case group) | 7:30–8 A.M. | Mean | 20.10 | 21.90 | 22.35 | 20.5 | 25 |
| SD | 0.21 | 0.49 | 0.35 | 0.84 | 1.97 | ||
| 10:30–11 A.M. | Mean | 19.50 | 20.40 | 21.15 | 19.15 | 20.4 | |
| SD | 0.42 | 0.56 | 2.33 | 0.49 | 0.49 | ||
| 13:30–14 P.M. | Mean | 18.40 | 19.25 | 19.85 | 19.10 | 21 | |
| SD | 4.66 | 0.07 | 1.34 | 0.84 | 1.41 | ||
Figure 1 shows the means of the SNRs at frequencies of 1000, 2000, 3000, 4000, and 6000 Hz in the right ear at different SPLs and time intervals. It is evident that time progressed towards the end of the shift work, the SNR values for the right ear decreased. Decreases occurred at all frequencies and all SPLs. Table 3 shows the means of the SNRs of the left ear at frequencies of −1000, 2000, 3000, 4000, and 6000 Hz at different SPLs and time intervals. Figure 2 shows the means of the SNRs at frequencies of 1000, 2000, 3000, 4000, and 6000 Hz in the left ear at different SPLs and time intervals. It was observed that the SNR values decreased as the duration of exposure to the noise increased.
Figure 1.
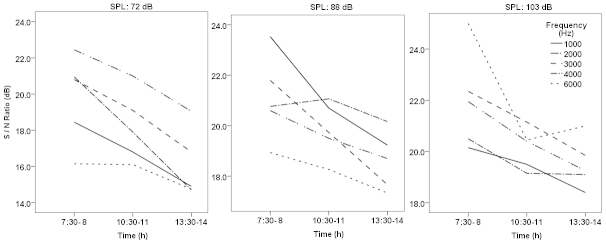
Means of the SNR values at different frequencies in the right ear
Table 3.
Means and standard deviations of the SNRs at different frequencies in the left ear
| SPL (dB) | Time (h) | Frequency (Hz) | |||||
|---|---|---|---|---|---|---|---|
| 1000 | 2000 | 3000 | 4000 | 6000 | |||
| 72 (Control group) | 7:30–8 A.M. | Mean | 17.65 | 22.35 | 21.05 | 21.10 | 22.05 |
| SD | 4.17 | 1.767 | 0.77 | 1.55 | 0.21 | ||
| 10:30–11 A.M. | Mean | 16.95 | 19.65 | 19.55 | 19.60 | 19.55 | |
| SD | 4.87 | 0.91 | 0.07 | 0.28 | 0.35 | ||
| 13:30–14 P.M. | Mean | 13 | 18.60 | 19.10 | 19.25 | 16.40 | |
| SD | 6.61 | 0.42 | 0.28 | 0.21 | 0.42 | ||
| 88 (Case group) | 7:30–8 A.M. | Mean | 24.86 | 21.5 | 21.2 | 23.40 | 18.56 |
| SD | 3.63 | 0.60 | 2.77 | 1.55 | 5.65 | ||
| 10:30–11 A.M. | Mean | 21.70 | 20 | 19.76 | 20.86 | 17.06 | |
| SD | 2.48 | 0.79 | 1.91 | 1.05 | 5.37 | ||
| 13:30–14 P.M. | Mean | 20.93 | 20.13 | 18.50 | 19.73 | 11.83 | |
| SD | 2.08 | 0.30 | 1.04 | 0.73 | 3.55 | ||
| 103 (Case group) | 7:30–8 A.M. | Mean | 22.65 | 20.50 | 21.45 | 23.20 | 23.55 |
| SD | 1.48 | 0.70 | 2.33 | 2.54 | 3.464 | ||
| 10:30–11 A.M. | Mean | 20.10 | 19.05 | 20.15 | 21 | 21.55 | |
| SD | 0.56 | 0.07 | 0.77 | 1.13 | 2.33 | ||
| 13:30–14 P.M. | Mean | 19.80 | 18.20 | 17.65 | 19.45 | 19.75 | |
| SD | 0.56 | 1.41 | 2.33 | 0.35 | 0.77 | ||
Figure 2.
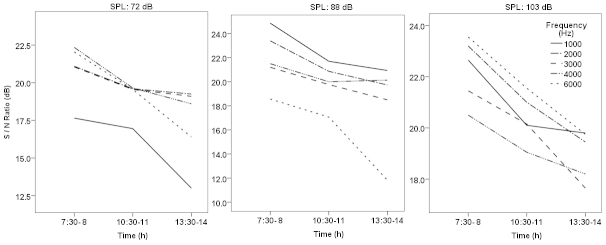
Means of the SNR values at different frequencies in the left ear
3.4. The effects of different factors on the SNR
The statistical method of ‘repeated measures’ was used to study the effect of various factors on the SNR. The results showed that the effects of age and BMI on the SNR were not statistically significant (p > 0.05). The effect of the duration of the measurements on the SNR was statistically significant in both the right and left ear (p = 0.027 and p < 0.001, respectively). The SPL also had a significant effect on the SNR in both the right and left ears (p = 0.023 and p = 0.041, respectively). Further analysis indicated that the SNR values of the right ear at the time intervals of 7:30–8:00 A.M. and 13:30–14:00 P.M. were statistically different (p = 0.024). Nevertheless, such differences between the time intervals 7:30–8:00 A.M. and 10:30–11:00 P.M. and the time intervals 10: 30–11:00 A.M. and 13:30–14:00 P.M. were not statistically significant (p > 0.05). Also, the SNR values of the left ear obtained at the time intervals of 7:30–8:00 A.M. and 13:30–14:00 P.M. were significantly different (p < 0.001). Also, there was a significant difference between the two means of the SNR values of the right and left ears at 3000 Hz for the SPL of 88 dBA.
No significant difference was observed in the other frequencies (p > 0.05). In the SPL of 103 dBA, there was a significant difference between the means at 3000 and 4000 Hz but there was no significant difference at the frequencies of 1000 and 2000 Hz. The results of Spearman rank-order correlation test in control group members exposed to 72 dBA SPL showed that there was a significant correlation between the duration of exposure and SNR values in the left ear at 2000, 3000, and 6000 Hz, and the SNR values decreased as the duration of exposure increased at these frequencies. Also, in the 88 dBA SPL, there was a significant correlation between the duration of exposure and SNR values at 1000, 2000, and 3000 Hz in the right ear. A similar relationship was found for the left ear at frequencies of 2000, 3000, and 4000 Hz. At 103 dBA, there was a statistically-significant correlation between the duration of exposure and SNR values at 2000 Hz in the right ear and at 3000, 4000, and 1000 Hz in the left ear.
4. Discussion
In this study, we evaluated the changes in the SNR using the DPOAE test. All subjects were in sedentary positions during the test. The researchers believed that inappropriate body postures would affect the results of the DPOAE test. The change in body posture changes the pressure inside the skull, and such a change in pressure could, in turn, affect the inner ear via the spiral channel (26). Thus, to eliminate the confounding effects of possible uncomfortable postures on test results, all subjects were placed in a sitting position throughout the tests.
In order to record DPOAE (2f1–f2), two signals, i.e., f1 and f2 (with f2 > f1) were used. The f2/f1 ratio was kept at 1.22, and the levels of these signals were L1 = 65 dB and L2 = 55 dB. The test was performed at frequencies of 1000, 2000, 3000, 4000, and 6000 Hz with an SNR ≥ 6. In the DPOAE test, SNR is commonly measured at frequencies of 2000, 3000, and 4000 Hz, and the SNR ≥ 6 also was considered as the inclusion criterion (24, 27, 28). The evaluation of the SNR values indicated that the SNR values were greater than 6 - in the right and left ear for all of the frequencies, so all of the SNR values were considered as acceptable responses.
Some researchers have performed the DPOAE test on 50 individuals. Four frequencies in the range of 550 to 4000 Hz were used in the study. The f2/f1 ratio of 1.19 for the frequency of 550 Hz and the f2/f1 ratio of 1.21 for the frequencies of 1000, 2000, and 4000 Hz were used with the primary-tone level of 65 dB SPL. The results of study showed that the acceptable measurements for the frequency of 550 Hz were in the range of 42 to 66%. The acceptable measurements for the corresponding frequencies of 1000, 2000, and 4000 Hz were in the range of 92 to 98%, 86 to 96%, and 90 to 96%, respectively (29). Other researchers have used DPOAEs at different f2 frequencies, ranging from 2 to 16 kHz. They made use of various stimulus level conditions for L1/L2 (60/45, 60/50, 70/55, and 70/60). They also reported an SNR value of 6 - or greater for inclusion. The reported acceptable test of 60/50% for the frequency of 9 kHz was 92%. The acceptable tests for frequencies of 11, 13, and 15 kHz were 96, 84, and 76%, respectively (30).
In a prior study, the DPOAE test was conducted on 40 subjects. They used primary-tone levels that ranged from 20 to 60 dB SPL and frequencies that ranged from 1 to 6 kHz. An SNR of 6 - or greater also was used for inclusion, which resulted in the exclusion of four subjects the SNR of 6 - was not met (27). In 2000, Beattie and Bleech conducted the DPOAE test with 55 participants and used a protocol of L1 = L2. The 35, 45 and 55 dB of primary-tone levels at geometric means of the frequencies of 531, 1000, 2000, and 4000 Hz with the ratio of 1.21 were used in the study. Sample sizes of 12, 25, 50, 100, 200, and 400 participants were determined for the study. SNR > 3 - was used for the selection. The frequencies over 1 kHz provided a high proportion of acceptable tests at the 55 dB SPL stimulus level (31).
In another study, researchers used the DPOAE test with 33 participants. They used the ratio of 1.22 for f2/f1. The levels of L1 and L2 were 65 and 55 dB SPL with three points per octave. They included the SNRs above zero in their analysis. The proportion of acceptable tests was obtained in the range of 99% and 82%. The frequency of 4 kHz had the lowest proportion (32). Uchida et al. showed that, with increasing age, DPOAE amplitudes were decreased (33). This study evaluated the effects of age and BMI on the SNR; the results showed that age and BMI did not have significant effects on the SNR. Therefore, after adjusting the effects of age and BMI, we investigated the effects of sound pressure levels and duration of exposure on the SNR. The effects of time and SPL on SNR in the right ear and left ear were significant; the ratio decreased gradually in the left and right ears from the beginning to the end of the work shift. There was a statistically significant relationship between SNR values in the right and left ears at the two specific time periods of7:30–8:00 A.M. and 13:30–14:00 P.M., and the SNR decreased as the duration of exposure increased. The effect of time duration on SNR was more significant in the left ear. This study showed that the frequency of 3000 Hz was affected the most. The findings of the current study are consistent with other studies. In accord with the findings of other researchers, DPOAE was more sensitive to noise at high frequencies, i.e., 3000, 4000, and 6000 Hz (34, 35). In 2005 and 2008, Balatsouras and Edward, respectively, showed that DPOAE was affected mainly at the frequency of −3000 Hz (36, 37). However, the findings of the current study differed from the results obtained by another researcher, who found that DPOAE was most severely affected at 6000 Hz (38). These results are consistent with findings of other studies. In a prior study, the DPOAE test was performed on 50 newborns, and the results showed that 90% of them had acceptable responses to the test. The 3 kHz frequency band also was more affected and had better repeatability (39). Therefore it was concluded that SNR values indicated that the values decreased during shift work in both the right and left ears for all frequencies and the three different SPLs. The limitation of this study was the small number of DPOAE devices that were prepared by the researchers with much effort.
5. Conclusions
This study showed that SNR values in both the right and left ears (in all frequencies and the three different SPLs) decreased during shift work. Since noise is the most common physical stress at workplaces and a high prevalence of hearing loss has been reported among Iran’s industrial workers, further studies should be conducted to prove the importance of the issue for health policy makers.
Acknowledgments
This research was supported by a grant from Tehran University of Medical Sciences and Health Services (project No. 24455). This paper was extracted from Sajad Zare’s Ph.D. thesis, which was supervised by Dr. Parvin Nassiri. The authors thank the staff members at Tehran University of Medical Sciences and Gol Gohar Mining and Industrial Company for their invaluable support.
Footnotes
Conflict of Interest:
There is no conflict of interest to be declared.
Authors’ contributions:
All authors contributed to this project and article equally. All authors read and approved the final manuscript.
References
- 1.Rachiotis G, Alexopoulos C, Drivas S. Occupational exposure to noise, and hearing function among electro production workers. Auris Nasus Larynx. 2006;33(4):381–5. doi: 10.1016/j.anl.2006.03.008. [DOI] [PubMed] [Google Scholar]
- 2.Kopke RD, Weisskopf PA, Boone JL, Jackson RL, Wester DC, Hoffer ME, et al. Reduction of noise-induced hearing loss using L-NAC and salicylate in the chinchilla. Hear Res. 2000;149(1):138–46. doi: 10.1016/S0378-5955(00)00176-3. [DOI] [PubMed] [Google Scholar]
- 3.Sayapathi BS, Su AT, Koh D. The impact of different permissible exposure limits on hearing threshold levels beyond 25 dBA. Iran Red Crescent Med J. 2014;16(10) doi: 10.5812/ircmj.15520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Halvani GH, Zare M, Barkhordari A. Noise induced hearing loss among textile workers of Taban factories in Yazd. Journal of Birjand University of Medical Sciences. 2009;15(4):69–74. (In Persian) [Google Scholar]
- 5.Moussavi-Najarkola S, Khavanin A, Mirzaei R, Salehnia M, Muhammadnejad A, Akbari M. Noise-induced outer hair cells’ dysfunction and cochlear damage in rabbits. Iran Red Crescent Med J. 2012;14(10):647. [PMC free article] [PubMed] [Google Scholar]
- 6.Fouladi D, Nassiri P, Monazzam E, Farahani S, Hassanzadeh G, Hoseini M. Industrial noise exposure and salivary cortisol in blue collar industrial workers. Noise Health. 2012;14(59):184. doi: 10.4103/1463-1741.99894. [DOI] [PubMed] [Google Scholar]
- 7.Ahmed H, Dennis J, Badran O, Ismail M, Ballal S, Ashoor A, et al. Occupational noise exposure and hearing loss of workers in two plants in eastern Saudi Arabia. Ann Occup Hyg. 2001;45(5):371–80. doi: 10.1093/annhyg/45.5.371. [DOI] [PubMed] [Google Scholar]
- 8.Prasher D, Morata T, Campo P, Fechter L, Johnson A-C, Lund SP, et al. NoiseChem: An European Commission research project on the effects of exposure to noise and industrial chemicals on hearing and balance. Noise Health. 2002;4(14):41. [PubMed] [Google Scholar]
- 9.Jovanović J, Popović V, Milošević Z, Jovanović M. Cumulative effects of communal and industrial noise on cardiovascular system. The Scientific Journal Facta Universitatis. 1997;4:57–61. [Google Scholar]
- 10.Manley GA, Fay RR. Active processes and otoacoustic emissions in hearing. Springer Handbook of Auditory Research. 2008;30 ISBN: 978-0-387-7146-77. [Google Scholar]
- 11.Nagy AL, Toth F, Vajtai R, Gingl Z, Jori J, Kiss J. Effects of noise on the intensity of distortion product otoacoustic emissions. Int Tinnitus J. 2002;8(2):94–6. [PubMed] [Google Scholar]
- 12.Kiss JG, Tóth F, Rovó L, Venczel K, Drexler D, Jóri J, et al. Distortion-product otoacoustic emission (DPOAE) following pure tone and wide-band noise exposures. Scand Audiol. 2001;30(1):138–40. doi: 10.1080/010503901300007335. [DOI] [PubMed] [Google Scholar]
- 13.Avan P, Bonfils P. Frequency specificity of human distortion product otoacoustic emissions. In Int J Audiol. 1993;32(1):12–26. doi: 10.3109/00206099309072924. [DOI] [PubMed] [Google Scholar]
- 14.Hall JW. Handbook of otoacoustic emissions. San Diego, CA: Singular; 2000. [Google Scholar]
- 15.Driscoll C, Kei J, McPherson B. Handedness effects on transient evoked otoacoustic emissions in schoolchildren. Jou J Am Acad Audiol. 2002;13(8):403–6. [PubMed] [Google Scholar]
- 16.Driscoll C, Kei J, McPherson B. Outcomes of transient evoked otoacoustic emission testing in 6-year-old school children: a comparison with pure tone screening and tympanometry. Int J Pediatr Otorhinolaryngol. 2001;57(1):67–76. doi: 10.1016/S0165-5876(00)00445-6. [DOI] [PubMed] [Google Scholar]
- 17.Nozza RJ, Sabo DL, Mandel EM. A role for otoacoustic emissions in screening for hearing impairement and middle ear disorders in school-age children. Ear Hear. 1997;18(3):227–39. doi: 10.1097/00003446-199706000-00006. [DOI] [PubMed] [Google Scholar]
- 18.Keppler H, Dhooge I, Maes L, D’haenens W, Bockstael A, Philips B, et al. Transient-evoked and distortion product otoacoustic emissions: A short-term test-retest reliability study. Int J Audiol. 2010;49(2):99–109. doi: 10.3109/14992020903300431. [DOI] [PubMed] [Google Scholar]
- 19.Edwards AL. Measurement of distortion product otoacoustic emissions in South African gold miners at risk for noise-induced hearing loss. University of the Witwatersrand; 2009. [Google Scholar]
- 20.Suryadevara AC, Wanamaker HH, Pack A. The effects of sound conditioning on gentamicin-induced vestibulocochlear toxicity in gerbils. Laryngoscope. 2009;119(6):1166–70. doi: 10.1002/lary.20145. [DOI] [PubMed] [Google Scholar]
- 21.ISO 8996: Ergonomics–Determination of metabolic heat production. International Organization for Standardization; Geneva, Switzerland: 2004. Available from: https://www.iso.org/obp/ui/#iso:std:iso:8996:ed-2:v1:en. [Google Scholar]
- 22.Campbell KCM, M G. Otoacoustic emissions [article online] Available from: http://emedicine.medscape.com/article/835943-overview, updated 15 June 2012; Accessed 20 September 2012.
- 23.ISO 9612: Acoustics—determination of occupational noise exposure—engineering method. International Organization for Standardization; Geneva, Switzerland: 2009. Available from: https://www.iso.org/obp/ui/#iso:std:iso:9612:ed-2:v1:en. [Google Scholar]
- 24.Attias J, Bresloff I, Reshef I, Horowitz G, Furman V. Evaluating noise induced hearing loss with distortion product otoacoustic emissions. Br J Audiol. 1998;32(1):39–46. doi: 10.3109/03005364000000049. [DOI] [PubMed] [Google Scholar]
- 25.Faulstich M, Kössl M. Evidence for multiple DPOAE components based upon group delay of the 2f 1 – f 2 distortion in the gerbil. Hear Res. 2000;140(1):99–110. doi: 10.1016/S0378-5955(99)00189-6. [DOI] [PubMed] [Google Scholar]
- 26.De Kleine E, Wit HP, van Dijk P, Avan P. The behavior of spontaneous otoacoustic emissions during and after postural changes. J Acoust Soc Am. 2000;107(6):3308–16. doi: 10.1121/1.429403. [DOI] [PubMed] [Google Scholar]
- 27.Wagner W, Heppelmann G, Vonthein R, Zenner HP. Test–retest repeatability of distortion product otoacoustic emissions. Ear Hear. 2008;29(3):378–91. doi: 10.1097/AUD.0b013e31816906e7. [DOI] [PubMed] [Google Scholar]
- 28.Reuter K, Ordoñez R, Hammershøi D. Overexposure effects of a 1-kHz tone on the distortion product otoacoustic emission in humans. J Acoust Soc Am. 2007;122(1):378–86. doi: 10.1121/1.2743163. [DOI] [PubMed] [Google Scholar]
- 29.Beattie RC, Kenworthy O, Luna CA. Immediate and short-term reliability of distortion-product otoacoustic emissions: Confiabilidad inmediata ya corto plazo de las emisiones otoacústicas por productos de distorsión. Int J Audiol. 2003;42(6):348–54. doi: 10.3109/14992020309101328. [DOI] [PubMed] [Google Scholar]
- 30.Dreisbach LE, Long KM, Lees SE. Repeatability of high-frequency distortion-product otoacoustic emissions in normal-hearing adults. Ear Hear. 2006;27(5):466–79. doi: 10.1097/01.aud.0000233892.37803.1a. [DOI] [PubMed] [Google Scholar]
- 31.Beattie R, Bleech J. Effects of sample size on the reliability of noise floor and DPOAE. Br J Audiol. 2000;34(5):305–9. doi: 10.3109/03005364000000142. [DOI] [PubMed] [Google Scholar]
- 32.Poole KCA, Codling A, Frost G. Optimum test conditions and variability of otoacoustic emission testing in individuals with normal hearing. HSE Books. 2011 (RR840), available from: http://www.hse.gov.uk/research/rrpdf/rr840.pdf. [Google Scholar]
- 33.Uchida Y, Ando F, Shimokata H, Sugiura S, Ueda H, Nakashima T. The effects of aging on distortion-product otoacoustic emissions in adults with normal hearing. Ear Hear. 2008;29(2):176–84. doi: 10.1097/AUD.0b013e3181634eb8. [DOI] [PubMed] [Google Scholar]
- 34.Mehrparvar AH, Mirmohammadi SJ, Davari MH, Mostaghaci M, Mollasadeghi A, Bahaloo M, et al. Conventional audiometry, extended high-frequency audiometry, and DPOAE for early diagnosis of NIHL. Iran Red Crescent Med J. 2014;16(1) doi: 10.5812/ircmj.9628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Baradarnfar MH, Karamifar K, Mehrparvar AH, Mollasadeghi A, Gharavi M, Karimi G, et al. Amplitude changes in otoacoustic emissions after exposure to industrial noise. Noise Health. 2012;14(56):28. doi: 10.4103/1463-1741.93329. [DOI] [PubMed] [Google Scholar]
- 36.Edwards AL, Taela M. Feasibility of screening distortion product otoacoustic emissions to monitor cochlear functioning in noise exposed mine workers. Occupational Health Southern Africa. 2008;14(1):18–21. [Google Scholar]
- 37.Balatsouras D, Homsioglou E, Danielidis V. Extended high-frequency audiometry in patients with acoustic trauma. Clin Otolaryngol. 2005;30(3):249–54. doi: 10.1111/j.1365-2273.2005.00984.x. [DOI] [PubMed] [Google Scholar]
- 38.Büchler M, Kompis M, Hotz MA. Extended frequency range hearing thresholds and otoacoustic emissions in acute acoustic trauma. Otol Neurotol. 2012;33(8):1315–22. doi: 10.1097/MAO.0b013e318263d598. [DOI] [PubMed] [Google Scholar]
- 39.Costa J, de Almeida VF, de Oliveira C, Sampaio A. Transient and distortion product evoked otoacoustic emissions in premature infants. Arq Int Otorrinolaringol. 2009;13:309–16. [Google Scholar]