

Abstract
Background
The cardiovascular safety of inhaled long-acting β2-agonists (LABAs) in patients with chronic obstructive pulmonary disease (COPD) is a controversial problem. Certain studies have suggested that inhaled LABAs lead to an increased risk of cardiovascular events in patients with COPD. This meta-analysis aimed to assess the cardiovascular safety of inhaled LABAs in COPD.
Methods
A meta-analysis of randomized, double-blind, parallel-group, placebo-controlled trials for LABA treatment of COPD with at least 3 months of follow-up was performed. The fixed-effects model was used to evaluate the effects of LABAs on fatal cardiovascular adverse events. Adverse events were collected for each trial, and the relative risk (RR) and 95% confidence intervals (CI) for LABA/placebo were estimated.
Results
There were 24 trials included in this meta-analysis. Compared with placebo, inhaled LABAs significantly decreased fatal cardiovascular adverse events in COPD patients (RR 0.65, 95% CI 0.50 to 0.86, P = 0.002). In sensitivity analysis, there was still no increased risk of fatal cardiovascular events (RR 0.68, 95%CI 0.46 to 1.01, P = 0.06) after excluding the trial with the largest weight. Among the different types of LABAs, only salmeterol had a significant effect (RR 0.64, 95% CI 0.46 to 0.90). In subgroup analyses, inhaled LABAs were able to significantly decrease fatal cardiovascular events in long-term trials (RR 0.64, 95% CI 0.47 to 0.87) and in trials with severe COPD patients (RR 0.69, 95% CI 0.50 to 0.96).
Conclusion
Inhaled LABAs do not increase the risk of fatal cardiovascular events in COPD patients.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common respiratory disorder that leads to high morbidity and mortality. Worldwide, COPD affects 329 million people or nearly 5% of the population [1]. Certain common symptoms of COPD, such as dyspnea, chronic cough, and shortness of breath, reduce the patients’ quality of life and cause a serious economic burden on healthcare resources. Inhaled bronchodilators, including β2-adrenoceptor agonists and anticholinergics, play a significant role in treating COPD. Inhaled β2-adrenoceptor agonists relieve the symptoms of COPD by relaxing the bronchial smooth muscles. Short-acting β2-adrenoceptor agonists (SABAs) are recommended on an as needed basis, whereas long-acting β2-adrenoceptor agonists (LABAs) are recommended as a first-line therapy for controlling the symptoms of COPD. Several meta-analyses have provided evidence that LABAs significantly reduce COPD exacerbations, improve pulmonary function and quality of life and are well tolerated [2–4].
However, COPD is often accompanied by cardiac disorders, and a proportion of the deaths of patients with COPD are the result of cardiovascular complications [5]. It has been reported that reduced FEV1 among COPD patients nearly doubles the risk of cardiovascular mortality, independent of age, sex and cigarette smoking [6].Thus, it is important to evaluate the cardiovascular safety of medications for treating COPD. Given that β2-receptors are also present in the heart, which can cause cardiac toxicity [7], the cardiovascular safety of using inhaled LABAs in COPD patients remains a controversial issue. Certain evidence has showed that inhaled LABAs increase the risk of adverse cardiovascular events [8, 9]. Salpeter et al performed a meta-analysis and found that compared with placebo, inhaled LABAs significantly increased sinus tachycardia, with a non-significant trend toward an increase in major cardiovascular events, including atrial fibrillation, congestive heart failure and myocardial infarction [8]. In contrast, Ferguson et al [10] analyzed seven placebo-controlled trials and provided evidence that there was no significant difference between salmeterol (a type of LABA) and placebo in terms of cardiovascular events and deaths. Moreover, a large double-blind, parallel-group, placebo-controlled trial with a 3-year follow-up, known as the TORCH study, found no significant difference between salmeterol and placebo with respect to cardiovascular complications [11]. Considering the evidence mentioned above, it is still uncertain whether inhaled LABAs can increase cardiovascular events and death in COPD patients. Moreover, certain new once-daily LABAs, such as indacaterol, olodaterol and vilanterol, have recently shown efficacy in improving COPD symptoms and reducing exacerbations [12–18], but the influence of these new agents on cardiovascular events is unknown. Therefore, we conducted this meta-analysis to determine the effect of inhaled LABAs compared with placebo on fatal cardiovascular events in COPD patients.
Methods
Eligibility criteria
The inclusion criteria for trials were as follows: (1) the study was a randomized controlled trial(RCT) with a double-blind, parallel-group, placebo-controlled design and more than 3 months of follow-up including any inhaled LABA; (2) the study patients had COPD of any severity; (3) the trial provided the details of fatal cardiovascular events and reported at least one such event; (4) trials were excluded if they enrolled patients with asthma, did not compare a LABA with placebo, were only protocols or abstracts, or were written in non-English languages.
Search strategy
We searched MEDLINE, EMBASE, the Cochrane Library and Clinicaltrials.gov for trials. We also examined the bibliographies of related systematic review articles for eligible trials, and two investigators independently reviewed all trials to determine if each study was an RCT and met the inclusion criteria mentioned above. The search strategy was “long acting beta 2 agonist” OR “long acting beta agonist” OR “LABA” OR “adrenergic beta 2 receptor agonists” OR “adrenergic beta agonists” OR “bronchodilator agents” OR “salmeterol” OR “formoterol” OR “olodaterol” OR “vilanterol” OR “indacaterol”, and “chronic obstructive pulmonary disease” OR “chronic obstructive lung disease” OR “chronic obstructive airway disease” OR “pulmonary disease, chronic obstructive” OR “COPD”, based on a previously published meta-analysis [19].
Outcome measures and data extraction
The primary outcomes were fatal cardiovascular adverse events. All events were coded using the Medical Dictionary for Regulatory Activities (MedDRA) [20]. We defined fatal cardiovascular events to include fatal events reported in the trials and three other terms (not coded as cardiovascular events by the MedDRA), which were sudden death, sudden cardiac death and cardiac death, as described in a previous meta-analysis [21]. Two reviewers independently and separately extracted the outcome data, and a third reviewer provided additional insight in the event of a discrepancy. If the primary outcomes were not available in the original articles, we searched for details using Clinicaltrials.gov, the US FDA website, and the manufacturers’ clinical trials registry website. All trials were evaluated using the Jadad scoring system, and a score >2 was required for a trial to be kept in the analysis [22].
Statistical analysis
Review Manager (RevMan) version 5.0 was used to calculate the relative risk (RR) and 95% confidence intervals (CIs) for the primary outcomes. A two-sided α value of 0.05 was defined as statistically significant. Statistical heterogeneity was addressed using the Cochrane Q test, and the magnitude of heterogeneity was estimated by I2 statistic [23], where a value more than 50% indicates a substantial level of heterogeneity. We used the fixed-effects model to pool data if substantial statistical heterogeneity was not present. Visual inspection of funnel plots was used to assess the presence of publication bias.
Subgroup analyses were carried out with the data segregated by the different types of inhaled LABAs, the study duration (≤6 months vs. >6 months), and the severity of COPD (FEV1>50% vs. FEV1≤50%). Sensitivity analysis was performed to evaluate the influence of individual studies on the summary effect by looking at the influence of each study and then repeating the analysis after excluding the study with the largest weight.
Results
Characteristics of the identified studies
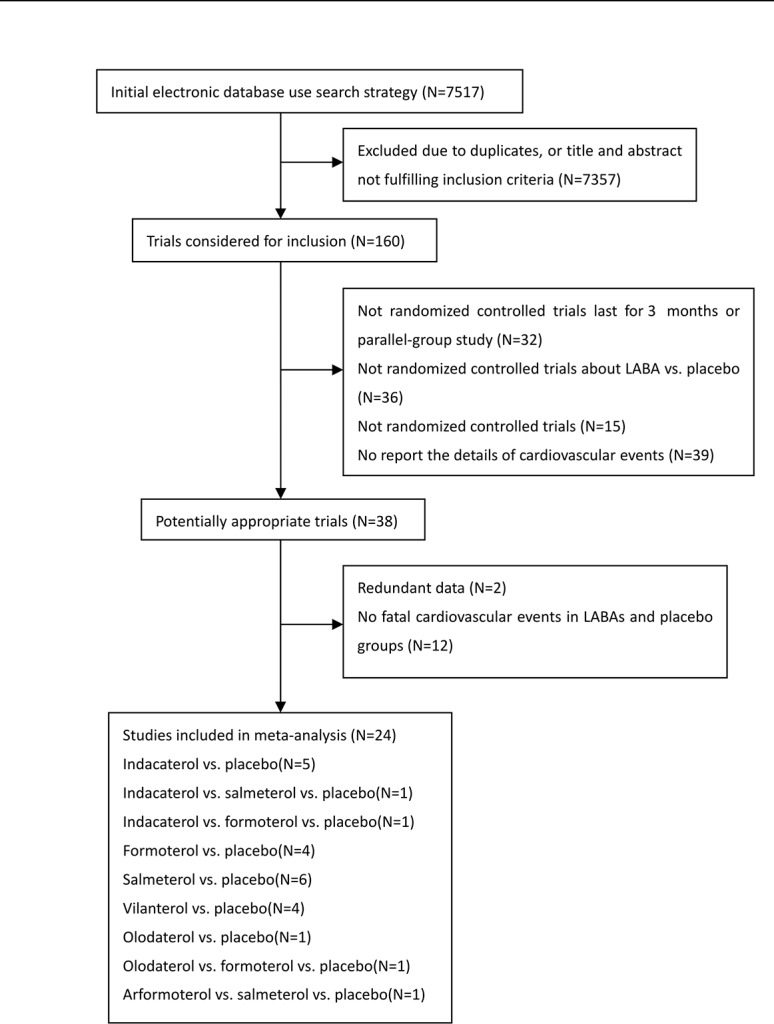
After a detailed review of 160 studies, a total of 24 trials that fulfilled the inclusion criteria were selected for the meta-analysis [11, 12, 14–18, 24–40]. The details of the trial selection strategy are shown in Fig 1, and the main characteristics of the included trials are shown in S1 Table. All trials were of good quality (Jadad score >2). In the 24 trials, a total of 12,291 patients received an inhaled LABA, and 7784 received placebo therapy. The mean age of the participants was more than 60 years in all of these trials. There were 8 long-term trials (longer than 6 months), and 16 short-term trials (12 to 26 weeks). The mean predicted FEV1 of the participants was more than 50% in 10 trials and less than 50% in 12 trials; 2 trials did not report the details of FEV1.
Fig 1. Flowchart of study identification.
Meta-analysis
In total, 24 studies reported at least one fatal cardiovascular event. Compared with placebo, the inhaled LABAs significantly decreased the risk of fatal cardiovascular events in COPD (RR 0.65, 95% CI 0.50 to 0.86, P = 0.002, Fig 2) with no evidence of statistical heterogeneity (I2 = 0%, P = 1.00).
Fig 2. Meta-analysis of fatal cardiovascular events in RCTs of LABAs compare with placebo.

Subgroup analyses
The results for the impact of different inhaled LABAs on fatal cardiovascular events are shown in Table 1. Moreover, there was a significant difference between the long-term and short-term trials. In the 8 long-term trials, LABAs significantly decreased the risk of fatal cardiovascular events compared with placebo (RR 0.64, 95% CI 0.47 to 0.87, P = 0.004, Fig 3), without obvious heterogeneity (I2 = 0%, P = 0.70). However, there was no significant difference between inhaled LABAs and placebo in terms of fatal cardiovascular events in the short-term trials (RR 0.78, 95% CI 0.40 to 1.50, P = 0.45, Fig 4). Furthermore, compared with placebo, LABAs significantly decreased the risk of fatal cardiovascular events in the trials in which the predicted FEV1 of the participants were less than 50% (RR 0.69, 95% CI 0.50 to 0.96, Fig 5). In contrast, there was no significant difference between inhaled LABAs and placebo in terms of fatal events in the trials in which the predicted FEV1 of participants were more than 50% (RR 0.62, 95% CI 0.32 to 1.23, Fig 6).
Table 1. Results of Meta-analysis of different inhaled LABAs on fatal cardiovascular events.
| LABAs | No. of RCTs | No./Total No. | RR (95%CI) | P Value | I2,%a | |
|---|---|---|---|---|---|---|
| LABA | Controls | |||||
| Salmeterol | 7 | 53/3313 | 83/3294 | 0.64(0.46,0.90) | 0.01 | 0 |
| Formoterol | 7 | 12/2392 | 12/1814 | 0.84(0.39,1.84) | 0.67 | 0 |
| Indacaterol | 7 | 7/3164 | 8/1906 | 0.56(0.22,1.42) | 0.22 | 0 |
| Vilanterol | 4 | 5/1233 | 4/969 | 1.05(0.30,3.68) | 0.94 | 0 |
| Olodaterol | 4 | 8/1759 | 9/885 | 0.45(0.19,1.11) | 0.08 | 0 |
| Aformoterol | 1 | 1/430 | 0/143 | 1.00(0.04,24.47) | 1.00 | NA |
Abbreviations: CI, confidence interval; RCT, randomized controlled trials; RR, relative risk
Fig 3. Meta-analysis of fatal cardiovascular events in long-term RCTs of LABAs compared with placebo.

Fig 4. Meta-analysis of fatal cardiovascular events in short-term RCTs of LABAs compared with placebo.

Fig 5. Meta-analysis of fatal cardiovascular events in RCTs (FEV1<50%) of LABAs compared with placebo.

Fig 6. Meta-analysis of fatal cardiovascular events in RCTs (FEV1≥50%) of LABAs compared with placebo.

Sensitivity analysis and publication bias
We performed the leave-one-out sensitivity analysis by removing one study per time to check whether individual study influenced the results. After excluding the trial that contributed to more than 50% of the weight in the fixed-effects model (with the largest sample size and the longest duration of follow-up) [11], the analysis of the remaining 23 trials on the primary outcome of fatal cardiovascular events yielded effect sizes (RR 0.68, 95% CI 0.46 to 1.01, P = 0.06), which still did not increase the risk of fatal cardiovascular events. There was no evidence of statistical heterogeneity among the trials (I2 = 0%). Moreover, we used the funnel plot to assess the publication bias. The funnel plot was symmetrical, and no publication bias was found (Fig 7).
Fig 7. Funnel plot for studies reporting fatal cardiovascular events in COPD patients.

Discussion
Based on the results of our meta-analysis of 24 clinical trials, inhaled LABAs significantly reduced the rate of fatal cardiovascular events in COPD patients compared with placebo (RR 0.65, 95% CI 0.50 to 0.86, P = 0.002). Moreover, the subgroup analyses showed that inhaled LABAs were able to significantly decrease fatal cardiovascular events in long-term trials and in studies with severe COPD patients (study duration >6 months and predicted FEV1 ≤50%).
There are certain potential mechanisms underlying the benefits of LABA treatment in terms of cardiovascular events. First, from a clinical perspective, it is known that COPD is an important cause of death and is closely related to cardiovascular morbidity and mortality [41]. There is certain evidence that recurrent COPD exacerbations, impairment of lung function, and respiratory failure are risk factors for fatal cardiovascular events, including malignant arrhythmia, ischemic heart disease, myocardial infarction and stroke [42–44]. In this context, it is important that the strategy for the treatment of COPD includes approaches to improve lung function and to reduce the frequency of exacerbations because these approaches can decrease cardiovascular morbidity and mortality. Numerous clinical trials have shown that inhaled LABAs significantly improve lung function and decrease the rate of COPD exacerbations compared with placebo, which might explain the observed outcome of favorable effects of LABAs. This finding also supported the results of the subgroup analyses. In long-term trials, the longer that inhaled LABAs were used, the more lung function improved. Therefore, the incidence of cardiovascular events decreased more significantly than in short-term trials. Moreover, as mentioned above, impairment of lung function was a risk factor for cardiovascular events in COPD patients. In trials with severe COPD patients (predicted FEV1≤50%), the rate of cardiovascular events was much higher than in trials with non-severe COPD patients (predicted FEV1>50%). Therefore, compared with placebo, the effect of inhaled LABAs on reducing cardiovascular events was more significant in trials with severe COPD patients. Second, with respect to biological mechanisms, it is known that there are three different types of β-receptors in humans. The heart expresses primarily β1-receptors and presents a relatively small proportion of β2-receptors. Most β2-receptors are present in human airway smooth muscle. All of the inhaled LABAs tested in the trials described here are highly selective β2-receptor agonists that mainly relax bronchial smooth muscle to improve lung function, dyspnea, hypoxia and exercise tolerance but have little direct impact on the heart. There is certain evidence that hypoxia, physical inactivity and oxidative stress increase sympathetic activity in patients with COPD [45]. Inhaled LABAs significantly reduce hypoxia and improve exercise tolerance, which down-regulate sympathetic activity, resulting in a reduction in myocardial oxygen consumption and cardiovascular events. Furthermore, certain studies have shown that the development of COPD is closely related to certain inflammatory cytokines. Compared with control subjects, the levels of TNF-α and IL-8 are elevated in the sputum of patients with COPD [46]. Moreover, patients with frequent exacerbations have higher levels of stable airway inflammatory markers, including the serum levels of IL-6 and IL-8 [47]. There is certain evidence that high levels of IL-8 and TNF-α increase the risk of cardiovascular events [48–50]. Inhaled LABAs can significantly suppress the release of IL-8 and TNF-α [51], which might be a mechanism for the reduction in cardiovascular events in patients with COPD.
In our meta-analysis, the sensitivity analysis showed that the benefit of inhaled LABAs was largely driven by the result of Calverley and colleagues [11], which contributed nearly 50% of the weight in the fixed-effects model. This may have been because this study enrolled the maximum number of COPD patients and lasted for 3 years, which allowed the researchers to assess the impact of inhaled LABAs on fatal cardiovascular events more accurately compared with other studies. However, there was still no increased risk of fatal cardiovascular events (RR 0.68, 95%CI 0.46 to 1.01, P = 0.06) after excluding this study. The impact of inhaled LABAs on fatal cardiovascular events in COPD patients still needs to be further confirmed by more long-term clinical trials.
There are certain discrepancies between the outcome of our meta-analysis and the results of previous studies. Based on observational studies, Gershon et al [52] and Au et al [53] reported that the use of inhaled LABAs was associated with a higher risk of cardiovascular events compared with not using these medications. Furthermore, an analysis conducted by Salpeter et al selected 13 single-dose and 20 longer-duration randomized, placebo-controlled trials to evaluate the cardiovascular effects of β2 agonists in patients with COPD and asthma [8]. The authors defined cardiovascular events as including sinus and ventricular tachycardia, syncope, atrial fibrillation, congestive heart failure, myocardial infarction, cardiac arrest and sudden death and estimated the effects of sinus tachycardia separately from those of the other events in the longer-duration trials. In the included trials, which lasted from 3 days to 1 year, β2 agonists increased the risk of cardiovascular events (RR 2.54, 95% CI 1.59 to 4.05), but when sinus tachycardia was excluded, there were no significant differences in major cardiovascular events (RR 1.66, 95% CI 0.76 to 3.60). There were certain limitations to this analysis. First, the clinical significance of this analysis with respect to the cardiovascular effects of inhaled LABAs on COPD is unclear because the analysis included trials that involved asthma patients and because only six longer trials of LABAs in COPD were included. Second, the authors only found a significant difference between β2 agonists and placebo for sinus tachycardia, which is considered to be a minor event. In contrast, we focused our attention on fatal cardiovascular events, which are more meaningful for clinical practice. Third, in the prior analysis, approximately one-half of adverse cardiac events occurred in a single trial of SABA use in asthma, which may have led to inaccurate outcomes regarding the effects of LABAs in COPD patients.
The results of our analysis are consistent with other published studies showing that inhaled LABAs have a beneficial effect on cardiovascular events in COPD patients. One retrospective case-control study found that inhaled LABAs decreased all-cause mortality in COPD (OR 0.92, 95% CI 0.88 to 0.96) and that there was a trend toward a benefit in terms of cardiovascular deaths (OR 0.97, 95% CI 0.84 to 1.11), although this effect did not reach statistical significance [54]. Furthermore, Ferguson et al[10] conducted a meta-analysis of seven trials assessing the cardiovascular safety of salmeterol and showed no increase in the risk of cardiovascular events compared with placebo (RR 1.03, 95% CI 0.8 to 1.3). Both groups had a similar incidence of cardiovascular events, including fatal events. Moreover, in addition to certain retrospective studies, several RCTs support our results [11, 55, 56], although two of these did not meet the inclusion criteria and were excluded from our meta-analysis [55, 56]. Campbell et al [55] compared formoterol with placebo for 8 weeks and found no significant differences between the two groups in terms of heart rate, ventricular premature beats, ventricular tachycardia events or supraventricular premature beats. Similarly, Nelson et al[56]estimated cardiac safety in a 12-week, multicenter, randomized, double-blind, placebo-controlled trial with formoterol. Compared with placebo, the occurrence of treatment-emergent adverse cardiac events was similar in the formoterol group, and no deaths or serious cardiac adverse events occurred during the treatment period. Furthermore, a new once-daily LABA, known as indacaterol, was recently shown to be efficient in treating COPD patients. A secondary analysis of three clinical trials provided evidence that indacaterol did not increase the risk of cardiovascular or cerebrovascular adverse events at any dose (RR 1.35, 95% CI 0.94 to 1.92) [57].
There are certain limitations to our study that make it difficult to achieve definitive conclusions. First, as with any meta-analysis, the potential for publication bias needs to be discussed. However, visual inspection of funnel plots suggested that publication bias was unlikely in this meta-analysis. Second, none of the included trials were specifically designed to monitor the risk of cardiovascular events, which might have resulted in incomplete reporting of cardiovascular events. Third, the data used in this analysis were based on the judgment of the investigators, which might result in discrepant reports between studies. Fourth, in our meta-analysis, the sensitivity analysis showed that the benefit of inhaled LABAs was largely driven by one study [11], which contributed nearly 50% of the weight in the fixed-effects model. This finding indicated that more studies with larger samples and longer durations will be needed to evaluate the association between LABAs and cardiovascular events. Finally, because of the low number of clinical trials examined, the results derived from the subgroup analyses should be interpreted with considerable caution. Despite these limitations, we believe that this analysis adds more positive evidence for the cardiovascular safety of inhaled LABA use in patients with COPD.
Conclusions
In summary, despite certain limitations, our findings still have potential implications. We performed a meta-analysis of 24 RCTs, and the outcome indicates that inhaled LABAs do not increase the risk of fatal cardiovascular events in COPD, which was especially noted in long-term trials with severe COPD patients. Therefore, it is safe to use LABAs in COPD patients who have comorbidities consisting of cardiovascular diseases.
Supporting Information
(DOC)
(DOCX)
(DOCX)
Acknowledgments
We thank American Journal Experts (AJE) for English language editing.
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
The authors received no specific funding for this work.
References
- 1. Stenger VG, Maren TH. The pharmacology of MS 222 (ethyl-m-aminobenzoate) in Squalus acanthias. Comparative and general pharmacology. 1974;5(1):23–35. . [DOI] [PubMed] [Google Scholar]
- 2. Decramer ML, Hanania NA, Lotvall JO, Yawn BP. The safety of long-acting beta2-agonists in the treatment of stable chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2013;8:53–64. 10.2147/COPD.S39018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Rodrigo GJ, Nannini LJ, Rodriguez-Roisin R. Safety of long-acting beta-agonists in stable COPD: a systematic review. Chest. 2008;133(5):1079–87. 10.1378/chest.07-1167 . [DOI] [PubMed] [Google Scholar]
- 4. Kew KM, Dias S, Cates CJ. Long-acting inhaled therapy (beta-agonists, anticholinergics and steroids) for COPD: a network meta-analysis. The Cochrane database of systematic reviews. 2014;3:CD010844 10.1002/14651858.CD010844.pub2 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Boschetto P, Beghe B, Fabbri LM, Ceconi C. Link between chronic obstructive pulmonary disease and coronary artery disease: implication for clinical practice. Respirology. 2012;17(3):422–31. 10.1111/j.1440-1843.2011.02118.x . [DOI] [PubMed] [Google Scholar]
- 6. Sin DD, Wu L, Man SF. The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest. 2005;127(6):1952–9. 10.1378/chest.127.6.1952 . [DOI] [PubMed] [Google Scholar]
- 7. Bristow MR. beta-adrenergic receptor blockade in chronic heart failure. Circulation. 2000;101(5):558–69. . [DOI] [PubMed] [Google Scholar]
- 8. Salpeter SR, Ormiston TM, Salpeter EE. Cardiovascular effects of beta-agonists in patients with asthma and COPD: a meta-analysis. Chest. 2004;125(6):2309–21. . [DOI] [PubMed] [Google Scholar]
- 9. Cazzola M, Matera MG, Donner CF. Inhaled β2-Adrenoceptor Agonists Cardiovascular Safety in Patients with Obstructive Lung Disease. Drugs. 2005;65(12):1595–610. [DOI] [PubMed] [Google Scholar]
- 10. Ferguson GT, Funck-Brentano C, Fischer T, Darken P, Reisner C. Cardiovascular safety of salmeterol in COPD. Chest. 2003;123(6):1817–24. . [DOI] [PubMed] [Google Scholar]
- 11. Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–89. 10.1056/NEJMoa063070 . [DOI] [PubMed] [Google Scholar]
- 12. Kornmann O, Dahl R, Centanni S, Dogra A, Owen R, Lassen C, et al. Once-daily indacaterol versus twice-daily salmeterol for COPD: a placebo-controlled comparison. Eur Respir J. 2011;37(2):273–9. 10.1183/09031936.00045810 . [DOI] [PubMed] [Google Scholar]
- 13. Kinoshita M, Lee SH, Hang LW, Ichinose M, Hosoe M, Okino N, et al. Efficacy and safety of indacaterol 150 and 300 microg in chronic obstructive pulmonary disease patients from six Asian areas including Japan: a 12-week, placebo-controlled study. Respirology. 2012;17(2):379–89. 10.1111/j.1440-1843.2011.02107.x . [DOI] [PubMed] [Google Scholar]
- 14. Donohue JF, Fogarty C, Lotvall J, Mahler DA, Worth H, Yorgancioglu A, et al. Once-daily bronchodilators for chronic obstructive pulmonary disease: indacaterol versus tiotropium. Am J Respir Crit Care Med. 2010;182(2):155–62. 10.1164/rccm.200910-1500OC . [DOI] [PubMed] [Google Scholar]
- 15. Martinez FJ, Boscia J, Feldman G, Scott-Wilson C, Kilbride S, Fabbri L, et al. Fluticasone furoate/vilanterol (100/25; 200/25 mug) improves lung function in COPD: a randomised trial. Respir Med. 2013;107(4):550–9. 10.1016/j.rmed.2012.12.016 . [DOI] [PubMed] [Google Scholar]
- 16. Kerwin EM, Scott-Wilson C, Sanford L, Rennard S, Agusti A, Barnes N, et al. A randomised trial of fluticasone furoate/vilanterol (50/25 mug; 100/25 mug) on lung function in COPD. Respir Med. 2013;107(4):560–9. 10.1016/j.rmed.2012.12.014 . [DOI] [PubMed] [Google Scholar]
- 17. Ferguson GT, Feldman GJ, Hofbauer P, Hamilton A, Allen L, Korducki L, et al. Efficacy and safety of olodaterol once daily delivered via Respimat(R) in patients with GOLD 2–4 COPD: results from two replicate 48-week studies. Int J Chron Obstruct Pulmon Dis. 2014;9:629–45. 10.2147/COPD.S61717 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Koch A, Pizzichini E, Hamilton A, Hart L, Korducki L, De Salvo MC, et al. Lung function efficacy and symptomatic benefit of olodaterol once daily delivered via Respimat(R) versus placebo and formoterol twice daily in patients with GOLD 2–4 COPD: results from two replicate 48-week studies. Int J Chron Obstruct Pulmon Dis. 2014;9:697–714. 10.2147/COPD.S62502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Dong YH, Lin HH, Shau WY, Wu YC, Chang CH, Lai MS. Comparative safety of inhaled medications in patients with chronic obstructive pulmonary disease: systematic review and mixed treatment comparison meta-analysis of randomised controlled trials. Thorax. 2013;68(1):48–56. 10.1136/thoraxjnl-2012-201926 . [DOI] [PubMed] [Google Scholar]
- 20. Celli B, Decramer M, Leimer I, Vogel U, Kesten S, Tashkin DP. Cardiovascular safety of tiotropium in patients with COPD. Chest. 2010;137(1):20–30. 10.1378/chest.09-0011 . [DOI] [PubMed] [Google Scholar]
- 21. Singh S, Loke YK, Furberg CD. Inhaled anticholinergics and risk of major adverse cardiovascular events in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300(12):1439–50. 10.1001/jama.300.12.1439 . [DOI] [PubMed] [Google Scholar]
- 22. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled clinical trials. 1996;17(1):1–12. . [DOI] [PubMed] [Google Scholar]
- 23. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. 2003;327(7414):557–60. 10.1136/bmj.327.7414.557 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Bogdan MA, Aizawa H, Fukuchi Y, Mishima M, Nishimura M, Ichinose M. Efficacy and safety of inhaled formoterol 4.5 and 9 mug twice daily in Japanese and European COPD patients: phase III study results. BMC Pulm Med. 2011;11:51 10.1186/1471-2466-11-51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Tashkin DP, Rennard SI, Martin P, Ramachandran S, Martin UJ, Silkoff PE, et al. Efficacy and safety of budesonide and formoterol in one pressurized metered-dose inhaler in patients with moderate to very severe chronic obstructive pulmonary disease: results of a 6-month randomized clinical trial. Drugs. 2008;68(14):1975–2000. . [DOI] [PubMed] [Google Scholar]
- 26. Donohue JF, Maleki-Yazdi MR, Kilbride S, Mehta R, Kalberg C, Church A. Efficacy and safety of once-daily umeclidinium/vilanterol 62.5/25 mcg in COPD. Respir Med. 2013;107(10):1538–46. 10.1016/j.rmed.2013.06.001 . [DOI] [PubMed] [Google Scholar]
- 27. Bateman ED, Ferguson GT, Barnes N, Gallagher N, Green Y, Henley M, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42(6):1484–94. 10.1183/09031936.00200212 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Singh D, Jones PW, Bateman ED, Korn S, Serra C, Molins E, et al. Efficacy and safety of aclidinium bromide/formoterol fumarate fixed-dose combinations compared with individual components and placebo in patients with COPD (ACLIFORM-COPD): a multicentre, randomised study. BMC Pulm Med. 2014;14:178 10.1186/1471-2466-14-178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Feldman G, Siler T, Prasad N, Jack D, Piggott S, Owen R, et al. Efficacy and safety of indacaterol 150 microg once-daily in COPD: a double-blind, randomised, 12-week study. BMC Pulm Med. 2010;10:11 10.1186/1471-2466-10-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Kerwin EM, Gotfried MH, Lawrence D, Lassen C, Kramer B. Efficacy and tolerability of indacaterol 75 mug once daily in patients aged >/ = 40 years with chronic obstructive pulmonary disease: results from 2 double-blind, placebo-controlled 12-week studies. Clin Ther. 2011;33(12):1974–84. 10.1016/j.clinthera.2011.11.009 . [DOI] [PubMed] [Google Scholar]
- 31. Dahl R, Chung KF, Buhl R, Magnussen H, Nonikov V, Jack D, et al. Efficacy of a new once-daily long-acting inhaled beta2-agonist indacaterol versus twice-daily formoterol in COPD. Thorax. 2010;65(6):473–9. 10.1136/thx.2009.125435 . [DOI] [PubMed] [Google Scholar]
- 32. Chapman KR, Rennard SI, Dogra A, Owen R, Lassen C, Kramer B, et al. Long-term safety and efficacy of indacaterol, a long-acting beta(2)-agonist, in subjects with COPD: a randomized, placebo-controlled study. Chest. 2011;140(1):68–75. 10.1378/chest.10-1830 . [DOI] [PubMed] [Google Scholar]
- 33. Calverley P, Pauwels R, Vestbo J, Jones P, Pride N, Gulsvik A, et al. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trial. The Lancet. 2003;361(9356):449–56. 10.1016/s0140-6736(03)12459-2 [DOI] [PubMed] [Google Scholar]
- 34. Stockley RA, Chopra N, Rice L. Addition of salmeterol to existing treatment in patients with COPD: a 12 month study. Thorax. 2006;61(2):122–8. 10.1136/thx.2004.033266 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Baumgartner RA, Hanania NA, Calhoun WJ, Sahn SA, Sciarappa K, Hanrahan JP. Nebulized arformoterol in patients with COPD: a 12-week, multicenter, randomized, double-blind, double-dummy, placebo- and active-controlled trial. Clin Ther. 2007;29(2):261–78. 10.1016/j.clinthera.2007.02.009 . [DOI] [PubMed] [Google Scholar]
- 36. Rossi A, Kristufek P, Levine BE, Thomson MH, Till D, Kottakis J, et al. Comparison of the efficacy, tolerability, and safety of formoterol dry powder and oral, slow-release theophylline in the treatment of COPD. Chest. 2002;121(4):1058–69. . [DOI] [PubMed] [Google Scholar]
- 37. Donohue JF, van Noord JA, Bateman ED, Langley SJ, Lee A, Witek TJ Jr., et al. A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest. 2002;122(1):47–55. . [DOI] [PubMed] [Google Scholar]
- 38. Brusasco V, Hodder R, Miravitlles M, Korducki L, Towse L, Kesten S. Health outcomes following treatment for six months with once daily tiotropium compared with twice daily salmeterol in patients with COPD. Thorax. 2003;58(5):399–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Rennard SI, Anderson W, ZuWallack R, Broughton J, Bailey W, Friedman M, et al. Use of a long-acting inhaled beta2-adrenergic agonist, salmeterol xinafoate, in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;163(5):1087–92. 10.1164/ajrccm.163.5.9903053 . [DOI] [PubMed] [Google Scholar]
- 40. Celli B, Crater G, Kilbride S, Mehta R, Tabberer M, Kalberg CJ, et al. Once-daily umeclidinium/vilanterol 125/25 mcg in COPD: a randomized, controlled study. Chest. 2014. 10.1378/chest.13-1579 . [DOI] [PubMed] [Google Scholar]
- 41. Sidney S, Sorel M, Quesenberry CP Jr., DeLuise C, Lanes S, Eisner MD. COPD and incident cardiovascular disease hospitalizations and mortality: Kaiser Permanente Medical Care Program. Chest. 2005;128(4):2068–75. 10.1378/chest.128.4.2068 . [DOI] [PubMed] [Google Scholar]
- 42. Shih HT, Webb CR, Conway WA, Peterson E, Tilley B, Goldstein S. Frequency and significance of cardiac arrhythmias in chronic obstructive lung disease. Chest. 1988;94(1):44–8. . [DOI] [PubMed] [Google Scholar]
- 43. Johnston AK, Mannino DM, Hagan GW, Davis KJ, Kiri VA. Relationship between lung function impairment and incidence or recurrence of cardiovascular events in a middle-aged cohort. Thorax. 2008;63(7):599–605. 10.1136/thx.2007.088112 . [DOI] [PubMed] [Google Scholar]
- 44. Donaldson GC, Hurst JR, Smith CJ, Hubbard RB, Wedzicha JA. Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest. 2010;137(5):1091–7. 10.1378/chest.09-2029 . [DOI] [PubMed] [Google Scholar]
- 45. van Gestel AJ, Kohler M, Clarenbach CF. Sympathetic overactivity and cardiovascular disease in patients with chronic obstructive pulmonary disease (COPD). Discovery medicine. 2012;14(79):359–68. . [PubMed] [Google Scholar]
- 46. Keatings VM, Collins PD, Scott DM, Barnes PJ. Differences in interleukin-8 and tumor necrosis factor-alpha in induced sputum from patients with chronic obstructive pulmonary disease or asthma. Am J Respir Crit Care Med. 1996;153(2):530–4. 10.1164/ajrccm.153.2.8564092 . [DOI] [PubMed] [Google Scholar]
- 47. Bhowmik A, Seemungal TA, Sapsford RJ, Wedzicha JA. Relation of sputum inflammatory markers to symptoms and lung function changes in COPD exacerbations. Thorax. 2000;55(2):114–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Boekholdt SM, Peters RJ, Hack CE, Day NE, Luben R, Bingham SA, et al. IL-8 plasma concentrations and the risk of future coronary artery disease in apparently healthy men and women: the EPIC-Norfolk prospective population study. Arteriosclerosis, thrombosis, and vascular biology. 2004;24(8):1503–8. 10.1161/01.ATV.0000134294.54422.2e . [DOI] [PubMed] [Google Scholar]
- 49. Vaddi K, Nicolini FA, Mehta P, Mehta JL. Increased secretion of tumor necrosis factor-alpha and interferon-gamma by mononuclear leukocytes in patients with ischemic heart disease. Relevance in superoxide anion generation. Circulation. 1994;90(2):694–9. . [DOI] [PubMed] [Google Scholar]
- 50. Ridker PM, Rifai N, Pfeffer M, Sacks F, Lepage S, Braunwald E. Elevation of tumor necrosis factor-alpha and increased risk of recurrent coronary events after myocardial infarction. Circulation. 2000;101(18):2149–53. . [DOI] [PubMed] [Google Scholar]
- 51. Donnelly LE, Tudhope SJ, Fenwick PS, Barnes PJ. Effects of formoterol and salmeterol on cytokine release from monocyte-derived macrophages. Eur Respir J. 2010;36(1):178–86. 10.1183/09031936.00158008 . [DOI] [PubMed] [Google Scholar]
- 52. Gershon A, Croxford R, Calzavara A, To T, Stanbrook MB, Upshur R, et al. Cardiovascular safety of inhaled long-acting bronchodilators in individuals with chronic obstructive pulmonary disease. JAMA internal medicine. 2013;173(13):1175–85. 10.1001/jamainternmed.2013.1016 . [DOI] [PubMed] [Google Scholar]
- 53. Au DH, Curtis JR, Every NR, McDonell MB, Fihn SD. Association between inhaled beta-agonists and the risk of unstable angina and myocardial infarction. Chest. 2002;121(3):846–51. . [DOI] [PubMed] [Google Scholar]
- 54. Lee TA, Pickard AS, Au DH, Bartle B, Weiss KB. Risk for death associated with medications for recently diagnosed chronic obstructive pulmonary disease. Ann Intern Med. 2008;149(6):380–90. . [DOI] [PubMed] [Google Scholar]
- 55. Campbell SC, Criner GJ, Levine BE, Simon SJ, Smith JS, Orevillo CJ, et al. Cardiac safety of formoterol 12 microg twice daily in patients with chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2007;20(5):571–9. 10.1016/j.pupt.2006.06.003 . [DOI] [PubMed] [Google Scholar]
- 56. Nelson HS, Gross NJ, Levine B, Kerwin EM, Rinehart M, Denis-Mize K, et al. Cardiac safety profile of nebulized formoterol in adults with COPD: a 12-week, multicenter, randomized, double- blind, double-dummy, placebo- and active-controlled trial. Clin Ther. 2007;29(10):2167–78. 10.1016/j.clinthera.2007.10.007 . [DOI] [PubMed] [Google Scholar]
- 57. Worth H, Chung KF, Felser JM, Hu H, Rueegg P. Cardio- and cerebrovascular safety of indacaterol vs formoterol, salmeterol, tiotropium and placebo in COPD. Respir Med. 2011;105(4):571–9. 10.1016/j.rmed.2010.11.027 . [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOC)
(DOCX)
(DOCX)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.