

Abstract
AIM: To assess the effectiveness of and complications associated with metallic stent placement for treatment of anastomotic colonic strictures.
METHODS: A 46-year-old man underging two procedures of surgery for perforation of descending colon due to a traffic accident presented with pain, abdominal distention, and inability to defecate. Single-contrast barium enema radiograph showed a severe stenosis in the region of surgical anastomosis and the patient was too weak to accept another laparotomy. Under fluoroscopic and endoscopic guidance, we placed two metallic stents in the stenosis site of the anastomosis of the patient with anastomotic colonic strictures.
RESULTS: In this case of postsurgical stenosis, the first stent relieved the symptoms of obstruction, but stent migration happened on the next day so an additional stent was required to deal with the stricture and relieve the symptoms.
CONCLUSION: This case confirms that metallic stenting may represent an effective treatment for anastomotic colonic strictures in the absence of other therapeutic alternatives.
INTRODUCTION
Self-expandable metallic stent treatment for colorectal diseases was falling behind that for other organs. Recently, however, there have been many reports on the use of self-expanding metallic stents in colorectal diseases, mainly from the West. Self-expanding metallic stent is generally used as a palliative treatment for malignant strictures of the colon and rectum and before bridge as a surgery for obstructing colorectal cancers[1-3]. Some investigators have reported on the usefulness of self-expanding metallic stents for strictures of benign diseases[4,5]. Management of narrow ( < 5-mm) colonic anastomotic stricture mainly is performed endoscopically by repeated balloon dilation, often ineffectively[6]. The use of metallic self- expanding stents in malignant and benign strictures of the large bowel has been suggested only recently, and is still being debated[7,8]. In this report we proposed a single-stage procedure that we developed to manage narrow anastomotic colonic strictures.
CASE REPORT
A 46-year-old man underging two procedures of surgery for perforation of descending colon due to a traffic accident presented with pain, abdominal distention, and inability to defecate. Single-contrast barium enema radiograph showed a severe stenosis in the region of surgical anastomosis. The patient was too weak to accept another laparotomy. He reached us with a significant stricture of the descending colon anastomoses (smaller than 5 mm in diameter).
With the patient in supine position and two knee joints reflexing, a catheter was inserted over a hydrophilic guide-wire through the anus to the lesion targeted under fluoroscopic and endoscopic guidance. An 85-cm 6-F catheter (Cook) and a 180-cm 0.35-inch guide wire (Bard) were used. The guide wire was maneuvered passing the stricture and the catheter was advanced. This guide wire was then replaced with another guide wire (Amplatz super stiff Guide Wire) for stent delivery and insertion. The stent was then positioned precisely across the lesion and released. The symptoms were released immediately, but on the next day the patient manifested abdominal distention, and inability to defecate. Anteroposterior radiographs from a follow-up barium study showed the stent migrated and a second stent was needed. The second stent was deployed with the same stent placement techniques. Radiographs obtained after a water-soluble enema on the day after the second stent deployed showed that the stents expanded to provide an adequate lumen (Figure 1, Figure 2, Figure 3, Figure 4). The first coated stent (Nanjing MicroTech, China) was 12-cm in length, 32-mm in diameter. The second uncoated stent (Nanjing MicroTech, China) was 20-cm in length, 32-mm in diameter. At the time of this writing, ie, 18 mo of follow-up evaluation, the patient could defecate without any difficulty.
Figure 1.
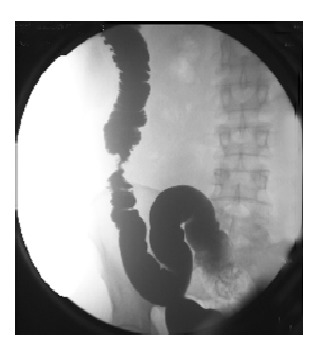
Stenosis at the segment of descending colon, less than 5 mm in diameter.
Figure 2.
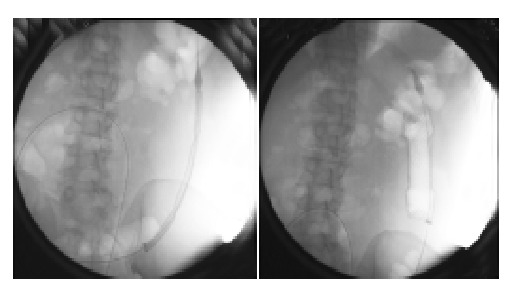
The first stent was appropriately positioned and deployed by withdrawing the enveloping membrane under fluoroscopic control to ensure that the lesion was adequately covered, thus relieving the obstruction.
Figure 3.
Clinical symptoms of obstruction recurred the next day. Anteroposterior radiographs showed the stent migrated above the lesion and a second stent was needed. Second stent was deployed with the same stent placement techniques through the lumen of the first stent.
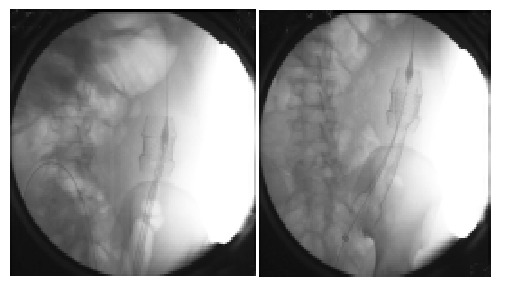
Figure 4.

Radiograph obtained after a water-soluble enema on the day after the second stent was deployed shows that the stents expanded to provide an adequate lumen.
DISCUSSION
Benign postoperative anastomotic strictures are frequent[9]. Several methods of treatment for benign anastomotic strictures after previous resection have been described, including microwave coagulation therapy, balloon and endoscopic bougie dilation, etc[10-14]. Placement of self-expanding metallic stents across narrower anastomotic colonic strictures is a viable alternative to colostomy and, by avoiding emergent surgery, could potentially lower morbidity and mortality[15-17]. The method of stent placement for treatment of benign colonic disorders is the same as that used in cases of malignant strictures, but few experiences with the placement of metallic stents for benign colonic disorders have been reported in the literatures. The indications for stenting were failure to establish dilatation therapy and/or refusal of surgical treatment, in high-risk patients[4-6].
In this case, the patient underwent two times of surgery and he was too weak to accept another surgery. Stenting might represent a therapeutic alternative, in cases of anastomotic strictures of esophageal carcinoma[18,19]. Endoprostheses may have a more lasting dilating effectiveness than balloons or endoscopic bougies, and the ease of recovering the stent when it has fulfilled its purpose could make treatment of the stenosis last for months or years[4-6].
Stent migration may be one of the most complications in treatment of anastomotic strictures. The stent tended to migrate once the stenosis was widened to a diameter at which it could no longer hold the prosthesis in place, and this phenomenon was followed by a recurrence of the clinical symptoms a few days later, which necessitated a series of interventions in these patients. The first stent migration happened and the second stent was needed to be placed in this case[20-22].
We conclude that the application of self-expandable metallic stents in benign stenosis of the gastrointestinal tract may be a possible therapeutic tool in selected patients. Further trials with a greater number of patients dealing with the questions of duration of stay of self-expandable metallic stents and choice of stent type are needed.
Footnotes
Edited by Wang XL Proofread by Zhu LH and Xu FM
References
- 1.Saida Y, Sumiyama Y, Nagao J. [Self-expandable metallic stent in the treatment of colorectal obstruction] Nihon Geka Gakkai Zasshi. 2003;104:554–557. [PubMed] [Google Scholar]
- 2.Mainar A, De Gregorio Ariza MA, Tejero E, Tobío R, Alfonso E, Pinto I, Herrera M, Fernández JA. Acute colorectal obstruction: treatment with self-expandable metallic stents before scheduled surgery--results of a multicenter study. Radiology. 1999;210:65–69. doi: 10.1148/radiology.210.1.r99ja0665. [DOI] [PubMed] [Google Scholar]
- 3.Miyayama S, Matsui O, Kifune K, Yamashiro M, Yamamoto T, Kitagawa K, Kasahara Y, Asada Y, Iida Y, Miura S. Malignant colonic obstruction due to extrinsic tumor: palliative treatment with a self-expanding nitinol stent. AJR Am J Roentgenol. 2000;175:1631–1637. doi: 10.2214/ajr.175.6.1751631. [DOI] [PubMed] [Google Scholar]
- 4.Paúl L, Pinto I, Gómez H, Fernández-Lobato R, Moyano E. Metallic stents in the treatment of benign diseases of the colon: preliminary experience in 10 cases. Radiology. 2002;223:715–722. doi: 10.1148/radiol.2233010866. [DOI] [PubMed] [Google Scholar]
- 5.Dormann AJ, Deppe H, Wigginghaus B. Self-expanding metallic stents for continuous dilatation of benign stenoses in gastrointestinal tract - first results of long-term follow-up in interim stent application in pyloric and colonic obstructions. Z Gastroenterol. 2001;39:957–960. doi: 10.1055/s-2001-18531. [DOI] [PubMed] [Google Scholar]
- 6.Piccinni G, Nacchiero M. Management of narrower anastomotic colonic strictures. Case report and proposal technique. Surg Endosc. 2001;15:1227. doi: 10.1007/s00464-001-4205-y. [DOI] [PubMed] [Google Scholar]
- 7.Morgan R, Adam A. Use of metallic stents and balloons in the esophagus and gastrointestinal tract. J Vasc Interv Radiol. 2001;12:283–297. doi: 10.1016/s1051-0443(07)61906-x. [DOI] [PubMed] [Google Scholar]
- 8.Chevallier P, Baqué P, Benchimol D, Bernard J, Souci J, Chevallier A, Bourgeon A, Padovani B. [Treatement of colorectal obstruction with self-expanding metallic stents under fluoroscopic guidance] J Radiol. 2002;83:473–477. [PubMed] [Google Scholar]
- 9.Schlegel RD, Dehni N, Parc R, Caplin S, Tiret E. Results of reoperations in colorectal anastomotic strictures. Dis Colon Rectum. 2001;44:1464–1468. doi: 10.1007/BF02234598. [DOI] [PubMed] [Google Scholar]
- 10.Takeuchi K, Tsuzuki Y, Ando T, Sekihara M, Hara T, Kori T, Nakajima H, Asao T, Kuwano H. Usefulness of flexible colonoscopic microwave coagulation therapy for a colorectal anastomotic stricture. Dis Colon Rectum. 2003;46:1430–1435. doi: 10.1007/s10350-004-6764-1. [DOI] [PubMed] [Google Scholar]
- 11.Luck A, Chapuis P, Sinclair G, Hood J. Endoscopic laser stricturotomy and balloon dilatation for benign colorectal strictures. ANZ J Surg. 2001;71:594–597. doi: 10.1046/j.1445-2197.2001.02207.x. [DOI] [PubMed] [Google Scholar]
- 12.Chia YW, Ngoi SS, Tung KH. Use of the optical urethrotome knife in the treatment of a benign low rectal anastomotic stricture. Dis Colon Rectum. 1991;34:717–719. doi: 10.1007/BF02050358. [DOI] [PubMed] [Google Scholar]
- 13.Araki Y, Kishimoto Y, Sato Y, Torigoe S, Kido K, Matono K, Shirouzu K. Transanal dilation using circular stapling for benign rectal stenosis: report of a case. Kurume Med J. 2002;49:149–151. doi: 10.2739/kurumemedj.49.149. [DOI] [PubMed] [Google Scholar]
- 14.Brandimarte G, Tursi A, Gasbarrini G. Endoscopic treatment of benign anastomotic colorectal stenosis with electrocautery. Endoscopy. 2000;32:461–463. doi: 10.1055/s-2000-651. [DOI] [PubMed] [Google Scholar]
- 15.Wholey MH, Levine EA, Ferral H, Castaneda-Zuniga W. Initial clinical experience with colonic stent placement. Am J Surg. 1998;175:194–197. doi: 10.1016/s0002-9610(97)00285-7. [DOI] [PubMed] [Google Scholar]
- 16.Mainar A, Tejero E, Maynar M, Ferral H, Castañeda-Zúñiga W. Colorectal obstruction: treatment with metallic stents. Radiology. 1996;198:761–764. doi: 10.1148/radiology.198.3.8628867. [DOI] [PubMed] [Google Scholar]
- 17.Kang SG, Jung GS, Cho SG, Kim JG, Oh JH, Song HY, Kim ES. The efficacy of metallic stent placement in the treatment of colorectal obstruction. Korean J Radiol. 2002;3:79–86. doi: 10.3348/kjr.2002.3.2.79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wengrower D, Fiorini A, Valero J, Waldbaum C, Chopita N, Landoni N, Judchack S, Goldin E. EsophaCoil: long-term results in 81 patients. Gastrointest Endosc. 1998;48:376–382. doi: 10.1016/s0016-5107(98)70006-9. [DOI] [PubMed] [Google Scholar]
- 19.Song HY, Park SI, Do YS, Yoon HK, Sung KB, Sohn KH, Min YI. Expandable metallic stent placement in patients with benign esophageal strictures: results of long-term follow-up. Radiology. 1997;203:131–136. doi: 10.1148/radiology.203.1.9122381. [DOI] [PubMed] [Google Scholar]
- 20.Friedland S, Hallenbeck J, Soetikno RM. Stenting the sigmoid colon in a terminally ill patient with prostate cancer. J Palliat Med. 2001;4:153–156. doi: 10.1089/109662101750290182. [DOI] [PubMed] [Google Scholar]
- 21.Harris GJ, Senagore AJ, Lavery IC, Fazio VW. The management of neoplastic colorectal obstruction with colonic endolumenal stenting devices. Am J Surg. 2001;181:499–506. doi: 10.1016/s0002-9610(01)00622-5. [DOI] [PubMed] [Google Scholar]
- 22.Law WL, Choi HK, Chu KW, Tung HM. Radiation stricture of rectosigmoid treated with self-expanding metallic stent. Surg Endosc. 2002;16:1106–1107. doi: 10.1007/s00464-001-4113-1. [DOI] [PubMed] [Google Scholar]