

Abstract
AIM: To investigate the expressions of E-cadherin and calretinin in exfoliated cells of serous effusions and evaluate their values in distinguishing malignant effusions from benign ones.
METHODS: Fresh serous effusion specimens were centrifuged and exfoliated cells were collected. Cells were then processed with a standardized procedure, including paraformaldehyde fixation, BSA-PBS solution washing and smears preparation. E-cadherin and calretinin were detected by immunocytochemistry (ICC).
RESULTS: In the exfoliated cells of serous effusions, most of carcinoma cells only expressed E-cadherin, and most of mesothelial cells only expressed calretinin, and benign cells (lymphocytes and granulocytes) did not express either of them. For E-cadherin, 85.7% (30/35) of malignant effusions and 8.1% (3/37) of benign fluids were ICC-positive (P < 0.001). The sensitivity of E-cadherin ICC in the diagnosis of malignant effusions was 85.7%, specificity 91.9%, and diagnostic rate 88.9%. For calretinin, 94.6% (35/37) of benign effusions and 11.4% (4/35) of malignant effusions were ICC-positive (P < 0.001). The sensitivity of calretinin ICC in the diagnosis of benign effusions was 94.6%, specificity 88.6%, and diagnostic rate 91.7%. For diagnosis of benign and malignant effusions by combining E-cadherin ICC and calretinin ICC, the specificities were up to 100% and 97.1%, respectively.
CONCLUSION: E-cadherin ICC and calretinin ICC are sensitive and specific in differential diagnosis of benign and malignant serous effusion specimens and specificities are evidently improved when both markers are combined.
INTRODUCTION
Serous effusions are common in clinical practice and some cases are caused by metastasis of malignant tumors (malignant effusions). Distinguishing malignant from benign tumors is very important, but sometimes very difficult[1]. Some studies have shown that immunocytochemistry (ICC) of exfoliated cells is valuable in differentiating malignant effusions from benign ones[2-6]. However, the diagnostic value of a single marker was limited, and a panel of markers were more useful[7,8]. Recently, several studies have shown that E-cadherin, an epithelial adhesion molecule, was a useful marker for identifying the carcinoma cells in effusions[9,10], and calretinin, a calcium-binding protein, was a useful marker for identifying the mesothelial cells[11,12]. It is well known that the differentiation between cancer cells and reactive mesothelial cells is the main problem in cytological diagnosis of effusions. In the present study, both E-cadherin and calretinin were used as markers in immunocytochemical staining of exfoliated cells in serous effusions, and their diagnostic values were evaluated.
MATERIALS AND METHODS
Patients and specimens
Seventy-two patients with serous effusions were enrolled in this study (35 male, 37 female, age 14-77 years with an average of 51.8 years). All patients were from the First Affiliated Hospital of Jiangxi Medical College from 2001 to 2002. Effusion specimens were collected and divided into two groups, benign and malignant, according to cytological results. Of these specimens, there were 45 pleural effusions, 24 peritoneal effusions, and 3 malignant pericardial effusions. In the 23 cases of benign pleural effusions, there were 13 cases of tuberculous pleuritis, 2 cases of liver cirrhosis, 1 pulmonary tuberculosis, 1 chyle pleural effusion, and 6 unknown causes. In the 22 cases of malignant pleural effusion, there were 11 cases of lung cancer, 1 submaxillary gland cancer, 1 gastric cancer, 1 primary liver cancer, and 8 cases of unknown origin. In the 14 cases of benign peritoneal effusions, there were 8 cases of liver cirrhosis, 3 tuberculous peritonitis, 1 hepatitis B, 1 Budd-Chiari syndrome, 1 unknown cause. In the 10 cases of malignant peritoneal effusions, there were 4 cases of ovarian cancer, 2 primary liver cancers, 1 gastric cancer, 1 colonic cancer, 1 duodenal papilla cancer, and 1 unknown origin. Three cases of malignant pericardial effusions included 1 case of lung cancer, 1 metastatic squamous cancer and 1 unknown origin.
Specimen processing
About 100 mL fresh effusion was centrifuged at 2000 r/min for 10 min, and cell pellets were collected. When the effusion was bloody, erythrocytes were destroyed with isotonic ammonium chloride solution (NH4Cl 4.5 g, KHCO3 0.5 g, EDTA 0.0186 g, solved in 400 mL distilled water, then distilled water add to a total volume of 500 mL). Same volume of the solution was added to dissolve the cell pellets, which were stirred for 5 min at room temperature, centrifuged at 2000 r/min for 10 min, and the supernatants removed. Two cell smears were prepared for cytological diagnosis. The remaining cells were processed with a “standardized” procedure[13]: fixed in 40 g/L paraformaldehyde-PBS solution, washed in 10 g/L BSA-PBS solution, the cell concentration was adjusted to 2 × 10 6/mL, and finally several cell smears were prepared. The smears were air-dried and stored in a freezer ( -85 °C).
Immunocytochemistry and evaluation
Reagents for immunocytochemical staining were provided by Beijing Zhongshan Biotechnology Co. Ltd. Mouse anti-human E-cadherin monoclonal antibody (1:100 dilution) or rabbit anti-human calretinin polyclonal antibody (1:50 dilution) was used as the primary antibody. Biotinylated goat anti-mouse/rabbit IgG was used as the second antibody. The reaction products were visualized by using the streptavidin-horseradish peroxidase and diaminobenzidine. The smears were counterstained with hematoxylin. PBS was used instead of the primary antibodies as negative control.
In E-cadherin ICC, positive cells were stained at cytomembrane, especially in the areas surrounding the cells. In calretinin ICC, whole cells were stained with a “fried eggs” staining pattern. One hundred cells (carcinoma and/or non-carcinoma) were counted under a high power microscope, and the percentage of positive cells was calculated. ICC-positive cells > / = 80% were defined as strong expression ( + + + ), 20%-79% as moderate expression ( + + ), 6%-19% as weak expression ( + ), 0-5% as negative expression ( - ). Specimens with expressions ( + )-( + + + ) were regarded as ICC-positive, and expression ( - ) as ICC-negative.
Statistical analysis
Qualitative data were analysed with chi-square test, and rank data were tested with rank sum test. Diagnostic values of ICC results were calculated in contrast to that of the cytological results. Diagnostic values of the combination of E-cadherin and calretinin ICC results were calculated in series ways.
RESULTS
E-cadherin expression of exfoliated cells in serous effusions
E-cadherin expression in carcinoma cells was usually strong, with obvious staining at cytomembrane and sometimes in cytoplasm (Figure 1). The areas surrounding the cells had densely stained lines in the clusters of carcinoma cells, but single carcinoma cell was weakly stained. Mesothelial cells were stained occasionally, and no lymphocytes and granulocytes were stained. Thirty of 35 malignant effusion specimens were ICC-positive for E-cadherin (85.7%), and most of them were strong (93.3% was + + - + + +). Only 3 of 37 benign effusions were ICC-positive for E-cadherin (8.1%), in which a few mesothelial cells were weakly stained in cytoplasm. The differences in positivity rates and expression intensities between two groups were significant (P < 0.001-0.0001) (Table 1).
Figure 1.
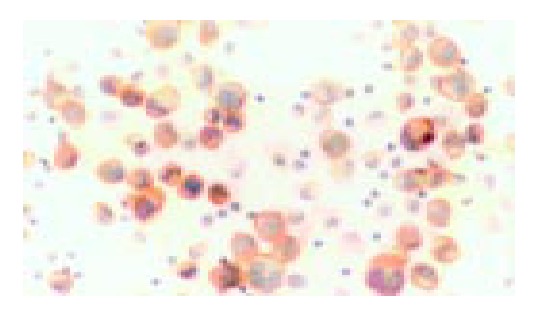
Immunocytochemistry of E-cadherin in the cells from a malignant ascites specimen. Carcinoma cells were mainly stained at cell membranes. Inflammatory cells without stain-ing were as control (Original magnification, × 400).
Table 1.
E-cadherin expression in exfoliated cells of serous effusions
| Effusion group | n | Positivity (%) |
Expression intensity |
|||
| – | + | ++ | +++ | |||
| Malignant | 35 | 30 (85.7) | 5 | 2 | 21 | 7 |
| Benign | 37 | 3 (8.1) | 34 | 1 | 2 | 0 |
χ 2 = 43.633, P < 0.001 between the two groups, H = 42.744, P < 0.0001 between the two groups.
Calretinin expression of exfoliated cells in serous effusions
Calretinin expression in mesothelial cells was usually high, stained in whole cells (Figure 2). The typical cells looked like “fried eggs”. Carcinoma cells were occasionally stained weakly, and no lymphocytes and granulocytes were stained. Thirty-five of 37 benign effusions were ICC-positive for calretinin (94.6%), and all of them were strong positive ( + + + ). Only 4 of 35 malignant effusion specimens were ICC-positive for calretinin (11.4%), with a few carcinoma cells stained weakly. Differences of positivity rates and expression intensities between the two groups were significant (P < 0.001-0.0001) (Table 2).
Figure 2.
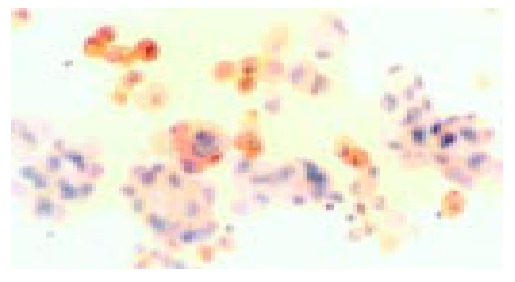
Immunocytochemistry of calretinin in the cells from a malignant ascites specimen. Mesothelial cells were stained strongly and some of them like “fried eggs”. Carcinoma cells and inflammatory cells without staining were as control (Original magnification, × 400).
Table 2.
Calretinin expression in exfoliated cells of serous effusions
| Effusion group | n | Positivity (%) |
Expression intensity |
|||
| – | + | ++ | +++ | |||
| Malignant | 35 | 4 (11.4) | 31 | 1 | 3 | 0 |
| Benign | 37 | 35 (94.6) | 2 | 0 | 0 | 35 |
χ 2 = 50.109, P < 0.001 between the two groups, H = 59.576, P < 0.0001 between the two groups.
Diagnostic values of E-cadherin ICC or/and calretinin ICC for serous effusions
The diagnostic values (sensitivity, specificity) of both E-cadherin ICC and calretinin ICC for malignant effusions were > / = 90%. Combination analysis of E-cadherin ICC and calretinin ICC could improve the specificities (up to 97.1%-100%), while the sensitivities maintained at an acceptable level (Table 3).
Table 3.
Diagnostic values of E-cadherin or/and calretinin ICC for serous effusions
| Index |
Malignant effusion (%) |
Benign effusion (%) |
||
| E-cadherin | E(+) + C(-) | Calretinin | E(-) + C(+) | |
| Sensitivity | 85.7 | 77.1 | 94.6 | 86.5 |
| Specificity | 91.9 | 100 | 88.6 | 97.1 |
| PV+ | 90.9 | 100 | 89.7 | 97.0 |
| PV- | 87.2 | 82.2 | 93.9 | 87.2 |
| DAR | 88.9 | 88.9 | 91.7 | 91.7 |
E ( + )/E ( - ): E-cadherin ( + )/( - ); C ( + )/C ( - ): Calretinin ( + )/( - ); PV + : ICC-positive predictive value; PV-: ICC-negative predic-tive value; DAR: Accordance rate.
DISCUSSION
Serous effusions are common clinical syndromes and can be simply divided into benign and malignant. Differentiation between two kinds of effusions is very important for diagnosis, treatment and prognostic evaluation. The cytological examination is a simple and reliable method for the diagnosis of malignant effusions, but its sensitivity is only 40-60%[14], even lower in clinical practice. Cytological examinations are based on the cellular morphology, which may raise difficulties in distinguishing carcinoma cells from reactive mesothelial cells. Sometimes, carcinoma cells without typical morphological changes or enough number could not be diagnosed cytologically. How to identify the metastatic carcinoma cells and differentiate them from reactive mesothelial cells is key to diagnosing malignant effusions[15]. In the past decade, immunocytochemistry seemed to be a valuable tool in solving the problem, with a complementary value for cytological diagnosis of malignant effusions[16].
The cadherin family consists of more than 16 kinds of molecules that make up a group of phylogenetically and structurally related molecules, with Mr 120 000[17]. E-cadherin, one member of a family of intracellular calcium-dependent adhesion molecules, is a transmembrane protein expressed in epithelial cells. Its extracellular amino terminal binds to the same structure of neighboring homotypic cells when calcium ion exists, mediating the epithelial cell-cell adhesion. Theoretically, only the exfoliated cells originating from epithelial tissues can express E-cadherin, so detection of E-cadherin expression is helpful for determining cells from epithelia. Because no epithelial cells were in benign effusions, the appearance of epithelial cells in effusions means a metastasis of carcinoma developed from epithelia. Our results showed that E-cadherin ICC of the exfoliated cells were valuable for the diagnosis of malignant effusions, with a sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic rate near or over 90% respectively, similar to other studies[1,18]. However, when epithelial cells transformed into malignant cells, E-cadherin expression might decrease to some extent[19,20]. That is the reason why a few carcinoma cells showed weak or negative E-cadherin expression in effusions.
Calretinin is a calcium adhesion protein with Mr 29000 and mainly expresses in nerve system. Lately, it was found that calretinin selectively expressed in mesotheliomas[21,22], with powerful ability to differentiate mesothelial cells from other cells in effusions[1,5,11,22]. Our results showed that calretinin expression in mesothelial cells was evident, but not in non-mesothelial cells, therefore it is useful in determining the cells from mesothelium, with a sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic rate all near or over 90%. The “fried eggs” staining pattern made calretinin ICC more valuable in differentiating mesothelial cells from carcinoma cells[1].
E-cadherin is an epithelial cell marker, and calretinin is a mesothelial cell marker. Our results showed that the combination of both markers significantly increased their differential diagnostic value with specificities up to 97.1% in serous effusions and 100% in benign and malignant effusions.
Footnotes
Edited by Chen WW and Zhu LH Proofread by Xu FM
References
- 1.Chhieng DC, Yee H, Schaefer D, Cangiarella JF, Jagirdar J, Chiriboga LA, Jagirdar J, Chiriboga LA, Cohen JM. Calretinin staining pattern aids in the differentiation of mesothelioma from adenocarcinoma in serous effusions. Cancer. 2000;90:194–200. doi: 10.1002/1097-0142(20000625)90:3<194::aid-cncr8>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 2.Ascoli V, Scalzo CC, Taccogna S, Nardi F. The diagnostic value of thrombomodulin immunolocalization in serous effusions. Arch Pathol Lab Med. 1995;119:1136–1140. [PubMed] [Google Scholar]
- 3.Ascoli V, Carnovale-Scalzo C, Taccogna S, Nardi F. Utility of HBME-1 immunostaining in serous effusions. Cytopathology. 1997;8:328–335. doi: 10.1111/j.1365-2303.1997.tb00557.x. [DOI] [PubMed] [Google Scholar]
- 4.Morgan RL, De Young BR, McGaughy VR, Niemann TH. MOC-31 aids in the differentiation between adenocarcinoma and reactive mesothelial cells. Cancer. 1999;87:390–394. doi: 10.1002/(sici)1097-0142(19991225)87:6<390::aid-cncr10>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- 5.Zimmerman RL, Fogt F, Goonewardene S. Diagnostic utility of BCA-225 in detecting adenocarcinoma in serous effusions. Anal Quant Cytol Histol. 2000;22:353–357. [PubMed] [Google Scholar]
- 6.Afify AM, Al-Khafaji BM, Paulino AF, Davila RM. Diagnostic use of muscle markers in the cytologic evaluation of serous fluids. Appl Immunohistochem Mol Morphol. 2002;10:178–182. doi: 10.1097/00129039-200206000-00014. [DOI] [PubMed] [Google Scholar]
- 7.Davidson B, Risberg B, Kristensen G, Kvalheim G, Emilsen E, Bjåmer A, Berner A. Detection of cancer cells in effusions from patients diagnosed with gynaecological malignancies. Evaluation of five epithelial markers. Virchows Arch. 1999;435:43–49. doi: 10.1007/s004280050393. [DOI] [PubMed] [Google Scholar]
- 8.Ko EC, Jhala NC, Shultz JJ, Chhieng DC. Use of a panel of markers in the differential diagnosis of adenocarcinoma and reactive mesothelial cells in fluid cytology. Am J Clin Pathol. 2001;116:709–715. doi: 10.1309/PJ7H-A52V-M3XB-V94Y. [DOI] [PubMed] [Google Scholar]
- 9.Schofield K, D'Aquila T, Rimm DL. The cell adhesion molecule, E-cadherin, distinguishes mesothelial cells from carcinoma cells in fluids. Cancer. 1997;81:293–298. [PubMed] [Google Scholar]
- 10.Schofield K, D'Aquila T, Rimm DL. E-cadherin expression is a sensitive and specific method for detection of carcinoma cells in fluid specimens. Diagn Cytopathol. 2000;22:263–267. doi: 10.1002/(sici)1097-0339(200005)22:5<263::aid-dc1>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- 11.Barberis MC, Faleri M, Veronese S, Casadio C, Viale G. Calretinin. A selective marker of normal and neoplastic mesothelial cells in serous effusions. Acta Cytol. 1997;41:1757–1761. doi: 10.1159/000333181. [DOI] [PubMed] [Google Scholar]
- 12.Wieczorek TJ, Krane JF. Diagnostic utility of calretinin immunohistochemistry in cytologic cell block preparations. Cancer. 2000;90:312–319. [PubMed] [Google Scholar]
- 13.Kuenen-Boumeester V, van Loenen P, de Bruijn EM, Henzen-Logmans SC. Quality control of immunocytochemical staining of effusions using a standardized method of cell processing. Acta Cytol. 1996;40:475–479. doi: 10.1159/000333902. [DOI] [PubMed] [Google Scholar]
- 14.Fenton KN, Richardson JD. Diagnosis and management of malignant pleural effusions. Am J Surg. 1995;170:69–74. doi: 10.1016/s0002-9610(99)80257-8. [DOI] [PubMed] [Google Scholar]
- 15.Bedrossian CW. Diagnostic problems in serous effusions. Diagn Cytopathol. 1998;19:131–137. doi: 10.1002/(sici)1097-0339(199808)19:2<131::aid-dc14>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 16.Delahaye M, Van der Ham F, Van der Kwast TH. Comple-mentary value of five carcinoma markers for the diagnosis of malignant mesothelioma, adenocarcinoma metastasis, and re-active mesothelium in serous effusions. Diagn Cytopathol. 1997;17:115–120. doi: 10.1002/(sici)1097-0339(199708)17:2<115::aid-dc6>3.0.co;2-f. [DOI] [PubMed] [Google Scholar]
- 17.Harrington KJ, Syrigos KN. The role of E-cadherin-catenin complex: more than an intercellular glue? Ann Surg Oncol. 2000;7:783–788. doi: 10.1007/s10434-000-0783-5. [DOI] [PubMed] [Google Scholar]
- 18.Simsir A, Fetsch P, Mehta D, Zakowski M, Abati A. E-cadherin, N-cadherin, and calretinin in pleural effusions: the good, the bad, the worthless. Diagn Cytopathol. 1999;20:125–130. doi: 10.1002/(sici)1097-0339(199903)20:3<125::aid-dc3>3.0.co;2-v. [DOI] [PubMed] [Google Scholar]
- 19.Wijnhoven BP, Dinjens WN, Pignatelli M. E-cadherin-catenin cell-cell adhesion complex and human cancer. Br J Surg. 2000;87:992–1005. doi: 10.1046/j.1365-2168.2000.01513.x. [DOI] [PubMed] [Google Scholar]
- 20.Cai KL, Wang GB, Xiong LJ. Effects of carbon dioxide and nitrogen on adhesive growth and expressions of E-cadherin and VEGF of human colon cancer cell CCL-228. World J Gastroenterol. 2003;9:1594–1597. doi: 10.3748/wjg.v9.i7.1594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gotzos V, Vogt P, Celio MR. The calcium binding protein calretinin is a selective marker for malignant pleural mesotheliomas of the epithelial type. Pathol Res Pract. 1996;192:137–147. doi: 10.1016/S0344-0338(96)80208-1. [DOI] [PubMed] [Google Scholar]
- 22.Doglioni C, Dei Tos AP, Laurino L, Iuzzolino P, Chiarelli C, Celio MR, Viale G. Calretinin: a novel immunocytochemical marker for mesothelioma. Am J Surg Pathol. 1996;20:1037–1046. doi: 10.1097/00000478-199609000-00001. [DOI] [PubMed] [Google Scholar]