

Abstract
Objective:
To determine the stability of improvement in polysomnographic measures of sleep disordered breathing, patient reported outcomes, the durability of hypoglossal nerve recruitment and safety at 18 months in the Stimulation Treatment for Apnea Reduction (STAR) trial participants.
Design:
Prospective multicenter single group trial with participants serving as their own controls.
Setting:
Twenty-two community and academic sleep medicine and otolaryngology practices.
Measurements:
Primary outcome measures were the apnea-hypopnea index (AHI) and the 4% oxygen desaturation index (ODI). Secondary outcome measures were the Epworth Sleepiness Scale (ESS), the Functional Outcomes of Sleep Questionnaire (FOSQ), and oxygen saturation percent time < 90% during sleep. Stimulation level for each participant was collected at three predefined thresholds during awake testing. Procedure- and/or device-related adverse events were reviewed and coded by the Clinical Events Committee
Results:
The median AHI was reduced by 67.4% from the baseline of 29.3 to 9.7/h at 18 mo. The median ODI was reduced by 67.5% from 25.4 to 8.6/h at 18 mo. The FOSQ and ESS improved significantly at 18 mo compared to baseline values. The functional threshold was unchanged from baseline at 18 mo. Two participants experienced a serious device-related adverse event requiring neurostimulator repositioning and fixation. No tongue weakness reported at 18 mo.
Conclusion:
Upper airway stimulation via the hypoglossal nerve maintained a durable effect of improving airway stability during sleep and improved patient reported outcomes (Epworth Sleepiness Scale and Functional Outcomes of Sleep Questionnaire) without an increase of the stimulation thresholds or tongue injury at 18 mo of follow-up.
Citation:
Strollo PJ, Gillespie MB, Soose RJ, Maurer JT, de Vries N, Cornelius J, Hanson RD, Padhya TA, Steward DL, Woodson BT, Verbraecken J, Vanderveken OM, Goetting MG, Feldman N, Chabolle F, Badr MS, Randerath W, Strohl KP, Stimulation Therapy for Apnea Reduction Trial Group. Upper airway stimulation for obstructive sleep apnea: durability of the treatment effect at 18 months. SLEEP 2015;38(10):1593–1598.
Keywords: upper airway stimulation, obstructive sleep apnea, therapy, hypoglossal nerve stimulation, pacing
INTRODUCTION
Untreated obstructive sleep apnea (OSA) is a significant public health problem.1 Upper airway stimulation (UAS) has been shown to be safe and effective in participants with moderate-to-severe OSA, who could not adhere to positive airway pressure therapy.2 The mechanism of action of UAS involves unilateral stimulation of the hypoglossal nerve to recruit the genioglossus muscle generating anterior displacement of the tongue, and dilation of the pharynx, leading to relief of airway obstruction during sleep.3–6
In a previous report,2 improvement in the primary outcome measures consisting of the apnea- hypopnea index (AHI) and the 4% oxygen desaturations index (ODI), and the secondary outcome measures consisting of self-reported sleepiness using the Epworth Sleepiness Scale (ESS), the Functional Outcomes of Sleep Questionnaire (FOSQ), and the percentage sleep time SaO2 < 90% were demonstrated at 12 mo after implantation. In a separate report of participants in a randomized therapy withdrawal portion of the study (n = 46), suspension of therapy for 1 w led to return of OSA severity and self-report ESS and FOSQ to the baseline level, and reactivation of therapy-maintained therapy efficacy at 18 mo.7 The current report focuses on the stability of the primary and secondary outcome measures, the durability of hypoglossal nerve recruitment, and overall safety of all study participants at 18 mo in the STAR (Stimulation Treatment for Apnea Reduction) trial.
METHODS
Participants
The STAR trial cohort included adults with a diagnosis of moderate to severe OSA who would not accept or adhere to treatment with continuous positive airway pressure (CPAP) therapy. The STAR trial study design was an international prospective multicenter single group trial with participants serving as their own controls. Participants were recruited from 13 community and nine academic sleep medicine and otolaryngology practices. The trial protocol was approved by the individual institutional review boards (in the United States) or the medical ethics committees (in Europe) at each center. All participants provided written informed consent before enrollment. Key exclusion criteria included body mass index > 32 kg/m2, neuromuscular diseases (including hypoglossal nerve palsy or injury), severe cardiopulmonary disorders (chronic obstructive pulmonary disease, pulmonary arterial hypertension, heart failure, persistent uncontrolled hypertension despite medications, a recent myocardial infarction (within 6 mo) or severe cardiac arrhythmias), active psychiatric disease, and comorbid nonrespiratory sleep disorders that would confound functional assessments related to sleep.
Participants who met inclusion/exclusion criteria underwent three screening tests: in-laboratory attended polysomnography (PSG), a surgical consultation visit, and drug-induced sedated endoscopy (DISE). Participants were excluded after the PSG for an AHI less than 20 or greater than 50; a central and/or mixed apnea index > 25% of the AHI; or a nonsupine AHI < 10. Participants were excluded during surgical consultation if pronounced anatomical abnormalities would prevent effective use or assessment of the device (e.g., tonsil size 3 or 4). DISE excluded any participant with observed complete concentric collapse at the level of the velopharynx because individuals with this particular pattern of airway obstruction responded poorly to UAS therapy in a prior feasibility study.8
Surgical Procedures
Qualified participants who met preimplant screening criteria underwent device implantation. Details of the surgical technique are described in a prior publication.5 The implanted system consists of three components: a stimulation cuff electrode which encircles a distal branch of the right hypoglossal nerve; a pressure sensing lead placed within the fourth or fifth right intercostal space to detect ventilatory effort; and an implantable pulse generator inserted into a subcutaneous pocket beneath the right mid-clavicle contralateral to the region commonly used in cardiac pacemaker implantation (Figure 1). The therapy is designed to sense ventilatory effort and provide synchronized stimulation to the hypoglossal nerve in order to increase airway muscle tone and luminal diameter.
Figure 1.
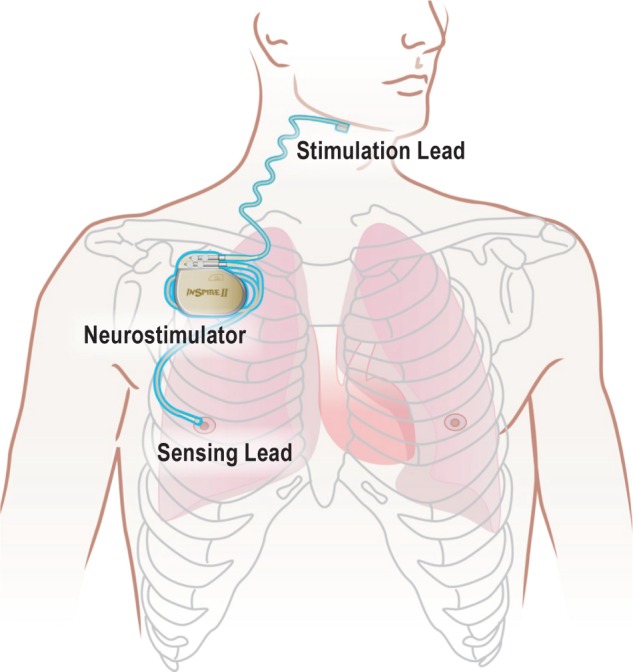
Upper airway stimulation (UAS) system for obstructive sleep apnea. The neurostimulator delivers electrical stimulating pulses to the hypoglossal nerve through the stimulation lead, synchronized with ventilation detected by the sensing lead. Stimulation lead: the main trunk of the hypoglossal nerve (XII) was exposed through a horizontal upper neck incision at the inferior border of the submandibular gland. The nerve was followed anteromedially until it branched into a lateral (l–XII) and a medial (m-XII) division. The stimulation lead was placed on the m-XII branch. The cuff section of stimulation lead includes three electrodes that can be configured in a variety of unipolar of bipolar electrode manner for optimal UAS. Appropriate placement of the stimulation lead was confirmed by observing tongue protrusion upon stimulation. Sensing lead: a second incision was made horizontally at the fourth intercostal region. The dissection was aimed at the upper border of the underlying rib. A 5-cm tunnel was created from posterior to anterior between the external and internal intercostal muscle. The ventilatory sensor was placed in the tunnel, with the sensing side facing inward. Neurostimulator: a third incision was made horizontally 2 cm inferior to the right clavicle. A pocket was created inferior to the incision and superficial to the pectoralis major muscle to accommodate the neurostimulator (implanted pulse generator or IPG). With a subcutaneous tunneling device, the leads of the stimulation electrode and the pressure sensor were led into the infraclavicular pocket space and connected to the IPG. Adequate functioning of the system was confirmed before closure.
Study Procedures
All participants had their device activated after a second baseline PSG, 1 mo following the implant procedure. PSGs and self-reported questionnaires were collected at both 12-and 18-mo follow-up visits. The primary outcomes assessed were changes in AHI and ODI from baseline to follow-up. Secondary outcome measures included patient reported outcomes, using the ESS and the FOSQ and percentage sleep time SaO2 < 90%. Clinical variables, including body mass index (BMI), neck circumference, and awake blood pressure, were measured at scheduled study visits in order to assess for any changes over the course of the study.
To determine whether there was a change in nerve recruitment over time, the stimulation level for each participant was collected at three predefined functional thresholds: sensation (minimal stimulation level perceived by the participant); bulk motion of the tongue; and discomfort (highest stimulation level tolerated by the participant) during awake testing. For consistency, all stimulation thresholds were collected at the same bipolar electrode configuration, stimulation frequency (33 Hz), and pulse duration (90 for all participants. Device parameters were adjusted for optimal therapy during titration PSG studies prior to the 12-mo follow-up.
All reported adverse events were reviewed and coded by the Clinical Events Committee. Serious adverse events were defined as any events that led to death, life-threatening illness, permanent impairment, or new or prolonged hospitalization. Adverse events were categorized as procedure related if they were due to the surgical procedure or the device after therapy activation.
Statistical Analysis
The sample size was calculated on the basis of previous studies.5 Approximately 108 participants were required for the primary endpoint evaluation using the exact one-sided binomial test at a significant level of 2.5% with 80% power. For primary endpoints, the AHI and ODI were compared to the baseline measurement, which was the average of the preimplant and 1 mo preactivation measurements. For post-12 mo results, post hoc paired t-tests were used to evaluate the difference between baseline and 12 mo and between 12 mo and 18 mo at the 5% significant level. No adjustments for multiplicity were made.
Role of the Funding Source
The STAR trial was funded by Inspire Medical Systems (Clinical Trials.gov number, NCT01161420). The protocol was developed by the company, study investigators, and the US Food and Drug Administration. An independent clinical events committee and a data and safety monitoring board provided review and adjudication of safety data. Verification of source data was performed by independent monitors. The study investigators had full access to the data and had the right to submit the manuscript for publication without input from the sponsor. The writing committee (the first, second, and last authors), an independent statistician (Teri Yurik, NAMSA), and the sponsor vouch for the accuracy and completeness of the data and analyses.
RESULTS
Characteristics of the Implanted Participants
The study population at implantation consisted of 126 participants, mostly Caucasian (97%) males (83%) with a mean age of 54.5 y (range, 31 to 80 y) and mean BMI of 28.4 kg/m2 (range, 18.4 to 32.5). Demographics of the initial study population are presented in Table 1. A total of 124 and 123 participants completed follow-up at 12 and 18 mo respectively (Figure 2), and their mean BMI was 28.5 kg/m2 at both 12 and 18 mo, which was unchanged from baseline.
Table 1.
Base line demographics.

Figure 2.

Study flow diagram. AHI, apnea-hypopnea index.
Primary Outcomes
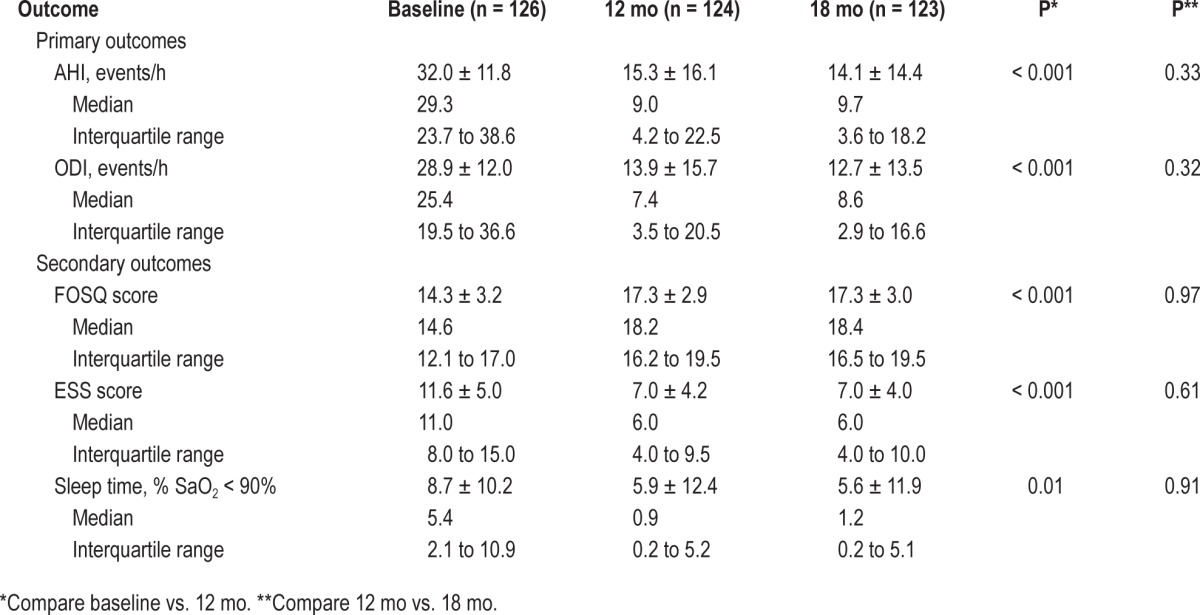
The primary outcomes measures (AHI and ODI) were improved at both 12 and 18 mo compared to baseline (Table 2). The median AHI was reduced by 67.4% from the baseline of 29.3/h to 9.7/h at 18 mo. The median ODI was reduced by 67.5% from 25.4 to 8.6/h at 18 mo. Response to therapy defined as, at least a 50% reduction and AHI < 20/h, was achieved in 64% of participants at 18 mo using intent-to-treat analysis. There were 29%, 52%, and 69% of participants with AHI less than 5, 10, or 15 at 18, respectively.
Table 2.
Primary and secondary outcome measures.
Secondary Outcomes
The FOSQ and ESS improved significantly at 18 mo compared to baseline values (Table 2). The improvement of FOSQ exceeded a two-point or more point increase, considered clinically meaningful improvement9; similarly the ESS score was consistent with normalization of the measure (i.e., ESS < 10). Among therapy nonresponders, 63% had a clinical meaningful improvement in FOSQ (≥ 2 in FOSQ increase) and 78% had a clinical meaningful improvement in ESS (≥ 2 in ESS reduction). The percent time for SaO2 < 90% of total sleep was reduced from a baseline value of 5.4% to 1.2% at 18 mo.
Durability of Therapy Response and Stimulation Parameters
All primary and secondary outcome measures were similar at 12 and at 18 mo. The average difference was −1.06/h (95% confidence interval (CI) −3.2 to 1.1/h) for AHI, and −1.02/h (95% CI −3.0 to 1.0/h) for ODI from 12 to 18 mo. Similarly, no difference was observed in FOSQ, ESS, and SaO2 between the two time points (Figure 3).
Figure 3.

Change in polysomnographic measures of sleep disordered breathing and patient reported measures from baseline to 18 mo. Tukey Box Plots: the box marks out the 25th to 75th percentiles; the line within that box marks the median; a line marks the outer part of the distribution, and outliers are represented as an o, x, or +. (A) Apnea-hypopnea index (AHI) at baseline, month 12, and month 18. (B) 4% oxygen desaturation index (ODI) at baseline, month 12, and month 18. (C) Functional Outcomes of Sleep Questionnaire (FOSQ) scores at baseline, month 12, and month 18. (D) Epworth Sleepiness Score (ESS) at baseline, month 12, and month 18. N, number of participants.
To address whether there was a change in device function over time, stimulation levels for each participant were collected at three predefined thresholds (sensation, bulk motion, and discomfort). The values for amplitude in volts at each threshold from initial therapy activation at 1 mo postimplantation, to 12 and 18 mo are displayed in Table 3. The functional threshold was unchanged from baseline at 18 months.
Table 3.
Stimulation threshold.

Adverse Events
The average duration of follow up for safety after implant was 911.3 ± 137.8 days (range, 310 to 1,197 days) after implant among all 126 participants. Two participants experienced a serious device-related adverse event that was related to the implanted pulse generator only. One participant reported discomfort 1 mo postimplant with a downward migration of the implanted pulse generator. The discomfort was resolved with repositioning and fixation of the device. The other event reported between 12 and 18 mo with a similar complaint of discomfort with a device that was in a non-standard lateral infraclavicular position. The discomfort was resolved after the device was placed in the standard mid-infraclavicular position. As presented in the previous report of safety after 12 mo follow-up,2 most procedure-related nonserious adverse events (86%) occurred within 30 days postimplant, and were expected postsurgical events. There was no tongue weakness reported at or after 12 months. Among device-related nonserious events reported after 12 months, 12% of the participants reported some discomfort associated with stimulation, and 3% of participants reported tongue soreness including abrasion on the lower side of the tongue. These events were related to the functional stimulation of the tongue muscles and/or the resulting tongue motion over the lower rough or missing teeth. The majority of these events resolved after the participants acclimated to the UAS therapy or through a device reprogramming to optimize stimulation parameters.
DISCUSSION
Upper airway stimulation of the hypoglossal nerve resulted in significant and clinically meaningful improvements in OSA severity, self-reported sleepiness, and quality of life measures at 18 mo after implantation. There were no changes in all primary and secondary outcome measures from 12 to 18 mo, demonstrating a consistent and sustained therapy response. The stimulation level required to produce predefined tongue activation remained stable from 1 mo post-implant to 18 mo. The safety profile remained excellent, with two elective device-related adverse events (pocket revisions for the stimulator) resolved completely by outpatient procedures. Minor discomfort related to stimulation and tongue movement could be addressed by clinical assessment and minor programming adjustment. Between 12 and 18 mo, no additional PSG studies were required.
There are limited treatment alternatives for patients with moderate to severe OSA who cannot adhere to CPAP. Oral appliances (OAs) are generally reserved for patients with mild to moderate OSA.10,11 There is increasing evidence of OA benefit in more severe OSA12,13 with follow-up ranging from 2 to 6 mo. Long-term adherence and outcomes of OA in moderate to severe OSA remain unclear. A substantial portion of patients seek surgical modifications of the upper airway.14 Uvulopalatopharyngoplasty (UPPP), as shown in a recent meta-analysis,15 reduced AHI by approximately 33% (95% CI 23% to 42%), with residual AHI averaging 29.8/h in follow-up from 3 to 12 mo. Similarly, upper airway radiofrequency ablation of the soft palate, the base of the tongue or multiple levels showed an AHI reduction of 34% (95% CI 19% to 46%). There were 22 participants (22%) who had a UPPP at enrollment. At 18 mo, the average AHI among these 22 participants with prior UPPP was 12.3 ± 11.0, which was similar to the AHI of 14.5 ± 15.1 among those without prior UPPP (P = 0.52). By comparison to these primary and “rescue” anatomic procedures, upper airway stimulation, while relatively new, has an established selection profile, a low morbidity, and a relatively high efficacy. Continuous objective device use at night is not recorded with the current generation of the device; however, pulse generation time as a measure of general use was consistent with patient self-report.2
The population that was implanted with the device was 83% male 97% Caucasian. No sex or racial differences had been identified to date relating to the response to upper airway stimulation. However, until additional data are examined the conclusion that the responses would be similar is only speculative.
Adverse events reported after 12 mo resulted from routine device use associated with functional stimulation. The rate of occurrence of these events was reduced after the first 12 mo of follow-up (see supplemental material). The daily use of UAS was 86% at 12 mo and 84% at 18 mo based on self-report. One participant requested elective explant due to lack of clinical improvement. The explant was completed without complications. No other participant discontinued therapy, even if their PSG results placed them in a “nonresponder” group (n = 46). Considering the nonadherent history of the participants with CPAP, the high usage with the neurostimulator suggested improved therapy adherence with the implanted device.
The voltage required for hypoglossal nerve stimulation and its muscle recruitment properties was stable over 18 mo. Specifically, the stimulation level required to produce predefined tongue activation was unchanged from 1 mo to 18 mo. Although longer term follow-up (e.g., 5 y) would be desirable to examine habituation or degradation of efficacy, the current data suggest that the nerve electrode interface became mature after 1 mo, and remained stable after 18 mo. In vagus nerve stimulation for medically refractory epilepsy, follow-up studies from 1 to 6 y16,17 have demonstrated overall stability of stimulation of the peripheral nerve for long-term therapy.
In conclusion, upper airway stimulation via hypoglossal nerve maintained a durable effect of improving airway stability during sleep and patient reported outcomes (ESS and FOSQ) without the need to increase the stimulation thresholds at 18 mo of follow-up. In patients with moderate to severe OSA who are intolerant or nonadherent to CPAP, upper airway stimulation provides a viable treatment option for many months after implantation.
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Strollo received grant support from Inspire Medical Systems during the conduct of the STAR Trial. He is a member of a scientific advisory panel for ResMed Inc. and Jazz Pharmaceuticals; is a consultant for Emmi Solutions, PinMed and the National Football League; and has received grant support from the National Institutes of Health, ResMed, Philips-Respironics. Dr. Gillespie received grant support from Inspire Medical Systems during the conduct of the STAR Trial. Dr. Soose received grant support and personal fees from Inspire Medical Systems during the conduct of the study, and personal fees from Philips-Respironics outside the submitted work. Dr. Maurer received grant support and personal fees from Inspire during the conduct of the study; grant support from Imthera, Phillips, and Revent; and personal fees from GlaxoS-mithKline, Weinmann, Olympus, ResMed, Neuwirth, Medtronic, and Heinen & Löwenstein outside the submitted work. Dr. de Vries received grant support from Inspire Medical Systems during the conduct of the study; has received grant support from NightBalance, and personal fees from Philips, Olympus, and Merck Sharp & Dohme outside the submitted work; and is also a medical advisor to NightBalance and Philips, and holds stock option in ReVent. Drs. Cornelius, Hanson, Padhya, Steward, Verbraecken, Goetting, Feldman, Chabolle, and Randerath received grant support from Inspire Medical Systems during the conduct of the STAR Trial. Dr. Woodson received grant support and personal fees from Inspire Medical Systems during the conduct of the study; has received grant support from Inspire Medical Centers and ResMed Foundation, personal frees from Medtronic, and other support from Siesta Medical outside of the submitted work; and holds a patent (re: hyoid and airway suspension patent), which is licensed to Medtronic and generates royalties. He also has holds patent on an adjustable tongue anchor for OSA, which is licensed to Phillips Respironics. Dr. Vanderveken received grant support from Inspire Medical Systems during the conduct of the study and grant support from SomnoMed outside the submitted work. Dr. Badr received grant support from the National Institutes of Health and from Inspire Medical Systems during the conduct of the STAR Trial. Dr. Strohl received grant and other support from Inspire Medical Systems during the conduct of the study; he received grant support from Inspire Medical Systems, grant support and personal fees from the National Institutes of Health, and personal fees from Galleon and the U.S. Food and Drug Administration outside the submitted work.
SUPPLEMENTAL MATERIAL
List of Study Contributors
STAR Trial Implanting Centers
STAR Trial Implanting Centers

Inspire Medical Systems (Sponsor): Quan Ni, PhD., Kris Selander
Medical Research Biostatistician: Teri Yurik (Namsa, Inc)
Clinical Events Committee: Kent Wilson, MD (Department of Otolaryngology, University of Minnesota (retired); KSW Consulting (current)), Markus Gapany, MD (Department of Otolaryngology, University of Minnesota; Minneapolis VAMC), Sandra M Skovlund, MD (Department of Otolaryngology – Head and Neck Surgery, Park Nicollet Clinic), Erik St. Louis, MD (Department of Neurology, Mayo Clinic and Foundation).
Procedure and Device Related Nonserious Adverse Events
See Table S1.
Table S1.

Procedure and device related nonserious adverse events.
Responder and Nonresponder Analysis
We have compared baseline characteristics between therapy responders and non-responders using measurements collected at 18 mo, and summarize the results in Table S2.
Table S2.

Characteristics of responders and non-responders at 18 mo.
In comparison with responders, nonresponders had similar baseline characteristics in BMI and neck size, slightly younger in age, similar AHI and ODI at baseline, slightly lower proportion with prior UPPP, and similar baseline FOSQ and ESS. There were no statistically significant associations between these characteristics and therapy outcome at 18 mo. These conclusions were consistent with the outcome data at 12 mo. Additional physiological studies of upper airway mechanics are necessary to understand the mechanical coupling between the velopharynx and the tongue-base, which may be the mechanism responsible for the multi-level response among therapy responders.
Among therapy nonresponders, 73% had a reduced level of snoring based on self-report, and 83% had reduced level of snoring based on partner report. These observations are likely to account for the improvement in the patient reported outcomes (FOSQ and ESS) in the nonresponders (see main text Results section – Secondary Outcomes).
Individual Data Points of Responders
See Figure S1.
Indvidual Date Points of Nonresponders
See Figure S2.
Device Adjustments
The upper airway stimulation system is activated 1 mo after the implant procedure. The stimulation amplitude thresholds for sensation, functional tongue response, and subdiscomfort level are obtained during wakefulness. The patient is sent home with a patient remote that allows the patient to turn the Inspire device on at night and to make adjustments the stimulation voltage within a certain range predefined by the physician. Follow-up visits are necessary during the first year to adjust the Inspire device settings.
A key characteristic of upper airway stimulation, as with CPAP and other neurostimulation therapies, is that it is adjustable in order to optimize therapy response and patient comfort. Specifically, the physician adjusts sensing parameters to deliver stimulation during the late expiratory phase and throughout the inspiratory phase of respiration. Amplitude, rate, pulse width, and electrode configuration can be adjusted to provide a patent airway without disturbing sleep.
The most common adjustment is amplitude. Stimulation amplitude is measured in volts and can be adjusted in 0.1-V increments from 0.0 V to 5.0 V. Titration of amplitude is similar in concept to the AASM guidelines for the titration of positive airway pressure in that during PSG studies the amplitude is slowly increased in the presence of obstructive apneas and hypopneas until a stable airway is established.
The patient amplitude control limits are selected by the physician to allow an appropriate and effective range of amplitude selections. The lower amplitude limit is selected to ensure an effective level of stimulation. The upper amplitude limit is selected to provide a reasonable number of amplitude choices for the patient, typically 5 (0.1 V changes) or fewer. For example a physician may choose therapy amplitude of 2.0 V and a patient control range of 1.8 V to 2.2 V.
Patient amplitude control is a common feature of other neurostimulation systems such as spinal cord stimulation for pain and sacral nerve stimulation for incontinence. This feature allows patients to fine-tune their therapy and to be actively engaged in their treatment. This feature is similar conceptually to auto-positive airway pressure (PAP), which allows for adjustments to PAP within physician selected limits.
Individual data points of responders. Among the 83 participants who met responder criteria (AHI < 20 and at least 50% reduction from baseline) at 12 mo (n = 83), 19 (23% of 83) did not meet responder criteria at 18 mo.
Individual data points of nonresponders. Among the 43 participants who did not met responder criteria at 12 mo, a total of 16 (37% of 43) met criteria at 18 mo. The overall responder rate was similar at 12 and 18 mo.
REFERENCES
- 1.Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383:736–47. doi: 10.1016/S0140-6736(13)60734-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Strollo PJ, Jr., Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370:139–49. doi: 10.1056/NEJMoa1308659. [DOI] [PubMed] [Google Scholar]
- 3.Schwartz AR, Bennett ML, Smith PL, et al. Therapeutic electrical stimulation of the hypoglossal nerve in obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 2001;127:1216–23. doi: 10.1001/archotol.127.10.1216. [DOI] [PubMed] [Google Scholar]
- 4.Eastwood PR, Barnes M, Walsh JH, et al. Treating obstructive sleep apnea with hypoglossal nerve stimulation. Sleep. 2011;34:1479–86. doi: 10.5665/sleep.1380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Van de Heyning PH, Badr MS, Baskin JZ, et al. Implanted upper airway stimulation device for obstructive sleep apnea. Laryngoscope. 2012;122:1626–33. doi: 10.1002/lary.23301. [DOI] [PubMed] [Google Scholar]
- 6.Mwenge GB, Rombaux P, Dury M, Lengele B, Rodenstein D. Targeted hypoglossal neurostimulation for obstructive sleep apnoea: a 1-year pilot study. Eur Respir J. 2013;41:360–7. doi: 10.1183/09031936.00042412. [DOI] [PubMed] [Google Scholar]
- 7.Woodson BT, Gillespie MB, Soose RJ, et al. Randomized controlled withdrawal study of upper airway stimulation on OSA: short- and long-term effect. Otolaryngol Head Neck Surg. 2014;151:880–7. doi: 10.1177/0194599814544445. [DOI] [PubMed] [Google Scholar]
- 8.Vanderveken OM, Maurer JT, Hohenhorst W, et al. Evaluation of drug-induced sleep endoscopy as a patient selection tool for implanted upper airway stimulation for obstructive sleep apnea. J Clin Sleep Med. 2013;9:433–8. doi: 10.5664/jcsm.2658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chasens ER, Ratcliffe SJ, Weaver TE. Development of the FOSQ-10: a short version of the Functional Outcomes of Sleep Questionnaire. Sleep. 2009;32:915–9. doi: 10.1093/sleep/32.7.915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Epstein LJ, Kristo D, Strollo PJ, Jr., et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5:263–76. [PMC free article] [PubMed] [Google Scholar]
- 11.Randerath WJ, Verbraecken J, Andreas S, et al. Non-CPAP therapies in obstructive sleep apnoea. Eur Respir J. 2011;37:1000–28. doi: 10.1183/09031936.00099710. [DOI] [PubMed] [Google Scholar]
- 12.Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2013;187:879–87. doi: 10.1164/rccm.201212-2223OC. [DOI] [PubMed] [Google Scholar]
- 13.Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med. 2014;10:215–27. doi: 10.5664/jcsm.3460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kezirian EJ, Maselli J, Vittinghoff E, Goldberg AN, Auerbach AD. Obstructive sleep apnea surgery practice patterns in the United States: 2000 to 2006. Otolaryngol Head Neck Surg. 2010;143:441–7. doi: 10.1016/j.otohns.2010.05.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Caples SM, Rowley JA, Prinsell JR, et al. Surgical modifications of the upper airway for obstructive sleep apnea in adults: a systematic review and meta-analysis. Sleep. 2010;33:1396–407. doi: 10.1093/sleep/33.10.1396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ardesch JJ, Buschman HPJ, Wagener-Schimmel LJJC, van der Aa HE, Hageman G. Vagus nerve stimulation for medically refractory epilepsy: a long-term follow-up study. Seizure. 2007;16:579–85. doi: 10.1016/j.seizure.2007.04.005. [DOI] [PubMed] [Google Scholar]
- 17.Choi SJ, Hong SC, Seo D-W, et al. Long-term outcome of vagus nerve stimulation for refractory epilepsy: a longitudinal 4 year follow-up study in Korea. J Epilepsy Res. 2013;3:16–20. doi: 10.14581/jer.13003. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Individual data points of responders. Among the 83 participants who met responder criteria (AHI < 20 and at least 50% reduction from baseline) at 12 mo (n = 83), 19 (23% of 83) did not meet responder criteria at 18 mo.
Individual data points of nonresponders. Among the 43 participants who did not met responder criteria at 12 mo, a total of 16 (37% of 43) met criteria at 18 mo. The overall responder rate was similar at 12 and 18 mo.