

Abstract
Aim:
The purpose of this study is to compare the efficiency of fluorescence-aided caries excavation (FACE) to remove carious dentin primary teeth with that of conventional methods.
Methods and Materials:
After caries excavation was carried out, dentin surfaces were conventionally inspected using visual tactile criteria and 415 cavities which were classified as caries-free, re-inspected with Face-Light and caries detector dye (CDD) methods. Orange-red fluorescing areas classified as carious dentin, as well as stained carious dentin. All the data were recorded according to localization of the caries and determination efficiency of the methods. X2 test was used to compare the mean values of both Face-Light and dye applications, while Wilcoxon test performed to evaluate the effectiveness for each diagnostic method.
Results:
A total of 273 patients with 415 Class II (OM/OD) cavities (1.65 ± 0.52 teeth per patient) with carious lesions in molar and premolar teeth, were examined. Out of 415 teeth, in 149 teeth (35.9%) no caries findings had been illustrated. While FACE detected remaining carious or partially removed areas in 237 teeth (57.2%), CDD stained only 29 teeth by itself (P < 0.05).
Conclusion:
In conclusion, FACE has a higher detectability compared to visual inspection and caries detector dye in diagnosis and removal of carious dentin.
Keywords: Caries detector dye, fluorescence-aided caries excavation, visual assessment
INTRODUCTION
In the era of minimally invasive dentistry, the common delineator is tissue preservation preferably by preventing disease occurrence and intercepting disease progress, as well as by removing and replacing diseased tissue with as little tissue loss as possible; consequently, this goal has changed dental diagnostic systems and dentistry's approach to dental caries management.[1,2] The traditional visual assessment and probing methods for detecting caries lesions have been commonly used procedures for over 60 years.[3] The diagnostic value of probing dental structures is extremely poor, and the indiscriminate use of sharp hand instruments can cause extensive tooth tissue damage, including iatrogenic pulp injuries, in addition to false-positive diagnoses.[4] Moreover, caries detector dyes (CDDs), which were released as an advancement in diagnostic dentistry, have recently decreased in popularity due to insufficient distinctive properties such as staining the less mineralized circumpulpal and predentin areas[5] which causes possible damage to pulpal tissue.[6]
Optical methods of caries diagnosis are considered as natural and noninvasive methods for lesion detection. These methods present possible advantages of allowing better identification and recognition of the affected area and ease in handling compared to the conventional visual assessment and probing methods.[7,8]
The optical methods that have been introduced recently include the following: Light scattering, fibre-optic transillumination, and fluorescence-aided caries excavation (FACE) by light or laser. During the process of caries formation, bacteria in affected dentine leave metabolic products (porphyrins) behind. Fluorescence light devices generally illuminate blue-violet light; however, when an exposed cavity is illuminated with this type of light, porphyrins display red fluorescence, thereby indicating the significant areas for caries detection and excavation.[9] Owing to the novelty of this study, investigating the caries detection performance of the FACE, which was introduced as a noninvasive new approach, seemed to be interesting. While it is claimed that, visualization of the remaining infected dentin and evaluation of the caries excavation can be performed without any specialization, clinical applicability and diagnostic performance of the method should be investigated.
The aim of this study was to evaluate the clinical applicability and efficiency of FACE by light and CDD methods in cavity preparation after caries excavation using conventional methods to evaluate the null hypothesis that FACE is an advanced diagnostic method compared to CDDs and visual inspection.
MATERIALS AND METHODS
Two hundred and seventy-three patients who were treated at the Restorative Dentistry Clinic at Ege University, Turkey, were selected for this study. The procedure and aims of this study were explained to these patients, and informed consent was obtained from all patients before their participation in this study. This study was conducted in accordance with the Declaration of Helsinki, and Ethics Committee approval was obtained. The following inclusion criteria were used to determine entry into the study: The included teeth must be permanent maxillary or mandibular molar and premolar teeth, caries must represent a primary lesion that could been diagnosed clinically, caries lesions must extend to one of the proximal surfaces (OM/OD), and the teeth must be free of any existing restorations, and any pulpitis symptoms. Pulp exposure due to caries removal and iatrogenic origin were the primary reasons for excluding those teeth from participation in the study.
Access cavities were prepared using a high-speed handpiece (NSK, Nakanishi International, Japan) with diamond burs under continuous water cooling, followed by caries excavation using a low-speed handpiece (NSK, Nakanishi International, Japan) with stainless steel round burs and excavators. After the caries excavation during an initial examination using the classical probe and visual assessment, all 415 cavities were classified as caries-free[Figure 1a].
Figure 1.
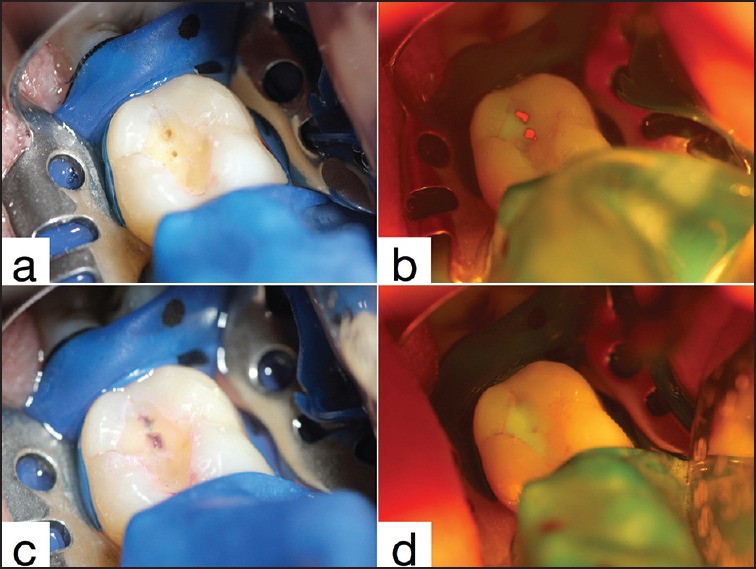
View of a molar, (a) after conventional caries excavation, (b) observed with fluorescence-aided caries excavation, (c) stained with caries detector dye, (d) final cavity
Fluorescence-aided caries excavation stage
After initial cavity preparation, fluorescence violet light (405 nm) was generated using a 100–130-watt xenon discharge lamp (FaceLight, W&H Dentalwerk, Bürmoos GmbH, Austria) to evaluate caries removal. The operator inspected the cavity through a 500 nm red long-pass glass filter, which is compatible with standard corrective goggles, to recognize the orange-red fluorescing areas representing the bacteria-infected dentin surfaces [Figure 1b]. Before CDD application, the results regarding the presence or absence of caries were collected from the FACE by light stage and recorded.
Caries detector dye stage
Subsequently, the teeth were dried briefly by using compressed air and evaluated using a CDD method without performing any operative procedures. Caries detection dye (Caries Detector, Kuraray, Osaka, Japan) was applied to the cavities for 10 s each, and then the cavities were rinsed with water for 10 s, and dried again using compressed air [Figure 1c]. Dentin surfaces that retained stain and stainless areas were recorded [Table 1].
Table 1.
Visual assessment scale for diagnosing caries excavation efficiency
Finally, all the remaining carious areas that were diagnosed using both methods were removed before the final restoration procedure and re-checked [Figure 1d]. All the acquired data were descriptively analyzed. The mean, standard deviation, and 95% confidence intervals were calculated for quantitative variables, and the frequencies were calculated for qualitative variables. Descriptive and explorative statistical analyses were performed using SPSS 17.0 (IBM SPSS Statistics, Chicago, IL, USA). While the Chi-square test was used to compare the mean values of both FACE and dye applications, the evaluation of the effectiveness of each diagnostic method was performed using the Wilcoxon 2 related sample test.
RESULTS
The results of the FACE method and caries detection dye method were compared with the conventional visual assessment and tactile probing method to calculate the sensitivity, specificity, and accuracy of the various caries diagnostic techniques. Furthermore, the obtained values for different caries diagnostic techniques were compared with each other [Table 2].
Table 2.
Percentage and difference (95% confidence interval) in sensitivity and specificity for each diagnostic meth

In total, 273 patients with 451 Black II (OM/OD) cavities (1.65 ± 0.52 teeth per patient) with caries lesions in molar and premolar teeth that were scored according to the International Caries Assessment and Detection System were examined. Of the 451 teeth, 36 teeth were excluded from the study due to pulpal exposure. Although the visual assessment yielded no caries lesions after cavity preparation and excavation, the FACE by the light method and the CDD method found no caries in 149 teeth (35.9%) [Table 3]. In 237 cases (57.2%), the FACE by light method detected remaining carious areas or partially removed caries, while CCD could not stain the carious areas (P < 0.05) of 94 cases (22.6%) that the FACE by light method diagnosed as partially excavated caries. In addition, CDD stained demineralized dentin areas close to the pulp chamber [Figure 2] in 28 cavities (6.7%) that had been diagnosed as sound using the FACE by the light method.
Table 3.
Number of patients and cases caries detected in each diagnostic method
Figure 2.
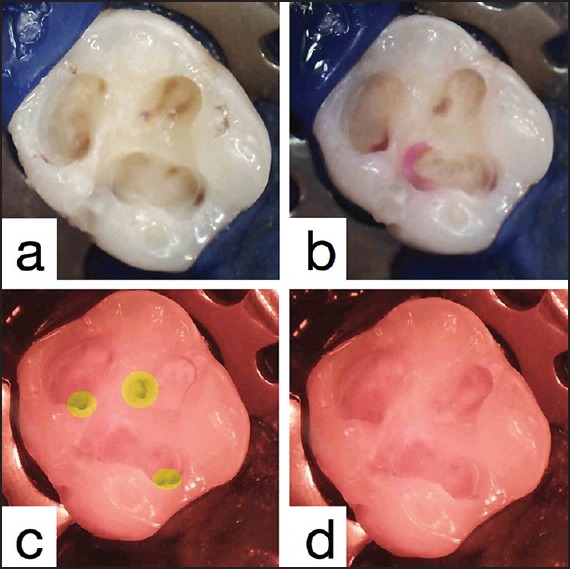
Intraoral camera (with 500 nm red-filter) view of a molar, (a) after excavation, (b) false-stained circumpulpal areas, (c and d) diagnosed with fluorescence-aided caries excavation
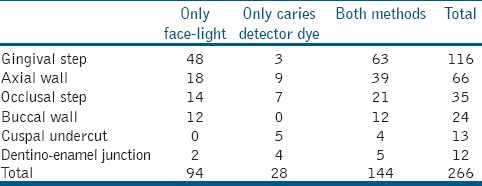
The locations of unexcavated and still affected areas are displayed in Table 4. The most common areas left insufficiently excavated during the cavity preparation stage that were detected by one of the two above-mentioned methods were gingival steps (27.8%) and axial walls (14.7%) (P < 0.05). The differences between the buccal wall, occlusal step, cuspal undercuts, and dentino-enamel junction (DEJ) were statistically insignificant (P > 0.05) (Tables 3 and 4).
Table 4.
Common localizations diagnosed with diagnostic methods where caries removal uncompleted
DISCUSSION
Most clinicians still rely on radiographs, exploration, and visual examination for caries detection. The development of noninvasive techniques and instruments that can detect early demineralization on or beneath the enamel surface is one of the desirable aims of dental researchers.[10,11,12] Although promoting the detection of noncavitated carious lesions has become an increasing focus, the irony is that these lesions could be detected only at the cavitation stage in most clinical settings.[13] While making dentinal cavities, clinicians frequently do not know where to stop the caries excavation process.
Various methods that have been used previously to guide the checkpoint for stopping caries excavation include the following: The use of CDDs and the use of laser fluorescence light.[14] In a review article, Ganter et al. emphasized that although CDDs are produced to aid the dentist in the differentiation of infected/affected dentin, these dyes are not specific or reliable for infected dentin detection.[15] The literature has also revealed that these dyes frequently stain the circumpulpal dentin or DEJ, leading to the unnecessary removal of sound tooth structures.[16] Although the use of chemo-mechanical methods for the removal of the caries is increasing, these systems are much more time consuming and misguiding than conventional systems.[17]
FACE has also been used previously[7,10,17] Lennon et al. examined FACE, CDDs, and conventional caries excavation in primary teeth and concluded that excavation using FACE is more effective than conventional excavation and dye usage in the removal of the infected primary dentin.[11] In another study by Lennon et al., the excavation results using FACE were found to be similar to conventional excavation and superior to CDDs and chemo-mechanical excavation; however, these FACE procedures required a significantly shorter excavation time compared to the time required for conventional excavation.[18] FACE by light is a fluorescence-aided diagnosing system that is based on illustrating the metabolic products that bacteria (porphyrins) left behind in caries-infected dentine with different fluorescent colors. This system employs the principle that the fluorescence signals from the dental tissues can be used for caries detection and excavation by differentiating between infected and affected dentin. da Silva et al. demonstrated that caries removal using the FACE method is significantly less painful compared to the conventional method and reduces the risk of pulpal exposure due to unnecessary removal of sound dentin tissues.[19]
Literature analyses also revealed that manual excavation could not succeed in removing all carious dentin from cavities, particularly at specific localization such as gingival margins and axial walls.[20,21] Determining the complete removal of carious dentin via color (visual criteria) and hardness (tactile criteria) could lead to the unnecessary excavation of sound dentin tissues or to insufficient cavity excavation.[22] In addition, caries excavation with conventional methods using steel, tungsten or polymeric burs leads to smear layer formation, and by this means, nonspecific detector dyes could possibly cause unintentional staining of the smear layer.[23]
Significant differences were observed between the results of the tactile examination and CDD and between the results of the tactile examination and the FACE method. Regardless, CDD stained the axial and pulpal surfaces of the carious dentin located by the FACE method. The high frequency of staining on such dentin surfaces close to the pulpal chamber found in this study may be related to the inherent disadvantages of CDDs in differentiating the less mineralized but sound circumpulpal dentin and enamel-dentin junction, which is consistent with the results of a study by Gugnani et al.[24] In addition, FACE is based on detecting fluorescence caused by bacterial products in carious tooth tissues and does not rely on measuring the mineral content of the tooth, thus discriminating carious dentin during or after cavity preparation.[24] Therefore, FACE method analysis indicated that the challenging areas where the caries are hard to access and remove such as gingival steps were the most common surfaces misevaluated as caries-free using conventional and dye application methods; this finding correlated with those results of the study conducted by Neves Ade et al.[25]
CONCLUSION
This study results showed that the incidence of residual caries after evaluation with FACE was significantly less than those for conventional visual assessment and detector dye application. Therefore, the hypothesis could be accepted for the comparison of FACE with conventional excavation but could not be proven for the comparison with CDD. The findings in this study reveal that FACE is an efficient, clinically applicable, and uncomplicated method for diagnosing sound and carious dentin.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Gimenez T, Braga MM, Raggio DP, Deery C, Ricketts DN, Mendes FM. Fluorescence-based methods for detecting caries lesions: Systematic review, meta-analysis and sources of heterogeneity. PLoS One. 2013;8:e60421. doi: 10.1371/journal.pone.0060421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Frencken JE, Peters MC, Manton DJ, Leal SC, Gordan VV, Eden E. Minimal intervention dentistry for managing dental caries - A review: Report of a FDI task group. Int Dent J. 2012;62:223–43. doi: 10.1111/idj.12007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ismail AI. Visual and visuo-tactile detection of dental caries. J Dent Res. 2004;83:C56–66. doi: 10.1177/154405910408301s12. [DOI] [PubMed] [Google Scholar]
- 4.Neuhaus KW, Ellwood R, Lussi A, Pitts NB. Traditional lesion detection aids. Monogr Oral Sci. 2009;21:42–51. doi: 10.1159/000224211. [DOI] [PubMed] [Google Scholar]
- 5.Thomas CC, Land MF, Albin-Wilson SM, Stewart GP. Caries detection accuracy by multiple clinicians and techniques. Gen Dent. 2000;48:334–8. [PubMed] [Google Scholar]
- 6.Tak O, Usumez A. Diffusion of HEMA through human carious and non-carious dentin in vitro. J Prosthodont. 2013;22:184–9. doi: 10.1111/j.1532-849X.2012.00935.x. [DOI] [PubMed] [Google Scholar]
- 7.Rechmann P, Rechmann BM, Featherstone JD. Caries detection using light-based diagnostic tools. Compend Contin Educ Dent. 2012;33:582–4, 586, 588. [PubMed] [Google Scholar]
- 8.Diniz MB, Boldieri T, Rodrigues JA, Santos-Pinto L, Lussi A, Cordeiro RC. The performance of conventional and fluorescence-based methods for occlusal caries detection: An in vivo study with histologic validation. J Am Dent Assoc. 2012;143:339–50. doi: 10.14219/jada.archive.2012.0176. [DOI] [PubMed] [Google Scholar]
- 9.Lennon AM, Buchalla W, Brune L, Zimmermann O, Gross U, Attin T. The ability of selected oral microorganisms to emit red fluorescence. Caries Res. 2006;40:2–5. doi: 10.1159/000088898. [DOI] [PubMed] [Google Scholar]
- 10.Terrer E, Koubi S, Dionne A, Weisrock G, Sarraquigne C, Mazuir A, et al. A new concept in restorative dentistry: Light-induced fluorescence evaluator for diagnosis and treatment. Part 1: Diagnosis and treatment of initial occlusal caries. J Contemp Dent Pract. 2009;10:E086–94. [PubMed] [Google Scholar]
- 11.Lennon AM, Attin T, Buchalla W. Quantity of remaining bacteria and cavity size after excavation with FACE, caries detector dye and conventional excavation in vitro. Oper Dent. 2007;32:236–41. doi: 10.2341/06-64. [DOI] [PubMed] [Google Scholar]
- 12.Javaheri M, Maleki-Kambakhsh S, Etemad-Moghadam SH. Efficacy of two caries detector dyes in the diagnosis of dental caries. J Dent (Tehran) 2010;7:71–6. [PMC free article] [PubMed] [Google Scholar]
- 13.Matos R, Novaes TF, Braga MM, Siqueira WL, Duarte DA, Mendes FM. Clinical performance of two fluorescence-based methods in detecting occlusal caries lesions in primary teeth. Caries Res. 2011;45:294–302. doi: 10.1159/000328673. [DOI] [PubMed] [Google Scholar]
- 14.Meller C, Heyduck C, Tranaeus S, Splieth C. A new in vivo method for measuring caries activity using quantitative light-induced fluorescence. Caries Res. 2006;40:90–6. doi: 10.1159/000091053. [DOI] [PubMed] [Google Scholar]
- 15.Ganter P, Al-Ahmad A, Wrbas KT, Hellwig E, Altenburger MJ. The use of computer-assisted FACE for minimal-invasive caries excavation. Clin Oral Investig. 2014;18:745–51. doi: 10.1007/s00784-013-1022-3. [DOI] [PubMed] [Google Scholar]
- 16.Celiberti P, Leamari VM, Imparato JC, Braga MM, Mendes FM. In vitro ability of a laser fluorescence device in quantifying approximal caries lesions in primary molars. J Dent. 2010;38:666–70. doi: 10.1016/j.jdent.2010.05.005. [DOI] [PubMed] [Google Scholar]
- 17.de Almeida Neves A, Coutinho E, Cardoso MV, Lambrechts P, Van Meerbeek B. Current concepts and techniques for caries excavation and adhesion to residual dentin. J Adhes Dent. 2011;13:7–22. doi: 10.3290/j.jad.a18443. [DOI] [PubMed] [Google Scholar]
- 18.Lennon AM, Attin T, Martens S, Buchalla W. Fluorescence-aided caries excavation (FACE), caries detector, and conventional caries excavation in primary teeth. Pediatr Dent. 2009;31:316–9. [PubMed] [Google Scholar]
- 19.da Silva RP, Assaf AV, Pereira SM, Mialhe FL, Ambrosano GM, Meneghim Mde C, et al. Validity of caries-detection methods under epidemiological setting. Am J Dent. 2011;24:363–6. [PubMed] [Google Scholar]
- 20.Nordbø H, Leirskar J, von der Fehr FR. Saucer-shaped cavity preparations for posterior approximal resin composite restorations: Observations up to 10 years. Quintessence Int. 1998;29:5–11. [PubMed] [Google Scholar]
- 21.Sánchez CC. Diagnosing incipient caries lesions. Is this the future for dentistry? Rev ADM. 2010;67:13–20. [Google Scholar]
- 22.Gurbuz T, Yilmaz Y, Sengul F. Performance of laser fluorescence for residual caries detection in primary teeth. Eur J Dent. 2008;2:176–84. [PMC free article] [PubMed] [Google Scholar]
- 23.Otake S. The influence of the difference of caries detective methods on the bond strength for caries affected root canal dentin. Kokubyo Gakkai Zasshi. 2010;77:20–6. [PubMed] [Google Scholar]
- 24.Gugnani N, Pandit I, Srivastava N, Gupta M, Gugnani S. Light induced fluorescence evaluation: A novel concept for caries diagnosis and excavation. J Conserv Dent. 2011;14:418–22. doi: 10.4103/0972-0707.87216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Neves Ade A, Coutinho E, De Munck J, Van Meerbeek B. Caries-removal effectiveness and minimal-invasiveness potential of caries-excavation techniques: A micro-CT investigation. J Dent. 2011;39:154–62. doi: 10.1016/j.jdent.2010.11.006. [DOI] [PubMed] [Google Scholar]