

Abstract
Aim:
This study aims to evaluate and compare microleakage at the occlusal wall and cervical wall in Class II cavities restored with one SonicFill Bulk Fill composite and two conventional Bulk Fill composites.
Materials and Methods:
Thirty freshly extracted teeth were divided into three groups of 10 teeth each. Standardized Class II cavities were made on the mesial and distal surfaces of each tooth and restored using SonicFill Bulk Fill composite and two conventional Bulk Fill composites, Tetric Evo Ceram, and X-tra fil. After storage, thermocycling and immersion in 0.6% rhodamine dye solution specimens were sectioned and evaluated for microleakage at the occlusal and cervical walls using confocal microscope.
Statistical Analysis Used:
Kruskal-Wallis test, Wilcoxon Signed-Rank test and Mann-Whitney U-test.
Results:
The results demonstrated that in the occlusal wall and cervical wall, SonicFill Bulk Fill composite, showed significantly less marginal microleakage than the other groups.
Conclusion:
Based on the results of this study, SonicFill Bulk Fill composite showed less microleakage than the other conventional Bulk Fill composites.
Keywords: Bulk Fill composites, Class II restorations, confocal microscope, marginal microleakage, rhodamine dye, SonicFill Bulk Fill composite
INTRODUCTION
Composites were introduced in the 1960's and since then have undergone a lot of research and development refinement in these materials led to the development of microhybrid composite, with mean particle sizes in the 0.6–0.7 micrometers range.[1]
The technique involved in placing posterior composite presents many challenges.[1]
The restoration of the large Class II mesial-occlusal-distal restorations with Resin Bonded Composites materials is time consuming, in terms of placement, light-curing each increment, and the operator time required for separate etching, priming, and bonding techniques.[2]
Despite having good physical properties, the main shortcomings of composite resin materials are polymerization shrinkage and polymerization stress resulting in internal microcracks within the bulk of the material; separation of the bonding agent from the cavity wall with resultant gap formation, marginal microleakage and the postoperative sensitivity; enamel microcracks; marginal staining; wear; discoloration; lower fracture resistance; recurrent caries; and deformation of tooth.[1,3,4,5,6,7,8]
Microleakage is considered to be a major factor influencing the longevity of dental restorations. The decrease of the polymerization shrinkage and consequent microleakage, can be obtained by an oblique layering technique with increments or cavity designs with a low C-factor.[1,9,10,11]
On the other hand, some changes in restorative materials, made in the past, such as modified fillers and composite materials have improved performance of the resins.[7,8,12]
Bulk Fill composites possess specific characteristics, including enhanced flowability to achieve consistent adaptation to the cavity preparation. Elasticity and low polymerization shrinkage stress reduce microleakage, postoperative sensitivity, and secondary caries. Improved depth of cure of at least 4 mm eliminates the need for layering.[13]
The recent introduction of the SonicFill (Kerr corp. USA) combines the attributes of a low viscosity composite and a universal composite. By activating the composite with sonic energy, it is possible to fill the cavity and adapt the low viscosity material easily, and then compact and model it while the composite changes its consistency until it reaches a higher viscosity.
As per the manufacturer, the advantages are reduced working time and polymerization shrinkage, better adaptation to cavity walls, and ease of use.[14]
The aim of this study is to evaluate the microleakage in Bulk Fill composites using confocal microscopy.
MATERIALS AND METHODS
Thirty human permanent mandibular first molars with no crack, decay, fracture, abrasion, previous restorations, or structural deformities, which are periodontally compromised were collected and stored in normal saline. After removing residual tissue tags, the specimens were cleaned with pumice. Sixty standardized Class II cavities were made on the mesial and distal surfaces of each tooth. Each cavity was prepared with a carbide bur (number 245). For every five preparations a new bur was used. Final dimension of the cavity showed 2 mm occlusal extension, 3 mm buccolingual extension, gingival seat was placed at the cementoenamel junction (CEJ).[1]
The cavities were cleaned using pumice paste and then were rinsed with a water spray and gently dried. Each specimen was mounted with adjacent teeth for placement of Tofflemire matrix which allowed building up of the proximal wall.
All the prepared cavity surfaces were dried with oil free compressed air, etched with 37% phosphoric acid for 15 s and then rinsed, and dried. Adper single bond 2 (3M) bonding agent was applied to the etched surface, gently dried, and cured. The teeth were then randomly divided into three groups of 10 each. Group I: SonicFill Bulk Fill composite (Kerr/Sybron Orange, CA), Group II: Tetric Evo Ceram Bulk Fill composite (Ivoclar Vivadent, Schaan, Liechtenstein), Group III: X-tra fill Packable Posterior Bulk Fill composite (Vocco products, Germany). The specimens in each group were restored with the corresponding Bulk Fill composite and cured for 20 s according to manufacturer's instructions.
The specimens were stored at 100% relative humidity at 37°C for 24 h and were then submitted to 1000 thermal cycles at 5°C and 55°C with a dwell time of 1-min at each temperature. The specimens were then covered with two layers of nail varnish, except the resin composite restoration and 1 mm area around it, followed by immersion in 0.6% aqueous rhodamine dye for 48 h.[15] The specimens were rinsed and sectioned mesiodistally using hard tissue microtome.[1]
The microleakage was measured using confocal microscopy at ×10 magnification (Confocal Fluorescence Imaging Microscope, Leica TCS-SP5, and DM 6000-CFS) in the fluorescent mode. Approximately, six photographs of each specimen were taken to obtain the full perimeter of the restoration. With a digital scale (Snagit digital scale), the width of interface between restoration and tooth surface was calculated.[15]
The microleakage scoring was done using the method, as per Radhika et al.[1]
Scoring for dye penetration for marginal microleakage on the occlusal wall
0 - No dye penetration.
1 - Dye penetration into half extension.
2 - Dye penetration more than half.
3 - Dye penetration into the pulpal wall.
Scoring for dye penetration for marginal microleakage on the cervical wall
0 - No dye penetration.
1 - Dye penetration into half extension of the cervical wall.
2 - Dye penetration into more than half or complete extension of the cervical wall.
3 - Dye penetration into the cervical and axial walls towards the pulp.
RESULTS
Confidence Interval will be within the interval of 95%.
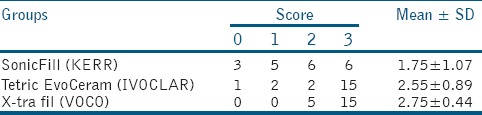
When the three groups were compared for microleakage along occlusal wall and cervical wall using Kruskal-Wallis test there was significant difference among the groups with P = 0.0455 and 0.0071, respectively [Tables 1 and 2, Graphs 1 and 2].
Table 1.
Inter group comparison at occlusal level using Kruskal-Wallis test
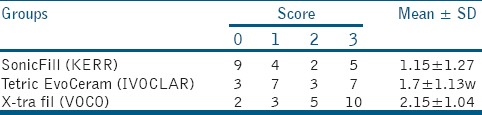
Table 2.
Inter group comparison at cervical level using Kruskal-Wallis test
Graph 1.
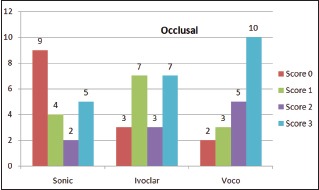
Microleakage along occlusal wall
Graph 2.
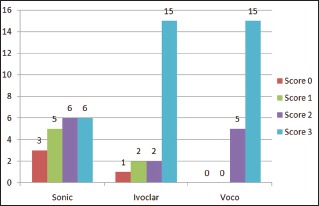
Microleakage along cervical wall
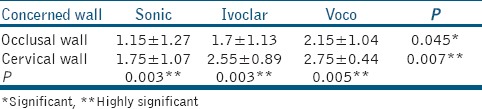
When microleakage was compared between occlusal wall and cervical wall using Wilcoxon Signed-Rank test, cervical wall showed more microleakage than occlusal wall in all the groups with P = 0.003, 0.003, and 0.005 respectively [Table 3 and Graph 3].
Table 3.
Comparison between occlusal and cervical wall using Wilcoxon Signed-Rank test
Graph 3.
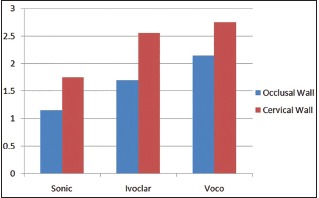
Comparision of microleakage between occlusal and cervical walls
When pair wise comparison was done along occlusal wall using Mann–Whitney U-test, Sonic - Voco showed significant result (P = 0.05), while Sonic - Ivoclar and Ivoclar - Voco results were not significant (P = 0.0708 and 0.115, respectively).
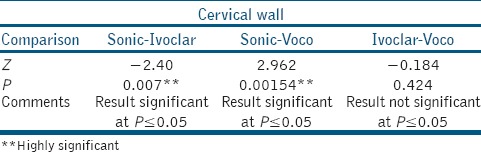
When pair wise comparison was done along cervical wall using Mann-Whitney U-test, Sonic - Ivoclar and Sonic - Voco showed significant result (P = 0.0070 and 0.00154, respectively), while between Ivoclar - Voco the result was not significant (P = 0.424) [Tables 4 and 5].
Table 4.
Pair wise comparison at occlusal level using Mann-Whitney U-test
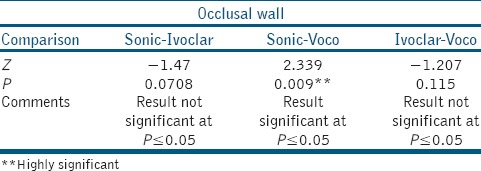
Table 5.
Pair wise comparison at cervical level using Mann-Whitney U-test
DICUSSION
Marginal integrity is essential to increase the longevity of any restoration.[16] This integrity is compromised, when microleakage occurs resulting from polymerization shrinkage. Polymerization shrinkage is the most common cause of failure of direct posterior composite restorations. Polymerization shrinkage is dependent on various aspects such as the boundary conditions, the material's formulation, and the amount of material in the polymerization reaction.[17] This phenomenon occurs because monomer molecules are converted into a polymer network and therefore, exchanges Van der Walls spaces into covalent bond spaces, creating contraction stresses in the resin composite leading to microleakage.[1]
Different resin composites have different formulations and consequently different polymerization shrinkage. Many studies have suggested the use of an incremental layering technique to reduce this shrinkage.[1,17,18] Nowadays, traditional placement techniques for composite resins include this technique.[17] Most practitioners recommend placing composites in 2 mm increments. However, every dentist who places posterior composite resins will prefer a composite material that can be used using a Bulk Fill technique.
The magnitude of the stress induced during polymerization shrinkage also depends upon other factors, such as the configuration factor (C-factor) of the cavity and also the effect of light-curing mode.[19]
In our study, the cavities were of the same dimensions, the same C-factor, and the light-curing mode was the same for all the restoration specimens.
In this study, we used SonicFill Bulk Fill composite and two conventional Bulk Fill composites. SonicFill TM was introduced in the dental market in 2010 and it combines the properties of a flow able composite with those of a universal composite.
The present study measured microleakage using confocal microscopy at ×10 magnification. Confocal laser scanning microscopy (CLSM) is a technique used for visualizing subsurface tissue characteristics. An advantage of this technique is the use of lens focus which can focus a few microns beneath the observed surface, thus avoiding the spread of stain due to specimen sectioning and also avoids polishing artifacts. Further observation of CLSM is made possible by elimination of scattered, reflected, and fluorescent light from planes other than the plane from which the image is created, the focal plane.[20] The laser scanning microscope scans the sample, sequentially point by point and line by line and assembles the pixel information into one image.[21]
All three composites, when compared for microleakage at occlusal and cervical wall, had a significant difference with P = 0.0455 and 0.0071 respectively.
When microleakage was compared along the occlusal wall and cervical wall, the cervical wall showed more microleakage than the occlusal wall in all the groups. SonicFill (P = 0.003), Tetric Evo Ceram (P = 0.003), X-tra fil (P = 0.005).
Results of this study showed that there was statistical significance in the microleakage with occlusal wall showing lesser microleakage than cervical wall in all the three composites. This can be attributed to the fact that the gingival seat of a Class II cavity, when prepared near the CEJ, is made up of dentin and cementum. Bonding to dentin has always been poor compared to enamel because of the morphological, histological, and compositional differences between the enamel and dentin. Enamel is more mineralized than dentin, having an inorganic content of 96% by weight, whereas the inorganic content of dentin is approximately 70% by weight, 18% organic material, and 12% water. Bonding to dentin is a challenge due to higher water and organic content. Cementum's organic phase consists of coarser collagen fibers than dentin; hence, a weaker bonding can be expected.[22]
Another factor, which can affect the marginal microleakage is the distance between the light-curing tip and the resin surface. When the distance between the light-curing tip and the resin surface is >2 mm, the light intensity is significantly reduced. This might prevent adequate polymerization of resin composite materials.[23]
Bulk Fill composites have higher filler content and thus have increased mechanical properties. Due to an enhanced translucency and by incorporating a photoactive group in the methacrylate resin, polymerization kinetics are claimed to be better controlled.[24]
In our study, there was significant difference in microleakage among the three groups. When pair wise comparison was done along occlusal wall and cervical wall using Mann-Whitney U-test, along occlusal wall Sonic - Voco showed significant result (P ≤ 0.05), while Sonic - Ivoclar and Ivoclar - Voco results were not significant (P = 0.0708 and 0.115, respectively). Along cervical wall Sonic - Ivoclar and Sonic - Voco showed significant result (P = 0.0070 and 0.00154 respectively), while between Ivoclar - Voco the result was not significant (P = 0.424).
Oscillation energy temporarily increases flowability of SonicFill to achieve precise filling of cavities. An advantage of this composite is the rapid placement through a single increment up to 5 mm due to reduced polymerization shrinkage, thereby reducing working time.[25]
This may be attributed to the ultra-sonic activation in SonicFill, where it incorporates a highly filled proprietary resin with special modifiers that react to sonic energy. As sonic energy is applied through the hand piece, the modifier causes the viscosity to drop (up to 87%), increasing the flowability of the composite enabling quick placement and precise adaptation to the cavity walls. When the sonic energy is stopped, the composite returns to a more viscous, nonslumping state that is perfect for carving and contouring.[25]
As voids may be present in the mass of the material future studies should also aim at evaluating the voids formed in Bulk Fill composites.
CONCLUSION
Based on the limitations of this study, it may be concluded that in Class II restorations, microleakage is observed regardless of the Bulk Fill composite used and Sonic Bulk Fill composite shows lesser microleakage at both cervical and occlusal walls.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Radhika M, Sajjan GS, Kumaraswamy BN, Mittal N. Effect of different placement techniques on marginal microleakage of deep class-II cavities restored with two composite resin formulations. J Conserv Dent. 2010;13:9–15. doi: 10.4103/0972-0707.62633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent. 2012;40:500–5. doi: 10.1016/j.jdent.2012.02.015. [DOI] [PubMed] [Google Scholar]
- 3.Zimmerli B, Strub M, Jeger F, Stadler O, Lussi A. Composite materials: Composition, properties and clinical applications. A literature review. Schweiz Monatsschr Zahnmed. 2010;120:972–86. [PubMed] [Google Scholar]
- 4.Ben-Amar A, Slutzky H, Matalon S. The influence of 2 condensation techniques on the marginal seal of packable resin composite restorations. Quintessence Int. 2007;38:423–8. [PubMed] [Google Scholar]
- 5.Vyver P. Clinical application of a new flowable base material for direct and indirect restorations. Int Dent S Afr. 2011;12:18–27. [Google Scholar]
- 6.Burke FJ, Crisp RJ, James A, Mackenzie L, Pal A, Sands P, et al. Two year clinical evaluation of a low-shrink resin composite material in UK general dental practices. Dent Mater. 2011;27:622–30. doi: 10.1016/j.dental.2011.02.012. [DOI] [PubMed] [Google Scholar]
- 7.Mahmoud SH, Al-Wakeel Eel S. Marginal adaptation of ormocer-, silorane-, and methacrylate-based composite restorative systems bonded to dentin cavities after water storage. Quintessence Int. 2011;42:e131–9. [PubMed] [Google Scholar]
- 8.Hickel R, Manhart J. Longevity of restorations in posterior teeth and reasons for failure. J Adhes Dent. 2001;3:45–64. [PubMed] [Google Scholar]
- 9.Vicente A, Ortiz AJ, Bravo LA. Microleakage beneath brackets bonded with flowable materials: Effect of thermocycling. Eur J Orthod. 2009;31:390–6. doi: 10.1093/ejo/cjn126. [DOI] [PubMed] [Google Scholar]
- 10.Gogna R, Jagadis S, Shashikal K. A comparative in vitro study of microleakage by a radioactive isotope and compressive strength of three nanofilled composite resin restorations. J Conserv Dent. 2011;14:128–31. doi: 10.4103/0972-0707.82609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Helvatjoglu-Antoniades M, Kalinderis K, Pedulu L, Papadogiannis Y. The effect of pulse activation on microleakage of a ‘packable’ composite resin and two ‘ormocers’. J Oral Rehabil. 2004;31:1068–74. doi: 10.1111/j.1365-2842.2004.01337.x. [DOI] [PubMed] [Google Scholar]
- 12.Ernst CP, Brandenbusch M, Meyer G, Canbek K, Gottschalk F, Willershausen B. Two-year clinical performance of a nanofiller vs a fine-particle hybrid resin composite. Clin Oral Investig. 2006;10:119–25. doi: 10.1007/s00784-006-0041-8. [DOI] [PubMed] [Google Scholar]
- 13.Michael R Sesemann. www.oralhealthgroup.com .
- 14.Giachetti L. A new method for direct composite restoration of the posterior teeth. J Dental Tribune Middle East and African edition - 2014 [Google Scholar]
- 15.Usha H, Kumari A, Mehta D, Kaiwar A, Jain N. Comparing microleakage and layering methods of silorane-based resin composite in class V cavities using confocal microscopy: An in vitro study. J Conserv Dent. 2011;14:164–8. doi: 10.4103/0972-0707.82624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Majety KK, Pujar M. In vitro evaluation of microleakage of class II packable composite resin restorations using flowable composite and resin modified glass ionomers as intermediate layers. J Conserv Dent. 2011;14:414–7. doi: 10.4103/0972-0707.87215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Schneider LF, Cavalcante LM, Silikas N. Shrinkage stresses generated during resin-composite applications: A review. J Dent Biomech 2010. 2010 doi: 10.4061/2010/131630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Roggendorf MJ, Krämer N, Appelt A, Naumann M, Frankenberger R. Marginal quality of flowable 4-mm base vs. conventionally layered resin composite. J Dent. 2011;39:643–7. doi: 10.1016/j.jdent.2011.07.004. [DOI] [PubMed] [Google Scholar]
- 19.Van Ende A, Mine A, De Munck J, Poitevin A, Van Meerbeek B. Bonding of low-shrinking composites in high C-factor cavities. J Dent. 2012;40:295–303. doi: 10.1016/j.jdent.2012.01.004. [DOI] [PubMed] [Google Scholar]
- 20.Minsky M. Memoir on inventing the confocal scanning microscope. J Scan. 1988;10:128–38. [Google Scholar]
- 21.Lopes MB, Consani S, Gonini-Júnior A, Moura SK, McCabe JF. Comparison of microleakage in human and bovine substrates using confocal microscopy. Bull Tokyo Dent Coll. 2009;50:111–6. doi: 10.2209/tdcpublication.50.111. [DOI] [PubMed] [Google Scholar]
- 22.Joseph A, Santhosh L, Hegde J, Panchajanya S, George R. Microleakage evaluation of Silorane-based composite and methacrylate-based composite in class II box preparations using two different layering techniques: An in vitro study. Indian J Dent Res. 2013;24:148. doi: 10.4103/0970-9290.114943. [DOI] [PubMed] [Google Scholar]
- 23.Poskus LT, Placido E, Cardoso PE. Influence of adhesive system and placement technique on microleakage of resin-based composite restorations. J Adhes Dent. 2004;6:227–32. [PubMed] [Google Scholar]
- 24.Van Ende A, De Munck J, Van Landuyt KL, Poitevin A, Peumans M, Van Meerbeek B. Bulk-filling of high C-factor posterior cavities: Effect on adhesion to cavity-bottom dentin. Dent Mater. 2013;29:269–77. doi: 10.1016/j.dental.2012.11.002. [DOI] [PubMed] [Google Scholar]
- 25.Eunice C, Margarida A, João C, Filomena B, Anabela P, Pedro A, et al. 99mTc in the evaluation of microleakage of composite resin restorations with SonicFillTM. An in vitro experimental model. Open J Stomatol. 2012;2:340–7. [Google Scholar]