

Abstract
Objective
A recent study demonstrated that a single 50-minute supplemental session that targeted the behavioral economic mechanisms of substance-free reinforcement and delayed reward discounting (Substance Free Activity Session: SFAS) enhanced the efficacy of a standard alcohol brief motivational intervention (BMI) for college drinkers. The purpose of the current study was to conduct a randomized controlled trial intended to replicate and extend the aforementioned study by focusing on both drug and alcohol misuse and reducing session length in order to enhance dissemination potential.
Method
Participants were 97 college students (58.8% women; 59.8% white/Caucasian & 30.9% African American; M age = 20.01, SD = 2.23) who reported at least one heavy drinking episode in the past month (M = 4.01 episodes). Most participants (62%) reported recent marijuana use (M = 12.22 days of past-month use). After completing a baseline assessment and an individual 30-minute alcohol-focused BMI, participants were randomized to either the 30-minute SFAS session or an education control session.
Results
A series of mixed model intent-to-treat analyses revealed that both groups reported drinking reductions and that participants in the BMI+SFAS group reported fewer days using marijuana at the 6-month follow-up.
Conclusions
These results do not support the incremental efficacy of the briefer SFAS for reducing drinking but suggest that it may improve marijuana outcomes. Future research is needed to identify the ideal length and timing of the SFAS supplement to BMIs.
Keywords: alcohol, marijuana, behavioral economics, motivational interventions, substance-free reinforcement
To date, the most promising approach for reducing risky drinking in college students is brief motivational interventions (BMIs) that include personalized feedback and motivational interviewing (Cronce & Larimer, 2011). Despite the fact that BMIs are consistently associated with significant drinking reductions relative to control conditions, they typically yield only small to moderate effect size reductions (Carey et al., 2007; Larimer, & Cronce, 2011; Moreira et al., 2009). Additionally, few studies have examined this approach with drug use outcomes (Lee, Neighbors, Kilmer, & Larimer, 2010; Lee et al., 2013; White e al., 2006) or developed novel treatment elements to enhance standard BMIs (DeMartini, Fucito & O’Malley, 2015; Turrisi et al., 2012).
Behavioral economic theory posits that substance use is influenced by constraints on access to drugs and the availability and value of alternative substance-free sources of reinforcement (Bickel, Johnson, Koffarnus, MacKillop & Murphy, 2014). Whereas substance use offers immediate rewards, many substance-free activities, such as health or career/education-promoting activities, are associated with delayed benefits, and may not be highly enjoyable in the moment (Murphy et al., 2006). The proportion of resource allocation and enjoyment associated with substances compared to substance-free reinforcers has been used to quantify the reinforcing efficacy of substances relative to other reinforcers in the individual’s environment (Heinz, Lilje, Kassel, & de Wit, 2012). Individuals with few rewarding alternatives to drinking are less likely to respond to traditional BMIs, and those who reduce their drinking following a BMI are likely to increase their engagement in some categories of substance-free activities, including academic activity (Murphy et al., 2005). Behavioral economic research suggests that increasing the salience of delayed rewards associated with substance-free activities can reduce impulsive response patterns and potentially decrease substance use (Hofmeyr, Ainslie, Charlton, & Ross, 2011).
A recent study by Murphy, Dennhardt, Skidmore, Borsari, Barnett et al. (2012) combined a 50–60 minute standard alcohol BMI and a 50–60 minute behavioral economic Substance-Free Activity Session (SFAS) delivered one-week after the BMI. The SFAS is delivered in a MI style and targets the behavioral economic mechanisms of substance-free reinforcement and delayed reward discounting by providing personalized feedback on patterns of substance-related and substance-free activity participation, and potential future rewards associated with substance-free academic and career-related activities, in order to encourage increased participation in academic, community and recreational activities. In comparison to an alcohol BMI plus a relaxation training active control session, the alcohol BMI+SFAS condition was associated with significantly greater reductions in heavy drinking and alcohol related problems at a 6-month follow-up assessment. However, drug use outcomes were not explored, and the addition of a 60-minute session one week after the alcohol BMI poses a significant barrier to dissemination across college campuses. Alcohol and drug use interventions are often delivered opportunistically to large numbers of students who are typically completing the intervention to satisfy an alcohol policy violation mandate and are generally not motivated to pursue treatment outside of what is mandated (Buscemi et al., 2010). At university health centers alone, approximately 57% of patients are at-risk drinkers (Zakletskaia, Wilson & Fleming, 2010) yet many universities lack resources to deliver empirically supported treatments (Nelson, Toomey, Lenk, Erikson, & Winters, 2010). Hence, campuses may be more likely to implement the BMI+SFAS combination if it could be administered in single 60 minute session. Furthermore, studies have suggested that a very brief intervention (10 minutes) can reduce alcohol related outcomes with little advantage of a longer intervention (50 minutes) or adding more of the same material (Barnett, Murphy, Colby, & Monti., 2007; Kulesza, Apperson, Larimer, & Copeland, 2010).
The current study intended to replicate and extend the Murphy et al. (2012) study by targeting both alcohol and drug use and by consolidating the BMI+SFAS sessions into 30-minute segments completed in a single visit (to increase the potential for dissemination). Additionally, to increase generalizability, this study incorporated a more heterogeneous sample of college students rather than just freshmen. We hypothesized that the BMI+SFAS would be associated with greater reductions in drinking and drug use relative to a BMI+Education active control condition.
Method
Participants and Procedure
Consistent with prior studies examining non-treatment seeking college drinkers (Carey, Carey, Maisto, & Henson, 2006) undergraduate students (N=1503) were screened from the university’s psychology subject pool (75.3%), other undergraduate courses (14.4%), and on-campus organizations (10.3%). Students were eligible to participate if they were at least 18 years old and reported one or more heavy drinking episodes (5/4 drinks on one occasion for a male/female) in the past month. Of those screened, 224 met the eligibility criteria and were contacted to participate in the study (See figure 1). Our final sample was representative of the campus and included 97 undergraduate students (59% female; 41% male). The sample was ethnically diverse; 60% identified as European American and 31% identified as African American. Baseline sample characteristics are presented in Table 1.
Figure 1.
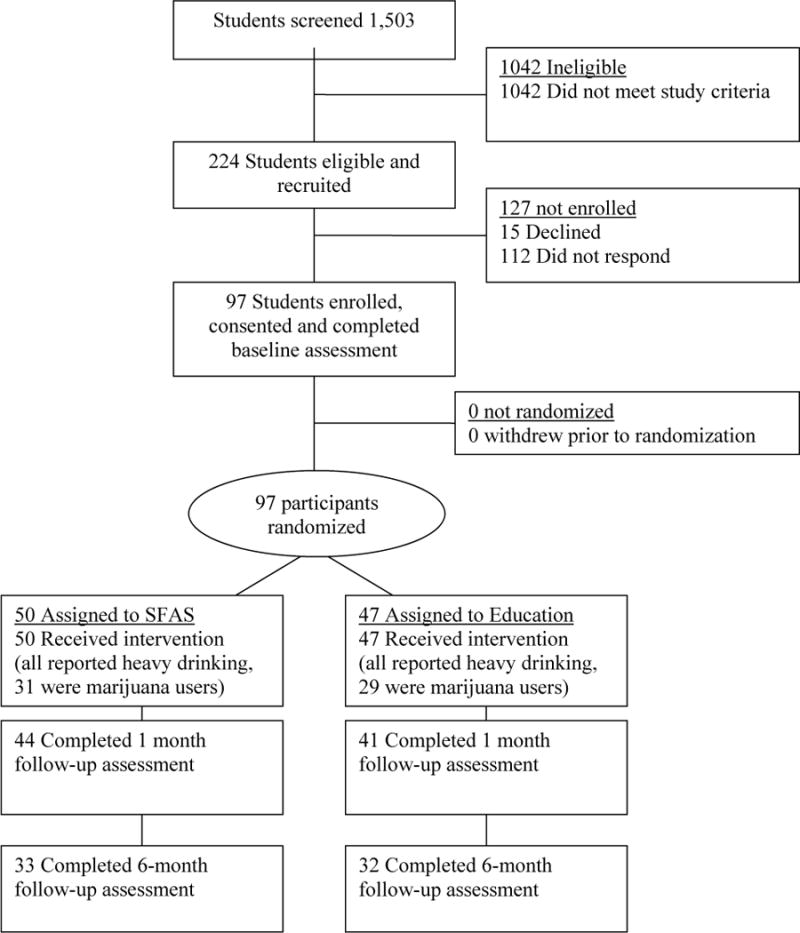
Flow of Participants through Each Stage of Study.
Table 1.
Baseline sample demographics
| SFAS | Education | t-statistic (df) | χ2 | |
|---|---|---|---|---|
| N | 50 | 47 | ||
| Age – M (SD) | 20.14 (2.32) | 20.06 (2.16) | t (95) = 0.17 | |
| Sex – (%) | .487 | |||
| Male | 21 (42.0) | 19 (40.4) | ||
| Female | 29 (58.0) | 28 (59.6) | ||
| Race/Ethnicity1 – (%) | ||||
| White or Caucasian | 30 (60.0) | 28 (59.6) | ||
| Black or African-American | 15 (30.0) | 15 (31.9) | ||
| Other | 5 (10.0) | 4 (8.5) | ||
| Class1 – (%) | ||||
| Freshman | 28 (57.1) | 24 (51.1) | ||
| Sophomore | 6 (12.2) | 10 (21.3) | ||
| Junior | 5 (10.2) | 9 (19.1) | ||
| Senior | 8 (16.3) | 4 (8.5) | ||
| Other2 | 2 (4.1) | 0 (0) | ||
| Drinks Per Week | 15.34 (9.90) | 11.53 (8.97) | t (95) = 2.28* | |
| Alcohol Related Problems | 11.72 (8.60) | 10.89 (7.89) | t (95) = .492 | |
| Past month Marijuana Use Days† | 12.45 (10.74) | 11.97 (10.77) | t (58) = .661 |
p < .05
p < .01
Mean and SD are only for those who reported baseline marijuana use.
Note.
Fisher’s exact test was used for the Race/Ethnicity and Class variables due to < 5 expected frequencies in at least one cell, therefore they do not have a statistic to report in the last column.
Participants categorized as “other” were students who were either in between years (i.e. third semester junior) or those who declined to answer.
All procedures were approved by the University Institutional Review Board. After providing informed consent, participants completed a series of baseline questionnaires and then a 30-minute alcohol and drug-focused BMI. Participants were then randomized to an alcohol/drug education control session or the SFAS. Counselor delivered education (ED) was chosen as an active control for contact time and therapist attention. Because several studies have found differential BMI response as a function of sex (Carey et al., 2007) and because we wanted to ensure representativeness of different ethnicities across conditions, we used a random number generator and stratified by sex and ethnicity. The same clinician delivered both interventions for each participant and the same group of clinicians conducted both BMI+ED and BMI+SFAS interventions. Follow-up assessments occurred 1-month and 6-months following the interventions (See Figure 1). Students recruited from undergraduate courses were given extra-course credit for their participation and other students were provided with a $25 cash payment at baseline and $10 for each completed follow-up. Follow-up assessments occurred in the lab at 1-month following the interventions to assess relatively short-term changes in the outcome variables, and again at 6-months to evaluate any long-term changes. For participants who were unable to attend the follow-up sessions (N=35), data was collected via a web survey from the secure site www.qualtrics.com.
Measures
Alcohol and Drug Use
The Daily Drinking Questionnaire (DDQ) was used to assess the total number of standard drinks consumed each day during a typical week in the past month (Collins, Parks, & Marlatt, 1985). Participants also reported on their number of heavy drinking episodes in the past month. Drug use was assessed by asking participants how many days they used illicit drugs (e.g., marijuana, cocaine) and/or prescription medications (e.g., stimulants, opioids) in the past month.
Alcohol Problems
The Young Adult Alcohol Consequences Questionnaire (YAACQ) is a 48-item scale that has been shown to accurately map the continuum of alcohol problem severity among college students (Read, Merrill, Kahler, & Strong, 2007). Participants indicated (yes/no) which items on a list of 48 potential problems they have experienced as a result of their drinking in the past month. Internal consistency for the YAACQ in this study was .91.
Intervention Conditions
Motivational interviewing sessions were conducted by five graduate students in psychology who had completed extensive training and supervision in motivational interviewing and in all three intervention protocols. Treatment manuals were developed for all three interventions to assist with internal validity and treatment integrity. Training included readings, training DVD’s, small group training, individual feedback, and completing at least one complete session role-play for each condition. Due to the inclusion of a diverse sample and the cultural relevance of the sessions, interventionists were also trained in cultural awareness. Clinicians were provided with readings and cases were discussed during supervision. All sessions were audio-taped and weekly group supervision was provided by the faculty advisor who is a licensed clinical psychologist with extensive experience training and supervising brief motivational interventions for substance misuse. In addition, integrity coding was conducted to ensure consistency with protocol in terms of content and motivational interviewing style (described below).
BMI
Following the baseline assessment, participants completed a 25–30 minute BMI that was delivered in an MI style (Miller & Rollnick, 2012). Although drug us was not an inclusion criteria for this study, if a student reported drug use on the baseline assessment, the BMI included information intended to encourage students to reduce both their use of alcohol and other reported drugs used and was explicitly developed for college students with mild to moderate levels of alcohol and/or drug use problems. Drug feedback was only provided to those students who reported use, and they were only given information for the specific drug(s) used. The session began by encouraging the student to talk about their use of alcohol and drugs (e.g., what they like and dislike about alcohol, how their pattern of use has changed over time). They then received personalized feedback on how their drinking and drug use compares to that of other students of their sex and ethnicity, along with information on tolerance, and engaging in risky alcohol and drug use. The clinician discussed the feedback with the student and assisted with goal-setting and provided advice on reducing or eliminating alcohol and drug use if the student indicated he or she was interested.
SFAS
This 25–30 minute session targeted the behavioral economic mechanisms of substance-free reinforcement and delayed reward discounting by encouraging the development of and commitment to academic and career goals. The intervention was personalized based on the student’s report of their interests, activities, career goals, and major, and presented in an MI style. Participants were asked to discuss college and career goals as well as the impact of drinking/drug use on goal progress. Information on the requirements for the student’s stated career goal(s) was presented as well as potential activities in which the student could participate related to these goals (e.g., organizations, internships related to their major/career goals, including minority-specific organizations for minority participants). Participants also received general information regarding financial advantages and other future benefits of graduating college and earning good grades. The session continued with feedback on how the participant currently spent their time and the difference between time spent using substances and time spent in other activities was highlighted and discussed in relation to their goals/values. Participants were also presented with information on coping skills to manage negative affect, which could interfere with goal pursuit. Because discrimination is a significant source of stress for minority students, these students received additional information on coping with discrimination (Broman, 2007). Finally, if the participant was interested, goal-setting was conducted regarding time management, grades, and valued activities. The participant was asked if they would like to reconsider their substance use goals in light of the information presented. In order to accommodate the multiple topics and maintain treatment integrity within the confines of a brief session, although all intervention elements were included in all sessions (and on the personalized feedback sheet created for each participant), consistent with MI style, the clinician selectively focused the discussion based on the participant’s interest and the clinician’s judgment of the particular functional relevance of a given topic to a participant’s goals and their unique patterns of activities and drinking/drug use.
ED
Participants randomized to the 25–30 minute education component were given additional information about alcohol and drugs during an individual meeting with a clinician. A counselor provided detailed (but not personalized) information to every student about the effects of alcohol and other drugs on the brain and nervous system, memory, sexual performance, and other areas of the body. A 5-minute interactive computerized component (Alcohol-101) discussed alcohol’s effects on specific brain areas and then clinicians provided students with a hand-out and discussed how alcohol and other drugs affect various bodily organs and systems (National Geographic Drugs, 2011; National Institute on Drug Abuse, 2011; Virginia Department of Alcoholic Beverage Control, 2003). Participants were invited to ask questions, but the session was primarily didactic.
Evaluation of Internal Validity (treatment integrity)
Approximately 20% of the BMI sessions (n = 19), SFAS (n = 10), and ED sessions (n = 9) were randomly selected and reviewed using a brief intervention adherence protocol commonly used in intervention trials (Murphy et al., 2010/2012a). Each component on the protocol and MI competence was rated as a 0 (Didn’t do it, N/A), 1 (Did it poorly or didn’t do it but should have), 2 (Meets Expectations), or 3 (Above Expectations) by two clinical psychology doctoral students with MI training who were not associated with this project. For the Alcohol MI intervention protocol and MI competence, 100% of the items rated as meeting or exceeding expectations. For the SFAS protocol, 100% of the components rated as meeting or exceeding expectations, with 90% of the MI competence items being rated as a 2 or 3. For the main components of the ED intervention protocol, 100% of the components were rated as meeting or exceeding expectations. Thus, clinicians consistently administered the intervention components and adhered to an MI style when indicated.
Data Analysis Plan
All variables were checked for outliers and deviations from normality prior to analyses. Outlier values greater than 3.29 SDs above the mean on a given variable were changed to one unit greater than the greatest nonoutlier value, and variables that were skewed or kurtotic were transformed using square root and/or log transformations depending on which provided a better correction (Tabachnick & Fidell, 2001). Alcohol-related problems and marijuana use days were log transformed and drinks per week were square root transformed. All transformations used in final analyses resulted in normal distributions except for baseline marijuana use days, which remained slightly kurtotic. Untransformed variables are presented in the tables and figures for interpretational clarity. A series of mixed-model repeated measures analyses (Gueorguieva & Krystal, 2004) were conducted to compare the BMI+ED group and the MI+SFAS group on each of the primary outcome variables at 1-month and 6-month follow-ups. Mixed-effect models (also known as hierarchical linear models or multilevel models; Gueorguieva & Krystal, 2004) provide a flexible framework for repeated measures analyses. Compared to traditional repeated measures analysis of variance (ANOVA), mixed-effect models utilize all available data for each participant to better accommodate for missing data and appropriate for use in an intention-to-treat analysis (Gueorguieva & Krystal, 2004). For each model tested, one of the primary outcome variables served as the dependent variable with sex and ethnicity included as covariates. We included sex as a covariate because several studies have found that college females are more responsive to brief alcohol interventions than college males (Carey et al., 2007; Murphy et al., 2004), and ethnicity due to the varying drinking and drug use patterns among different ethnicities (Cranford, McCabe, & Boyd, 2006). Only participants who reported baseline marijuana use were included in marijuana use outcome analyses. Although the primary analyses used an intent- to-treat approach that modeled missing data, for ease of interpretability, tables and figures report data only for those who completed each follow-up.
Results
Baseline Characteristics
Overall, participants reported consuming an average of 13.49 (SD = 9.60) drinks in a typical week and experiencing a total of 11.32 (SD = 8.23) alcohol-related problems over the past month. Students who reported past-month drug use (n = 67, 69% of the sample) were using on average 14.22 (SD= 13.60) days in the past month. Marijuana was the most commonly used drug with 62% of participants reporting use at least 1 day in the past month at baseline, followed by stimulant medication with 15% reporting past-month use. Because of the high prevalence of marijuana use compared to other drug use, drug use analyses focused only on marijuana outcomes. Students assigned to BMI+SFAS drank significantly more than students assigned to BMI+ED, but there were no other baseline demographic or substance use group differences (See Table 1). Those who were recruited from undergraduate courses reported higher levels of alcohol consumption and marijuana use compared to those recruited via other methods. Although all randomized participants completed the intervention, 12 participants did not complete the one-month follow-up (N = 85, 88% follow-up rate) and 32 participants did not complete the six-month follow-up (N = 65, 67% follow-up rate). The sample size for those who used marijuana at baseline and were included in the marijuana analyses were: SFAS condition (baseline, n = 31, 1-month follow-up, n = 27, and 6-month follow-up, n = 23) and ED condition (baseline, n = 29, 1-month follow-up, n = 25, and 6-month follow-up, n = 21). Follow-up rates did not differ by condition or recruitment method and there were no demographic or baseline drinking or marijuana differences between completers and non-completers.
There was a significant main effect for time on weekly drinking, [F(2, 71.56) = 11.83, p = .000] and alcohol related problems, [F(2, 71.28) = 6.82, p = .002], but no differences between treatment groups. Both conditions were associated with moderate effect size reductions (see Table 2). There was a significant main effect for time for days of marijuana use, [F(2, 44.73) = 6.85, p = .003, and a significant time by condition interaction. Participants in the BMI+SFAS condition used marijuana on significantly fewer days at the 6-month follow-up (M = 6.46) compared to those in the BMI+ED condition (M = 11.38), [F(2, 45.10) = 4.10, p = .023; See figure 2]1. Effect size reductions in marijuana use days were moderate for both conditions at the 1-month follow-up. At the 6-month follow-up BMI+SFAS demonstrated moderate effect size reductions whereas as BMI+ED group was associated with small effect size reductions (see Table 2). Exploratory analyses examining sex and treatment revealed that within group effect size (SFAS) for marijuana reduction was similar for men (d=.62) and women (d=.67).
Table 2.
Pre-Post Means (SD) and Effect Sizes for Drinking and Drug Use Outcomes
| Outcome Variable | Baseline | 1-Month | 6-Month | Within Subjects Effect Size (dws) | |
|---|---|---|---|---|---|
| Group Status | M (SD) | M (SD) | M (SD) | 1-Month | 6-Month |
| Drinks Per Week | |||||
| SFAS | 15.34 (9.90) | 9.58 (9.35) | 9.97 (10.59) | .60 | .52 |
| Education | 11.53 (8.97 | 7.95 (8.59) | 9.36 (12.77) | .41 | .20 |
| Alcohol Related Problems | |||||
| SFAS | 11.72 (8.60) | 6.53 (7.48) | 8.33 (9.46) | .64 | .37 |
| Education | 10.89 (7.89) | 5.33 (6.85) | 5.94 (8.78) | .75 | .59 |
| Marijuana Use Days | |||||
| SFAS | 12.45 (10.74) | 8.74 (10.43) | 6.46 (9.12) | .35 | .41 |
| Education | 11.97 (10.77) | 8.88 (10.60) | 11.38 (12.28) | .29 | .05 |
Note. Although the primary analyses used an intent-to-treat approach that modeled missing data, for ease of interpretability, this table reports data only for those who completed each follow-up. All study participants reported heavy drinking at baseline and were included in the intent to treat drinking analyses. The descriptive data presented above includes 33 SFAS and 32 Education participants who provided data at all three time-points. The marijuana intent to treat analyses includes participants who reported marijuana use at baseline (SFAS, n = 31, Education n = 29). The descriptive marijuana use data presented above includes 23 SFAS and 21 Education participants who provided data at all three time-points.32 Completed 6-month follow-up assessment
Figure 2.
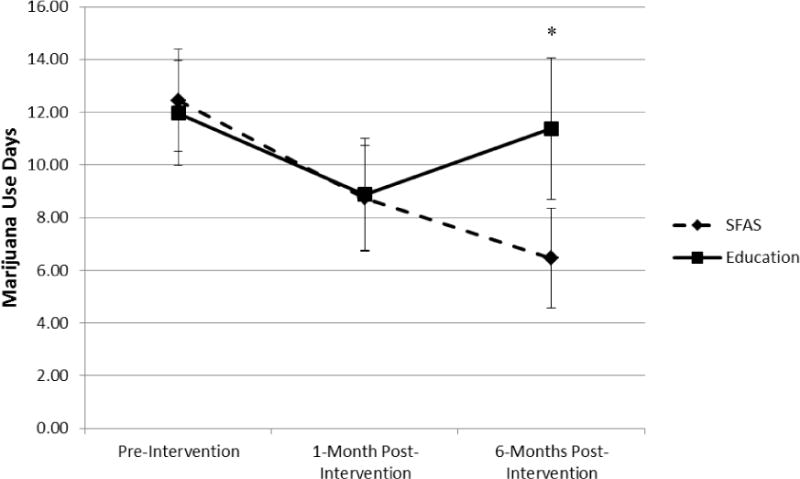
Changes in Number of Days Using Marijuana by Condition. Error bars reflect + Standard Error of the Mean.
Note. Results demonstrated a significant group by time interaction. *p < .05. Sample sizes for the SFAS condition were: baseline, n = 31, 1-month follow-up, n = 27, and 6-month follow-up, n = 23. Sample sizes for the ED condition were: baseline, n = 29, 1-month follow-up, n = 25, and 6-month follow-up, n = 21. The number of participants who reported any marijuana use at baseline, 1-month and 6-months were: SFAS (31, 18, and 15, respectively) and Education (29, 20, and 15, respectively).
Discussion
Consistent with previous research on BMIs, both intervention conditions were associated with significant, moderate effect size reductions in drinking (Cronce & Larimer, 2011; DeMartini et al., 2015). Contrary to our hypothesis, the BMI+SFAS was not associated with significantly greater reductions in drinking or alcohol related problems than the BMI+ED intervention. The BMI+SFAS session was associated with greater effect size reductions in monthly marijuana use in comparison to the BMI+ED condition that was equal in length and modality.
Although previous research suggests that stand-along alcohol education is not efficacious (Cronce & Larimer, 2011), to the authors’ knowledge, education has never previously been evaluated as a clinician-delivered intervention that occurs in conjunction with a BMI and it is possible that education delivered in this format is more efficacious than the relaxation control included in Murphy et al. In fact, similar to the future goal information included in the SFAS, information about the future health effects of drinking included in the education session may have elicited greater overall awareness of the future outcomes associated with heavy drinking.
Participants in the BMI+SFAS condition demonstrated moderate effect size reductions in drinks per week at both follow-ups that were comparable to the alcohol reductions in the Murphy et al. (2012) study, but the reductions in alcohol problems were smaller than observed in the earlier study. This may be due to the fact that the SFAS length was reduced to 30 minutes, hence decreasing the dosage of the original SFAS by approximately 50%, and that it was delivered immediately after the BMI rather than one week later as was the case in the original study. Although some prior research has indicated that providing longer BMI sessions (e.g., 10 vs. 50 min; Kulesza et al., 2010) or booster sessions (Barnett et al., 2007) does not appear to improve outcomes, a recent integrative data analysis study found that when brief alcohol intervention content is personalized, interventions that include more content are generally more efficacious (Ray et al., in 2014). It is also possible that the week delay between the BMI and the SFAS provides an ideal period for the student to consider drinking changes, and then enter the SFAS session open to the possibility of reorganizing their time in order to pursue other goals. When all the relatively novel alcohol, drug use, and SFAS-related content is delivered in a single appointment it may overwhelm the student and reduce the overall potency, particularly with respect to avoiding alcohol-related problems. Given the greater focus on drug use in this study compared to the Murphy et al. (2012) study, it is possible that for many participants the SFAS highlighted the particular incompatibility between illicit drug use and goal pursuit (Meshesha, Dennhardt, & Murphy, in 2015), and they focused their change efforts on reducing drug use rather than drinking.
Students in the SFAS condition made significant reductions in the number of days using marijuana at 6-months compared to those in the BMI+ED control group, whose use days returned to baseline levels. The effect sizes were slightly larger than those observed in other studies that examined marijuana outcomes in BMIs trials primarily focused on alcohol misuse (e.g., Amaro et al., 2010; White et al., 2006). The SFAS includes discussion/feedback related to a student’s academic and career goals, and the potential impact of a drug arrest on those goals (e.g., jeopardizing student loans, graduate school admission, professional licensure). This material may be particularly effective for motivating reductions in marijuana use. The emphasis on developing alternative leisure activities and on coping with stress and negative affect may have also contributed to the marijuana reductions, given that marijuana use is associated with stress and diminished engagement in academic activities (Dennhardt & Murphy, 2013; Meshesha et al., 2015). This seems to be especially true for marijuana users who also highly value alcohol. A paper that was recently published from this data (Dennhardt, Yurasek, Murphy, 2015) examined behavioral economic moderators and found that students with high alcohol demand who also used marijuana were more likely to reduce their use after the SFAS intervention.
The results of this study should be interpreted within the context of its limitations. The sample size was small and there was significant attrition at 6-months, which likely reduced our ability to identify significant differences between groups on drinking related variables. Additionally, we relied on self-report data rather than biological verification of drug and alcohol use. However, other trials in this area have used similar measurement approaches (Lee et al., 2010; 2013), and self-report may be the only feasible way to measure what may be relatively small reductions marijuana use in harm-reduction trials with non-treatment seeking marijuana users. Additionally, we did not include a comparable problem questionnaire for marijuana as we did for alcohol, nor did we have adequate measures of quantity of marijuana used or whether smoking occurred alongside alcohol consumption. Similarly, our study targeted both alcohol and drug use, however perhaps enrolling only marijuana users would be a better way to examine the efficacy of this intervention on marijuana use. Other limitations include baseline difference in drinking level and the relatively short-follow-up period. It is possible that the potential impact of developing alternatives to substance use may take more time to manifest as students become increasingly engaged and aware of the impact of substance use on other goals over time. It is also possible that many students may require repeated booster contact to effectively increase engagement in substance-free activities. Future research should consider asking participants to report on whether they implemented the various strategies and activities discussed during the SFAS session. The majority of our participants reported marijuana use, however future research may want to examine other substance use including tobacco.
Despite these limitations, this study extends the literature on brief alcohol interventions by evaluating a theoretically derived supplement using an experimental design. Despite the popularity of alcohol BMIs, there have been very few studies that have developed and evaluated brief supplements that attempt to improve their modest effect sizes and address co-occurring drug misuse (DeMartini et al., 2015). The results of the present study, in conjunction with the earlier SFAS evaluation (Murphy et al., 2012), suggests that the SFAS may result in incremental utility for reducing alcohol use and problems only if it is delivered as a 60-minute session a week after the alcohol BMI session, and that the SFAS may have utility, beyond a stand BMI, in reducing marijuana use.
Acknowledgments
This research was supported by the University of Memphis Psychology Department and a NIDA training grant to Ali Yurasek (T32 DA016184; PI: Damaris Rohsenow). Dr. Murphy’s contributions were supported by R01AA020829.
Footnotes
Disclosures
All authors contributed to the manuscript significantly and have read and approved the final manuscript. The authors have no conflicts of interest to disclose.
Although there is some evidence that reductions in alcohol use can contribute to decreases in marijuana use (Woolard et al., 2013), the results of an exploratory mediation analysis indicated that change in drinking was not a significant mediator on the effects of the BMI+SFAS on marijuana use days. Nor was change in marijuana use a significant mediator on the effects of the BMI+SFAS on alcohol related problems.
References
- Amaro H, Reed E, Rowe E, Picci J, Mantella P, Prado G. Brief screening and intervention for alcohol and drug use in a college student health clinic: Feasibility, implementation, and outcomes. Journal of American College Health. 2010;58(4):357–364. doi: 10.1080/07448480903501764. [DOI] [PubMed] [Google Scholar]
- Barnett NP, Murphy JG, Colby SM, Monti PM. Efficacy of counselor vs. computer-delivered intervention with mandated college students. Addictive Behaviors. 2007;32(11):2529–2548. doi: 10.1016/j.addbeh.2007.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnett NP, Tevyaw T, Fromme K, Borsari B, Carey KB, Corbin WR, Monti PM. Brief alcohol interventions with mandated or adjudicated college students. Alcoholism: Clinical and Experimental Research. 2004;28(6):966–975. doi: 10.1097/01.ALC.0000128231.97817.C7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel WK, Johnson MW, Koffarnus MN, MacKillop J, Murphy JG. The behavioral economics of Substance Use Disorders: Reinforcement pathologies and their repair. Annual Review of Clinical Psychology. 2014;13:20.1–20.37. doi: 10.1146/annurev-clinpsy-032813-153724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Broman CL. Percieved discrimination and alcohol use among black and white college students. Journal of Abnormal Psychology. 2007;51:448–456. [Google Scholar]
- Buscemi J, Murphy JG, Martens MP, McDevitt-Murphy ME, Dennhardt AA, Skidmore JR. Help-seeking for alcohol-related problems in college students: Correlates and preferred resources. Psychology of Addictive Behaviors. 2010;24(4):571–580. doi: 10.1037/a0021122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Carey MP, Maisto SA, Henson JM. Brief motivational interventions for heavy college drinkers: A randomized controlled trial. Journal of Consulting and Clinical Psychology. 2006;74(5):943–954. doi: 10.1037/0022-006X.74.5.943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Scott-Sheldon LJ, Carey MP, DeMartini KS. Individual Level interventions to reduce college student drinking: A meta-analytic review. Addictive Behaviors. 2007;32(11):2469–2494. doi: 10.1016/j.addbeh.2007.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins R, Parks GA, Marlatt G. Social determinants of alcohol consumption: The effects of social interaction and model status on the self-administration of alcohol. Journal of Consulting and Clinical Psychology. 1985;53(2):189–200. doi: 10.1037/0022-006X.53.2.189. [DOI] [PubMed] [Google Scholar]
- Cranford JA, McCabe S, Boyd CJ. A new measure of binge drinking: Prevalence and correlates in a probability sample of undergraduates. Alcoholism: Clinical and Experimental Research. 2006;30(11):1896–1905. doi: 10.1111/j.1530-0277.2006.00234.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cronce JM, Larimer ME. Individual-focused approaches to the prevention of college student drinking. Alcohol Research: Current Reviews. 2011;34(2):210–221. [PMC free article] [PubMed] [Google Scholar]
- Del Boca FK, Darkes J, Greenbaum PE, Goldman MS. Up close and personal: Temporal variability in the drinking of individual college students during their first year. Journal of Consulting and Clinical Psychology. 2004;72(2):155–164. doi: 10.1037/0022-006X.72.2.155. [DOI] [PubMed] [Google Scholar]
- DeMartini KS, Fucito LM, O’Malley SS. Novel approaches to individual alcohol interventions for heavy drinking college students and young adults. Current Addiction Reports. 2015 doi: 10.1007/s40429-015-0043-1/. Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dennhardt AA, Yurasek AM, Murphy JG. Change in delay discounting and substance reward value following a brief alcohol and drug use intervention. Journal Of The Experimental Analysis of Behavior. 2015;103(1):125–140. doi: 10.1002/jeab.121. [DOI] [PubMed] [Google Scholar]
- Grossbard JR, Mastroleo NR, Kilmer JR, Lee CM, Turrisi R, Larimer ME, Ray A. Substance use patterns among first-year college students: Secondary effects of a combined alcohol intervention. Journal of Substance Abuse Treatment. 2010;39(4):384–390. doi: 10.1016/j.jsat.2010.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gueorguieva R, Krystal JH. Move over ANOVA: Progress in analyzing repeated-measures data and its reflection in papers. Archives of General Psychiatry. 2004;61:310–317. doi: 10.1001/archpsyc.61.3.310. Retrieved from http://www.archgenpsychiatry.com/ [DOI] [PubMed] [Google Scholar]
- Heinz AJ, Lilje TC, Kassel JD, de Wit H. Quantifying reinforcement value and demand for psychoactive substances in humans. Current Drug Abuse Reviews. 2012;5(4):257–272. doi: 10.2174/1874473711205040002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hingson R, Berson J, Dowley K. Interventions to reduce college student drinking and related health and social problems. In: Plant M, Single E, Stockwell T, editors. Alcohol: Minimising the harm: What works? London England: Free Association Books; 1997. pp. 143–170. [Google Scholar]
- Hofmeyr A, Ainslie G, Charlton R, Ross D. The relationship between addiction and reward bundling: An experiment comparing smokers and non-smokers. Addiction. 2011;106(2):402–409. doi: 10.1111/j.1360-0443.2010.03166.x. [DOI] [PubMed] [Google Scholar]
- Kulesza M, Apperson M, Larimer ME, Copeland AL. Brief alcohol intervention for college drinkers: How brief is? Addictive Behaviors. 2010;35(7):730–733. doi: 10.1016/j.addbeh.2010.03.011. [DOI] [PubMed] [Google Scholar]
- Lee CM, Kilmer JR, Neighbors C, Atkins DC, Zheng C, Walker DD, Larimer ME. Indicated prevention for college student marijuana use: A randomized controlled trial. Journal of Consulting and Clinical Psychology. 2013;81(4):702–709. doi: 10.1037/a0033285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee C, Neighbors C, Kilmer J, Larimer M. A brief, web-based personalized feedback selective intervention for college student marijuana use: A randomized clinical trial. Psychology of Addictive Behaviors. 2010;24(2):265–273. doi: 10.1037/a0018859.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meshesha LZ, Dennhardt AD, Murphy JG. Polysubstance use is associated with deficits in substance-free reinforcement in college students. Journal of Studies on Alcohol and Drugs. 2015;76(1):106–116. [PubMed] [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Helping people change. 3rd. New York, NY US: Guilford Press; 2012. [Google Scholar]
- Murphy JG, Barnett NP, Colby SM. Alcohol-related and alcohol-free activity participation and enjoyment among college students: A behavioral theories of choice analysis. Experimental and Clinical Psychopharmacology. 2006;14(3):339–349. doi: 10.1037/1064-1297.14.3.339. [DOI] [PubMed] [Google Scholar]
- Murphy JG, Dennhardt AA, Skidmore JR, Martens MP, McDevitt-Murphy ME. Computerized versus motivational interviewing alcohol interventions: Impact on discrepancy, motivation, and drinking. Psychology Of Addictive Behaviors. 2010;24(4):628–639. doi: 10.1037/a0021347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy JG, Dennhardt AA, Skidmore JR, Borsari B, Barnett NP, Colby SM, Martens MP. A Randomized controlled trial of a behavioral economic supplement to brief motivational interventions for college drinking. Journal of Consulting and Clinical Psychology. 2012 doi: 10.1037/a0028763. Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy JG, Correia CJ, Colby SM, Vuchinich RE. Using behavioral theories of choice to predict drinking outcomes following a brief intervention. Experimental and Clinical Psychopharmacology. 2005;13(2):93–101. doi: 10.1037/1064-1297.13.2.93. [DOI] [PubMed] [Google Scholar]
- National Geographic Drugs Inc. (n.d.). Retrieved September 9th 2011 channel.nationalgeographic.com/channel/drugs-inc/interactives/infographic-how-marijuana-works/
- National Institute on Drug Abuse. (n.d.). Retrieved September 9th 2011 from http://www.drugabuse.gov.
- Nelson TF, Toomey TL, Lenk KM, Erickson DJ, Winters KC. Implementation of NIAAA College Drinking Task Force recommendations: How are colleges doing 6 years later? Alcoholism: Clinical and Experimental Research. 2010;34(10):1687–1693. doi: 10.1111/j.1530-0277.2010.01268.x. [DOI] [PubMed] [Google Scholar]
- Ray AE, Kim SY, White HR, Larimer ME, Mun EY, Clarke N, Jiao Y, Atkins DC, Huh D, The Project INTEGRATE Team When less is more and more is less in brief motivational interventions: Characteristics of intervention content and their associations with drinking outcomes. Psychology of Addictive Behaviors. 2014 doi: 10.1037/a0036593. http://dx.doi.org/10.1037/a0036593. [DOI] [PMC free article] [PubMed]
- Read JP, Merrill JE, Kahler CW, Strong DR. Predicting functional outcomes among college drinkers: Reliability and predictive validity of the Young Adult Alcohol Consequences Questionnaire. Addictive Behaviors. 2007;32(11):2597–2610. doi: 10.1016/j.addbeh.2007.06.021. [DOI] [PubMed] [Google Scholar]
- Tabachnick BG, Fidell LS. Using multivariate statistics. 4th. Boston: Allyn & Bacon; 2001. [Google Scholar]
- Turrisi R, Mallett KA, Cleveland MJ, Varvil-Weld L, Abar C, Scaglione N, Hultgren B. Evaluation of timing and dosage of a parent-based intervention to minimize college students’ alcohol consumption. Journal of Studies on Alcohol and Drugs. 2013;74(1):30–40. doi: 10.15288/jsad.2013.74.30. Retrieved from http://www.jsad.com/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- Virginia Department of Alcoholic Beverage Control. 2003 Retrieved September 9th 2011 from http://www.abc.state.va.us/Education/resources/AlcoholBody.pdf.
- Wells-Parker E. Mandated treatment: Lessons from research with drinking and driving offenders. Alcohol Health & Research World. 1995;18(4):302–306. [PMC free article] [PubMed] [Google Scholar]
- White HR, Morgan TJ, Pugh LA, Celinska K, Labouvie EW, Pandina RJ. Evaluating two brief substance-use interventions for mandated college students. Journal of Studies on Alcohol. 2006;67:309–317. doi: 10.15288/jsa.2006.67.309. Retrieved from http://www.jsad.com/ [DOI] [PubMed] [Google Scholar]
- Woolard R, Baird J, Longabaugh R, Nirenberg T, Lee CS, Mello MJ, Becker B. Project REDUCE: Reducing alcohol and marijuana misuse: Effects of a brief intervention in the Emergency Department. Addictive Behaviors. 2013;38(3):1732–1739. doi: 10.1016/j.addbeh.2012.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zakletskaia L, Wilson E, Fleming MF. Alcohol use in students seeking primary core treatment at university health services. Journal of American College Health. 2010;59(3):217–223. doi: 10.1080/07448481.2010.502413. [DOI] [PMC free article] [PubMed] [Google Scholar]