

Abstract
Dimercaptosuccinic acid (DMSA) is an analog of dimercaprol used as metal chelating moiety in variety of conditions. In nuclear medicine itself two types of Tc-99m DMSA complexes are used, trivalent and pentavalent forms. In this review, we have discussed the mechanism of uptake of both complexes as well as diagnostic and therapeutic application in a clinical scenario.
Keywords: Dimercaptosuccinic acid, glucose-mediated acidosis, pentavalent, renal cortex, trivalent
INTRODUCTION
Dimercaptosuccinic acid (DMSA) contains two sulfhydryl groups, an analog of dimercaprol and is used for metal chelation. Traditionally, this has been used as an antidote to heavy metal toxicity.[1,2] It is also reported to be used for removal of heavy metals from the body of autistic children, a one major concern in autism.[3] However, its chelation property has been exploited in nuclear medicine. Tc-99m labeled DMSA shows altered organ distribution depending on methods of preparation. At acidic pH (pH 2–3), DMSA chelates with technetium in lower oxidation (III) and forms a trivalent complex Tc-99m (III) DMSA also represented as Tc-99m DMSA [Figure 1a]. Tc-99m DMSA accumulates in proximal tubular cells of kidneys and thereby used for renal cortical imaging. At alkaline pH (pH 8–9), it chelates with technetium in higher oxidation state to form a pentavalent complex Tc-99m (V) DMSA, resembles phosphate ion and is rapidly excreted in the urine[4] [Figure 1b].
Figure 1.
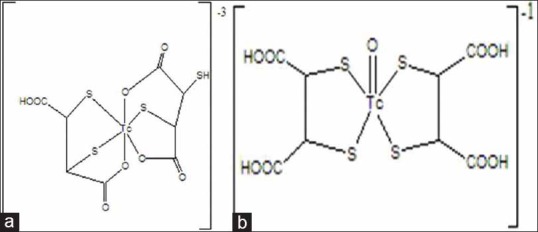
Chemical structure of (a) Tc-99m (III) dimercaptosuccinic acid (DMSA) and (b) Tc-99m (V) DMSA
MECHANISM OF UPTAKE
Trivalent Tc-99m dimercaptosuccinic acid
Trivalent Tc-99m DMSA has high binding affinity for the proximal convoluted tubules thus providing good imaging of the renal parenchyma. Two main Tc-99m DMSA tubular uptake routes have been proposed (i) peritubular extraction from plasma and (ii) tubular reabsorption.[5,6] Muller and Gutsche in 1995 proposed that after injection, Tc-99m DMSA is bound to plasma proteins in the circulating blood and penetrate the glomerular filter at very low rates. Tc-99m DMSA is completely excreted and does not reabsorbed from the tubular fluid. Peritubular excretion accounts for the Tc-99m DMSA uptake in the proximal tubular cells of the renal cortex. Tc-99m DMSA is then bound to the cell plasma protein with a high binding constant and accumulates in the kidney.[6] Burckhardt et al. proposed the role of sodium-dependent dicarboxylate transporter (NaDC-3) in the basolateral uptake of Tc-99m DMSA from peritubular capillaries into proximal tubule cells.[7] Tc-99m DMSA reabsorption from the glomerular ultra-filtrate substantially contributes to the renal uptake of the tracer.[8,9,10] Recently, Weyer et al. studied the role of the megalin/cubilin receptors for the accumulation of Tc-99m DMSA and proposed that Tc-99m DMSA binds to α-1 microglobulin plasma protein. Tc-99m DMSA is freely filtered by glomeruli and accumulates in renal proximal tubules by multiligand-binding mediated by megalin/cubilin receptor endocytosis. Free Tc-99m DMSA and trace amounts of microglobulin–bound Tc-99m DMSA are excreted in the urine.[11]
Pentavalent Tc-99m (V) dimercaptosuccinic acid
Tc-99m (V) DMSA localizes in a number of tumor types, most notably medullary thyroid carcinoma (MTC), bone metastases and other bone lesions. At pentavalent state, both sulfhydryl groups (-SH) of DMSA are bound with Tc-99m and no free -SH group is left for protein binding [Figure 1b]. The small Tc-99m (V) DMSA complex does not accumulate in the kidney and gets easily excreted by the kidney.[12]
Tc-99m (V) DMSA core has structural similarity with phosphate ion (PO4-3) and is avidly taken up by metabolic active cancer cells.[13,14] In addition, Tc-99m (V) DMSA uptake by tumors is related to glucose-mediated acidosis and mitotic activity.[15,16] In aggressive or malignant tumors the rate of glycolysis, so the production of lactic acid is increased that results in the acidic pH of the tumor microenvironment.[17,18] Phosphate is transported via all three NaPi co-transporters, however, Tc-99m (V) DMSA is transported by NaPi Type III co-transporters and can be used as a tumor proliferation marker.[19] Physiological uptake of Tc-99m (V) DMSA has been reported in the nasal mucosa, lacrimal glands and blood pool such as in the heart, and vessels. The excretion of Tc-99m(V)DMSA is through kidney. Uptake is also noted in pituitary and breast.[20,21]
FACTORS INFLUENCING THE UPTAKE OF TC-99M (V) DMSA
Phosphonoformic acid
The phosphate accumulation is linked to NaPi Type III co-transporter expression In the presence of a specific NaPi cotransporter inhibitor, phosphonoformic acid, Tc-99m (V) DMSA accumulation decreases with the decreased phosphate accumulation.[19]
Extracellular sodium concentration
Tc-99m (V) DMSA uptake is dependent on extracellular sodium concentration, in the same way as phosphate uptake, suggesting an important role of sodium-dependent transporter in Tc-99m (V) DMSA uptake and more specifically, the involvement of NaPi co-transporter, as phosphate transporters is known to be strongly dependent on extracellular sodium.[22] In the absence of extracellular sodium only <30% Tc-99m (V) DMSA enters in cells by simple diffusion.
pH
Uptake of both Tc-99m (V) DMSA and phosphate is stimulated at acidic pH and inhibited at alkaline pH. The plausible reason is that at acidic pH, carboxyl groups of DMSA (V) are fully associated and impart an average global charge of −1 to the DMSA (V) complex. The activity of Type III NaPi co-transporters increases because of preference for monovalent substrates.[18,23] Tumor cells over express Type III NaPi co-transporters and have more acidic extracellular pH than normal tissues.[15,17]
Applications of dimercaptosuccinic acid in nuclear medicine
Dimercaptosuccinic acid is a very useful radiopharmaceutical and being used for the detection of many diseases such as renal disorder, MTC, brain tumor, etc. Pentavalent Re-188/Re-186 DMSA is suitable candidate for internal radiation therapy.
TRIVALENT DIMERCAPTOSUCCINIC ACID (TC-99M DMSA)
Renal disorders
At low pH (2–3), trivalent Tc-99m DMSA is formed and localizes in the kidney. Since it is taken up by renal cortex and retained there, according to latest EANM guidelines, trivalent Tc-99m DMSA is the agent of choice for the detection of focal renal parenchymal abnormalities, renal sequelae after acute infection, acute pyelonephritis, ectopic kidney, confirmation of nonfunctional multicystic kidney and associated abnormalities such as abnormal duplex kidney, small kidney, dysplastic tissue, horseshoe kidney etc.[24] It is very useful in the detection of renal cortical scars. The superior renal to background ratio offered by DMSA is useful in the diagnosis of congenital renal conditions such as horseshoe kidney, ectopic kidney, crossed fused ectopic kidney. Tc-99m DMSA is also used to evaluate kidney parenchyma, functioning renal tissue and proximal tubular dysfunction. This scintigraphy has a great value in the diagnosis and evaluation of tubule-interstitial nephropathy in diseases like Joubert syndrome.[25]
Tc-99m DMSA renal scintigraphy can also be used to assess effects of cytotoxic drugs such as ifosfamide, cisplatin, methotrexate and cyclophosphamide on renal function in children who receive chemotherapy for various malignancies. A highly significant relationship has been reported between Tc-99m DMSA uptake and cumulative ifosfamide dose (P < 0.001).[26] Tc-99m DMSA scintigraphy is a noninvasive and sensitive method for the detection of ifosfamide-induced tubular dysfunction, subclinical injury and to predict risk at retreatment.[26,27,28]
PENTAVALENT DIMERCAPTOSUCCINIC ACID (TC-99M (V) DMSA)
The blood pool activity of Tc-99m (V) DMSA is seen up to 3 h and is actively taken up by the growing bones. Tc-99m (V) DMSA is proved to be useful in patients with MTC, brain, and soft tissue tumors. However in lung, liver, gastrointestinal tract, malignant melanoma and lymphoma Tc-99m (V) DMSA has only limited role.[29] The biodistribution and diagnostic value of Tc-99m (V) DMSA planar and single photon emission computed tomography (SPECT) scintigraphy had been assessed in patients with head and neck tumors. The results showed the bi-exponential blood clearance and rapid elimination from all organs except kidneys.[30]
Medullary carcinoma of thyroid
Medullary carcinoma of the thyroid is an uncommon tumor and arises from the parafollicular cells of the thyroid. The early detection of tumor sites in patients with MTC is important as it tends to metastasize to regional neck lymph nodes and mediastinum.[31] The major distant metastasis sites are lung, liver, and bones. Tc-99m (V) DMSA has demonstrated to be taken up by the primary as well as recurrent and metastatic tumors[32,33,34,35] [Table 1]. Intense accumulation of Tc-99m (V) DMSA is found in MTC and its metastatic sites.[36] Tc-99m (V) DMSA is found to be very specific since no significant uptake is observed in other thyroid malignancies, normal thyroid, salivary glands, and bones.[37]
Table 1.
Studies showing role of Tc-99m (V) DMSA in MTC
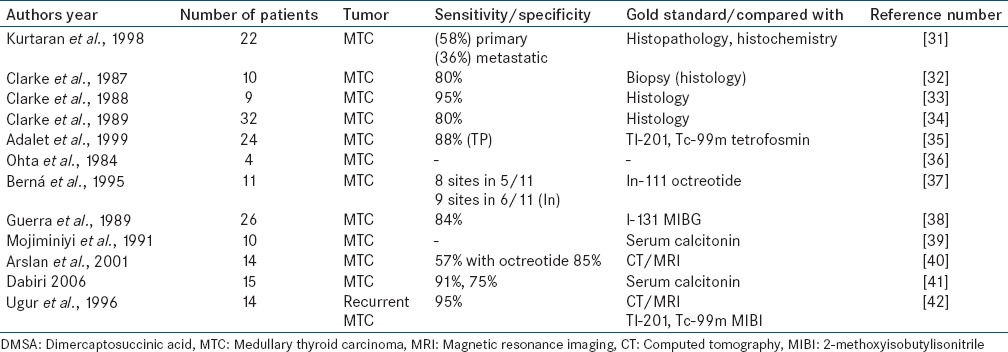
Tc-99m (V) DMSA has been compared to Tc-99m tetrofosmin and Tl-201 in patients of MTC with variable calcitonin levels and showed superior detection of metastatic sites in patients with MTC over Tc-99m tetrofosmin and Tl-201 scintigraphy.[35] Tc-99m (V) DMSA showed sensitivity similar to In-111 octreotide and I-131 MIBG in localizing primary MTC; but, these scans are unable to detect small lymph node involvement before initial surgery.[37,38] However, the sensitivity may improve with high serum calcitonin levels[39,40] Tc-99m (V) DMSA demonstrated better sensitivity and specificity as compared to CT and can be used for identification of recurrence or metastasis of MTC.[40,41] In another study based on the lesion sensitivity, Tc-99m (V) DMSA has been found to be superior to Tc-99m MIBI and Tl-201in the follow-up of MTC patients.[42] Tc-99m (V) DMSA may result in early diagnosis and proper management of patients with MTC [Table 1].
Head and neck
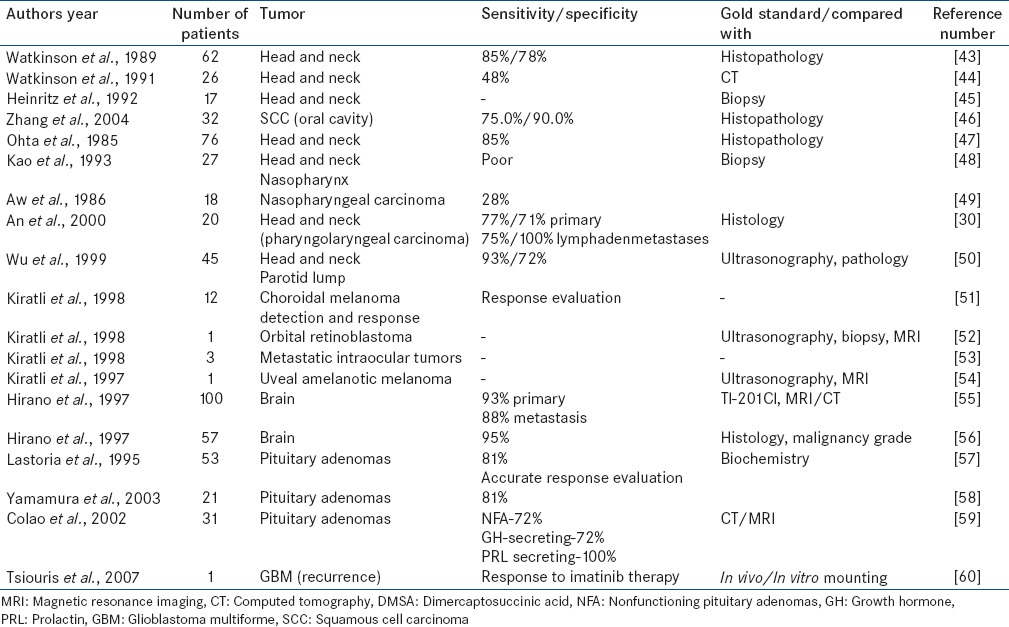
The identification of primary and metastatic sites plays an important role in the treatment and management of squamous cell carcinoma (SCC). Many radiopharmaceuticals such as Ga-67 citrate, Co-57 bleomycin, In-111 bleomycin, etc. have been used in past with low sensitivity and specificity. The studies of head and neck SCC of Tc-99m DMSA showed good uptake at the primary tumor and correlated well with the results of clinical and conventional imaging findings. However, it is found to be less sensitive for metastatic cervical nodes.[43,44,45] Tc-99m (V) DMSA SPECT imaging demonstrated high affinity in patients with oral SCC for metastatic lymph nodes in the neck and were helpful for designing proper neck dissection.[46,47] Tc-99m (V) DMSA showed no role in detecting primary nasopharyngeal carcinoma (NPC).[48,49] However, metastatic neck lymph node lesions of NPC could be detected by Tc-99m (V) DMSA. These studies demonstrated that Tc-99m (V) DMSA imaging may be used for the detection of the primary site in SCC of head and neck, with limited utility in the evaluation of cervical nodes.[45] The role of Tc-99m (V) DMSA has been explored in other head and neck malignancies like pharyngolaryngeal carcinoma and parotid tumors and fairly good results were obtained[30,50] [Table 2].
Table 2.
Studies showing role of Tc-99m (V) DMSA in head and neck, ocular and brain tumors
Ocular tumors
Tc-99m (V) DMSA scintigraphy may play a crucial role in the detection and follow-up of retinoblastoma, uveal amelanotic melanoma, and choroidal melanoma. Locally extended as well as a metastatic orbital retinoblastoma has been assessed by Tc-99m (V) DMSA. Planar and SPECT images demonstrated primary and metastatic sites which were confirmed by ultrasonography, magnetic resonance imaging, and incision biopsy.[51] Intraocular tumor of metastatic breast, lung, and rectal carcinomas can be imaged by Tc-99m (V) DMSA. The scan also detected unknown primary and other systemic lesions that may help in the diagnosis and the management of these patients[52,53,54] [Table 2]. This group suggested the complementary role of Tc-99m (V) DMSA on rare situations of decision making.
Brain tumors
Tc-99m (V) DMSA can be used as a promising agent for brain tumors. It has high specificity for differential diagnosis of benign from malignant tumors and also differentiating their histological malignancy grade, noninvasively. Approximately 95% of benign and malignant primary brain tumors are detected by Tc-99m (V) DMSA SPECT images. The vascularity could be adjudged by early uptake ratios without statistically significant difference in the tumor histology. The delayed uptake ratio, retention ratio, and retention index are higher for the malignant tumors as compared to the benign pathology. Tc-99m (V) DMSA also demonstrated superiority over Tl-201 imaging for primary and metastatic brain tumors[55,56,57,58,59,60] [Table 2].
Lung carcinoma
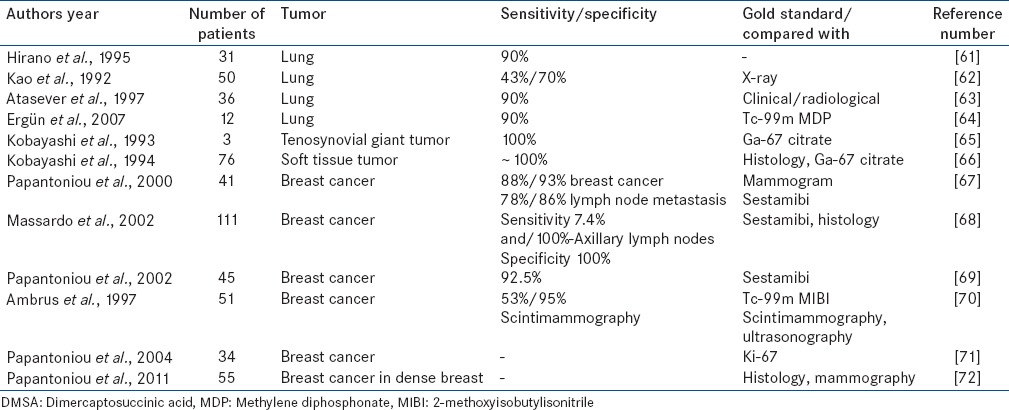
Role of Tc-99m (V) DMSA has also been assessed in primary lung cancers and related bone metastases. Various types of primary lung cancers (adenocarcinoma, SCC, small-cell carcinoma, large-cell carcinoma and bronchial carcinoid tumor) could also be detected (~90%) by Tc-99m (V) DMSA SPECT. No false-positive case for the primary lesions was reported. Uptake ratios were higher in SCCs than adenocarcinomas.[61,62,63,64] However, evaluation of mediastinal tumor extension and nodal metastatic lesions are difficult due to the high blood-pool activity and slow cardiovascular clearance. Differentiation of lung cancer from single solid lung mass showed little importance of Tc-99m (V) DMSA [Table 3].
Table 3.
Studies showing role of Tc-99m (V) DMSA in lung, soft tissue and breast cancers
Soft tissue tumor
Tc-99m (V) DMSA demonstrated diagnostic potential in histological proven cases of soft tissue tumors. Tc-99m (V) DMSA uptake is observed in almost all sarcomas, metastatic carcinomas, highly recurrent benign tumors of extra-abdominal desmoids, tenosynovial giant cell tumors, hemangiomas, and granulomatous soft-tissue lesions. Low-grade malignant and highly recurrent benign lesions can be detected with Tc-99m (V) DMSA scintigraphy with no uptake in benign solid soft tissue tumors[65,66] [Table 3].
Breast cancer
The role of Tc-99m (V) DMSA has been explored in scintimammography and demonstrated high sensitivity and specificity for breast cancers patients with high T/B ratios. Tc-99m (V) DMSA could detect cases of nonpalpable ductal carcinoma in situ, metastatic lymph nodes and preinvasive lesions with risk of developing malignancy. It is suitable for the assessment of primary lesions and axillary involvement in breast cancer patients and also for the surgical planning of such patients.[67,68,69,70] The uptake of Tc-99m (V) DMSA is found to have a positive correlation with the proliferative activity (Ki-67) of breast cancer cells. Tc-99m (V) DMSA uptake in breast cancer and Ki-67 expression suggests Tc-99m (V) DMSA as a surrogate marker of cell proliferation.[71] Tc-99m (V) DMSA correlates with tumor aggressiveness and provides important information regarding the correlation of tumor subtype with breast density[72] [Table 4].
Table 4.
Studies showing role of Tc-99m (V) DMSA in skeletal cancers (primary and metastatic) other cancers, infections and response to therapy
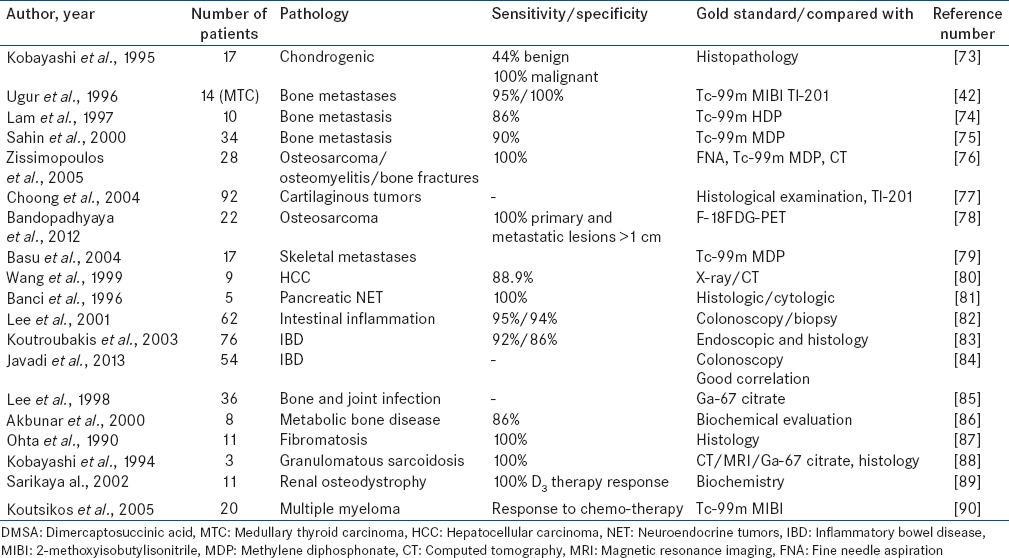
Skeletal metastases
Tc-99m (V) DMSA has also been evaluated in the detection of metastatic and degenerative bone lesions. The diagnostic efficacy of Tc-99m (V) DMSA in the detection of bone metastases is comparable to Tc-99m-methylene diphosphonate (MDP). However, degenerative lesions do not show the uptake of Tc-99m (V) DMSA.[42,73,74,75,76] Choong et al. evaluated Tc-99m (V) DMSA and Tl-201 imaging in the management of cartilaginous tumors and compared with histology.[77] Tc-99m (V) DMSA SPECT/CT in patients with osteosarcoma is found to be comparable with F-18 fluorodeoxyglucose (F-18 FDG) PET/CT in the evaluation of primary and metastatic lesions with size more than 1cm. However, F-18-FDG PET/CT could also detect sub-centimeter lesions.[78] Basu et al. studied and compared the findings of Tc-99m-MDP bone scan and Tc-99m (V) DMSA scintigraphy in the detection of osseous metastases arising from various malignancies[79] [Table 4].
Other tumors
The role of Tc-99m (V) DMSA has not been established in patients with carcinomas of the gastrointestinal tract, malignant melanoma, and lymphoma.[28] However, one study demonstrated approximately 90% sensitivity of Tc-99m (V) DMSA in the detection of hepatocellular carcinoma.[80] Pancreatic neuroendocrine tumors also demonstrated high uptake of Tc-99m (V) DMSA[81] [Table 4].
Infection and inflammation
Tc-99m (V) DMSA is also evaluated as an agent for visualization of inflammatory lesions and proven as a procedure of choice with colonoscopy for confirming the diagnosis.[82,83,84] Tc-99m (V) DMSA showed greater sensitivity and as well as accuracy than Ga-67 in the assessment of bone and joint infection, metabolic bone disease. However, the difference is not statistically significant.[85,86] High uptake at the sites of fibromatosis and moderate uptake at granulomatous inflammatory lesions of sarcoidosis is shown with Tc-99m (V) DMSA and could be of value in the diagnosis and in determining the appropriate site for biopsy[87,88] [Table 3].
Therapy and response evaluation
Re-186/188 (V) DMSA is a therapeutic analog of Tc-99m (V) DMSA and may be used for therapy of soft tissue tumors and bony metastases.[74] Basu et al. demonstrated the role a Tc-99m (V) DMSA in selection of patients for Re-188 (V) DMSA therapy and response evaluation to bisphosphonate therapy.[79] Re-186/188 (V) DMSA offers the potential for targeted radiotherapy, the avidity of the tracer in most bone metastasis suggests that this could be applied for palliative treatment. Tc-99m (V) DMSA is a noninvasive tumor cell proliferation marker and may also be used to evaluate the response to radio and chemotherapy, predict patient prognosis and help in management of various tumors and other therapies.[51,60,89,90]
CONCLUSION
Trivalent Tc-99m DMSA is a widely used tracer for renal cortical imaging. Tc-99m (V) DMSA accumulation is linked to phosphate uptake and kinase pathway activation and act as a surrogate marker of cell proliferation. It has the potential role in patient management, prognosis estimation, and therapy response monitoring. However, sensitivity is not comparable to F-18-FDG PET/CT in the detection of sub-centimeter nodules due to lower spatial resolution of the gamma camera than the PET/CT. The cost of F-18-FDG PET/CT scan is many times more than the cost of a Tc-99m (V) DMSA scan. However, it seems to be a good alternate to F-18-FDG PET/CT in those centers where PET/CT is not available. Furthermore, the sensitivity of Tc-99m (V) DMSA scan may be improved for detection of sub-centimeter nodules using the SPECT/CT. The β-emitting analogs Re-186/188 (V) DMSA offers the potential for targeted radiotherapy to Tc-99m (V) DMSA avid bone metastasis for palliative treatment.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Dart RC, Hurlbut KM, Maiorino RM, Mayersohn M, Aposhian HV, Hassen LV. Pharmacokinetics of meso-2,3-dimercaptosuccinic acid in patients with lead poisoning and in healthy adults. J Pediatr. 1994;125:309–16. doi: 10.1016/s0022-3476(94)70217-9. [DOI] [PubMed] [Google Scholar]
- 2.Asiedu P, Moulton T, Blum CB, Roldan E, Lolacono NJ, Graziano JH. Metabolism of meso-2,3-dimercaptosuccinic acid in lead-poisoned children and normal adults. Environ Health Perspect. 1995;103:734–9. doi: 10.1289/ehp.95103734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Adams JB, Baral M, Geis E, Mitchell J, Ingram J, Hensley A, et al. Safety and efficacy of oral DMSA therapy for children with autism spectrum disorders: Part A – Medical results. BMC Clin Pharmacol. 2009;9:16. doi: 10.1186/1472-6904-9-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Krejcarek GE, Wicks JH, Heerwald PE. The structure of stannous dimercaptosuccinic acid chelates. J Nucl Med. 1976;17:565. [Google Scholar]
- 5.de Lange MJ, Piers DA, Kosterink JG, van Luijk WH, Meijer S, de Zeeuw D, et al. Renal handling of technetium-99m DMSA: Evidence for glomerular filtration and peritubular uptake. J Nucl Med. 1989;30:1219–23. [PubMed] [Google Scholar]
- 6.Müller-Suur R, Gutsche HU. Tubular reabsorption of technetium-99m-DMSA. J Nucl Med. 1995;36:1654–8. [PubMed] [Google Scholar]
- 7.Burckhardt BC, Drinkuth B, Menzel C, König A, Steffgen J, Wright SH, et al. The renal Na(+)-dependent dicarboxylate transporter, NaDC-3, translocates dimethyl- and disulfhydryl-compounds and contributes to renal heavy metal detoxification. Am Soc Nephrol. 2002;13:2628–38. doi: 10.1097/01.asn.0000033463.58641.f9. [DOI] [PubMed] [Google Scholar]
- 8.Provoost AP, Van Aken M. Renal handling of technetium-99m DMSA in rats with proximal tubular dysfunction. J Nucl Med. 1985;26:1063–7. [PubMed] [Google Scholar]
- 9.Peters AM, Jones DH, Evans K, Gordon I. Two routes for 99mTc-DMSA uptake into the renal cortical tubular cell. Eur J Nucl Med. 1988;14:555–61. doi: 10.1007/BF00286776. [DOI] [PubMed] [Google Scholar]
- 10.van Luijk WH, Ensing GJ, Meijer S, Donker AJ, Piers DA. Is the relative 99mTc-DMSA clearance a useful marker of proximal tubular dysfunction? Eur J Nucl Med. 1984;9:439–42. doi: 10.1007/BF00563165. [DOI] [PubMed] [Google Scholar]
- 11.Weyer K, Nielsen R, Petersen SV, Christensen EI, Rehling M, Birn H. Renal uptake of 99mTc-dimercaptosuccinic acid is dependent on normal proximal tubule receptor-mediated endocytosis. J Nucl Med. 2013;54:159–65. doi: 10.2967/jnumed.112.110528. [DOI] [PubMed] [Google Scholar]
- 12.Blower PJ, Singh J, Clarke SE. The chemical identity of pentavalent technetium-99m-dimercaptosuccinic acid. J Nucl Med. 1991;32:845–9. [PubMed] [Google Scholar]
- 13.Yokoyama A, Saji H. Tumor diagnosis using radioactive metal ions and their complexes. In: Siegel H, Saji H, editors. Metal Ions in Biological Systems. New York: Marcel Dekker; 1980. pp. 313–40. [Google Scholar]
- 14.Wulfrank DA, Schelstraete KH, Small F, Fallais CJ. Analogy between tumor uptake of technetium(V)-99m dimercaptosuccinic acid (DMSA) and technetium-99m-MDP. Clin Nucl Med. 1989;14:588–93. doi: 10.1097/00003072-198908000-00007. [DOI] [PubMed] [Google Scholar]
- 15.Horiuchi K, Saji H, Yokoyama A. Tc(V)-DMS tumor localization mechanism: A pH-sensitive Tc(V)-DMS-enhanced target/nontarget ratio by glucose-mediated acidosis. Nucl Med Biol. 1998;25:549–55. doi: 10.1016/s0969-8051(98)00012-2. [DOI] [PubMed] [Google Scholar]
- 16.Papantoniou V, Nakopoulou L, Christodoulidou J, Papadaki E, Souvatzoglou M, Stipsaneli A, et al. Correlation and multivariate regression analysis between Tc-99m (V) DMSA and Tc-99m MIBI uptake and steroid receptors, proliferation index, tumor size, age, malignant grade, p53, and c-erbB-2 in primary breast cancer [abstract] Eur J Nucl Med. 2001;28:1120. [Google Scholar]
- 17.Tannock IF, Rotin D. Acid pH in tumors and its potential for therapeutic exploitation. Cancer Res. 1989;49:4373–84. [PubMed] [Google Scholar]
- 18.Werner A, Dehmelt L, Nalbant P. Na -dependent phosphate cotransporters: The NaPi protein families. J Exp Biol. 1998;201:3135–42. doi: 10.1242/jeb.201.23.3135. [DOI] [PubMed] [Google Scholar]
- 19.Denoyer D, Perek N, Le Jeune N, Frere D, Dubois F. Evidence that 99mTc-(V)-DMSA uptake is mediated by NaPi cotransporter type III in tumour cell lines. Eur J Nucl Med Mol Imaging. 2004;31:77–84. doi: 10.1007/s00259-003-1334-7. [DOI] [PubMed] [Google Scholar]
- 20.Watkinson JC, Lazarus CR, Mistry R, Maisey MN, Clarke SE. 99Tcm (v) DMSA: A clinical, planar and SPECT study to evaluate patients with head and neck squamous carcinoma. Nucl Med Commun. 1990;11:111–20. [PubMed] [Google Scholar]
- 21.Nakamoto Y, Sakahara H, Kobayashi H, Saga T, Tsuboyama N, Nakamura T, et al. Technetium-99m (V)-dimercaptosuccinic acid: Normal accumulation in the breasts. Eur J Nucl Med. 1997;24:1146–8. doi: 10.1007/BF01254247. [DOI] [PubMed] [Google Scholar]
- 22.Fernandes I, Béliveau R, Friedlander G, Silve C. Na, PO4 cotransport type III (PiT1) expression in human embryonic kidney cells and regulation by PTH. Am J Physiol Renal Physiol. 1999;277:F543–51. doi: 10.1152/ajprenal.1999.277.4.F543. [DOI] [PubMed] [Google Scholar]
- 23.Kavanaugh MP, Kabat D. Identification and characterization of a widely expressed phosphate transporter/retrovirus receptor family. Kidney Int. 1996;49:959–63. doi: 10.1038/ki.1996.135. [DOI] [PubMed] [Google Scholar]
- 24.Piepsz A, Colarinha P, Gordon I, Hahn K, Olivier P, Roca I, et al. Guidelines for 99mTc-DMSA scintigraphy in children. Eur J Nucl Med. 2001;28:BP37–41. [PubMed] [Google Scholar]
- 25.Gedik GK, Lay Ergün E, Fani Bozkurt M. The role of 99mTc DMSA renal scintigraphy in Joubert syndrome. Rev Esp Med Nucl. 2006;25:258–62. doi: 10.1157/13090659. [DOI] [PubMed] [Google Scholar]
- 26.Anninga JK, Valdés Olmos RA, de Kraker J, van Tinteren H, Hoefnagel CA, van Royen EA. Technetium-99m dimercaptosuccinic acid and ifosfamide tubular dysfunction in children with cancer. Eur J Nucl Med. 1994;21:658–62. doi: 10.1007/BF00285589. [DOI] [PubMed] [Google Scholar]
- 27.Rossleigh MA, Farnsworth RH, Leighton DM, Yong JL, Rose M, Christian CL. Technetium-99m dimercaptosuccinic acid scintigraphy studies of renal cortical scarring and renal length. J Nucl Med. 1998;39:1280–5. [PubMed] [Google Scholar]
- 28.Caglar M, Yarís N, Akyuz C. The utility of (99m)Tc-DMSA and Tc(99m)-EC scintigraphy for early diagnosis of ifosfamide induced nephrotoxicity. Nucl Med Commun. 2001;22:1325–32. doi: 10.1097/00006231-200112000-00008. [DOI] [PubMed] [Google Scholar]
- 29.Ohta H, Endo K, Fujita T, Konishi J, Torizuka K, Horiuchi K, et al. Clinical evaluation of tumour imaging using 99Tc(V)m dimercaptosuccinic acid, a new tumour-seeking agent. Nucl Med Commun. 1988;9:105–16. [PubMed] [Google Scholar]
- 30.An R, Bender H, Guhlke S, Biersack HJ. Diagnostic value of pentavalent 99mTc-dimercaptosuccinicacid ([V]-DMSA) in head and neck tumors. J Tongji Med Univ. 2000;20:303–7. doi: 10.1007/BF02888186. [DOI] [PubMed] [Google Scholar]
- 31.Kurtaran A, Scheuba C, Kaserer K, Schima W, Czerny C, Angelberger P, et al. Indium-111-DTPA-D-Phe-1-octreotide and technetium-99m-(V)-dimercaptosuccinic acid scanning in the preoperative staging of medullary thyroid carcinoma. J Nucl Med. 1998;39:1907–9. [PubMed] [Google Scholar]
- 32.Clarke SE, Lazarus C, Mistry R, Maisey MN. The role of technetium-99m pentavalent DMSA in the management of patients with medullary carcinoma of the thyroid. Br J Radiol. 1987;60:1089–92. doi: 10.1259/0007-1285-60-719-1089. [DOI] [PubMed] [Google Scholar]
- 33.Clarke SE, Lazarus CR, Wraight P, Sampson C, Maisey MN. Pentavalent [99mTc]DMSA, [131I]MIBG, and [99mTc]MDP – An evaluation of three imaging techniques in patients with medullary carcinoma of the thyroid. J Nucl Med. 1988;29:33–8. [PubMed] [Google Scholar]
- 34.Clarke S, Lazarus C, Maisey M. Experience in imaging medullary thyroid carcinoma using 99mTc (V) dimercaptosuccinic acid (DMSA) Henry Ford Hosp Med J. 1989;37:167–8. [PubMed] [Google Scholar]
- 35.Adalet I, Demirkale P, Unal S, Ouz H, Alagöl F, Cantez S. Disappointing results with Tc-99m tetrofosmin for detecting medullary thyroid carcinoma metastases comparison with Tc-99m VDMSA and TI-201. Clin Nucl Med. 1999;24:678–83. doi: 10.1097/00003072-199909000-00008. [DOI] [PubMed] [Google Scholar]
- 36.Ohta H, Yamamoto K, Endo K, Mori T, Hamanaka D, Shimazu A, et al. A new imaging agent for medullary carcinoma of the thyroid. J Nucl Med. 1984;25:323–5. [PubMed] [Google Scholar]
- 37.Berná L, Cabezas R, Mora J, Torres G, Estorch M, Carrió I. 111In-octreotide and 99mTc(V)-dimercaptosuccinic acid studies in the imaging of recurrent medullary thyroid carcinoma. J Endocrinol. 1995;144:339–45. doi: 10.1677/joe.0.1440339. [DOI] [PubMed] [Google Scholar]
- 38.Guerra UP, Pizzocaro C, Terzi A, Giubbini R, Maira G, Pagliaini R, et al. New tracers for the imaging of the medullary thyroid carcinoma. Nucl Med Commun. 1989;10:285–95. doi: 10.1097/00006231-198904000-00005. [DOI] [PubMed] [Google Scholar]
- 39.Mojiminiyi OA, Udelsman R, Soper ND, Shepstone BJ, Dudley NE. Pentavalent Tc-99m DMSA scintigraphy. Prospective evaluation of its role in the management of patients with medullary carcinoma of the thyroid. Clin Nucl Med. 1991;16:259–62. [PubMed] [Google Scholar]
- 40.Arslan N, Ilgan S, Yuksel D, Serdengecti M, Bulakbasi N, Ugur O, et al. Comparison of In-111 octreotide and Tc-99m (V) DMSA scintigraphy in the detection of medullary thyroid tumor foci in patients with elevated levels of tumor markers after surgery. Clin Nucl Med. 2001;26:683–8. doi: 10.1097/00003072-200108000-00004. [DOI] [PubMed] [Google Scholar]
- 41.Dabiri S. Tc-99m (V) DMSA in detection of metastases of medullary thyroid carcinoma. Iran J Nucl Med. 2006;14:15–24. [Google Scholar]
- 42.Ugur O, Kostakglu L, Güler N, Caner B, Uysal U, Elahi N, et al. Comparison of 99mTc(V)-DMSA, 201Tl and 99mTc-MIBI imaging in the follow-up of patients with medullary carcinoma of the thyroid. Eur J Nucl Med. 1996;23:1367–71. doi: 10.1007/BF01367593. [DOI] [PubMed] [Google Scholar]
- 43.Watkinson JC, Lazarus CR, Mistry R, Shaheen OH, Maisey MN, Clarke SE. Technetium-99m (v) dimercaptosuccinic acid uptake in patients with head and neck squamous carcinoma: Experience in imaging. J Nucl Med. 1989;30:174–80. [PubMed] [Google Scholar]
- 44.Watkinson JC, Lazarus CR, Todd C, Maisey MN, Clarke SE. Metastatic squamous carcinoma in the neck: An anatomical and physiological study using CT and SPECT 99Tcm (V) DMSA. Br J Radiol. 1991;64:909–14. doi: 10.1259/0007-1285-64-766-909. [DOI] [PubMed] [Google Scholar]
- 45.Heinritz H, Marienhagen J, Wolf F, Schuster B, Stenglein C, Iro H. Scintigraphic imaging of head and neck cancers with 99m technetium (v) dimercaptosuccinic acid. A prospective clinical study. HNO. 1992;40:437–41. [PubMed] [Google Scholar]
- 46.Zhang Y, Guo CB, Yu GY, Ma DQ, Li Q, Zhang CL. Application of 99mTc(V)-dimercaptosuccinic acid imaging in detecting neck metastases in patients with oral squamous cell carcinoma. Zhonghua Er Bi Yan Hou Ke Za Zhi. 2004;39:425–8. [PubMed] [Google Scholar]
- 47.Ohta H, Endo K, Fujita T, Nakashima T, Sakahara H, Torizuka K, et al. Imaging of head and neck tumors with technetium(V)-99m DMSA. A new tumor-seeking agent. Clin Nucl Med. 1985;10:855–60. doi: 10.1097/00003072-198512000-00006. [DOI] [PubMed] [Google Scholar]
- 48.Kao CH, Wang SJ, Wey SP, Shen LH, Ting G, Yeh SH. The detection of nasopharynx carcinoma in technetium-99m (V) dimercaptosuccinic acid SPECT imaging. Clin Nucl Med. 1993;18:321–3. doi: 10.1097/00003072-199304000-00011. [DOI] [PubMed] [Google Scholar]
- 49.Aw SE, Sundram FX, Goh AS. 99mTechnetium(V) dimercaptosuccinic acid (99mTc(v) DMSA) as a tumour seeking agent in nasopharyngeal carcinoma. Ann Acad Med Singapore. 1986;15:498–501. [PubMed] [Google Scholar]
- 50.Wu X, Lin G, Zhang Q. Evaluation of clinical value of technetium-99m(V) dimercaptosuccinic acid SPECT in diagnosis of parotid lump. Zhonghua Kou Qiang Yi Xue Za Zhi. 1999;34:334–6. [PubMed] [Google Scholar]
- 51.Kiratli H, Kiratli PO, Ercan MT. Scintigraphic evaluation of tumors metastatic to the choroid using technetium-99m(V)-dimercaptosuccinic acid. Jpn J Ophthalmol. 1998;42:60–5. doi: 10.1016/s0021-5155(97)00110-x. [DOI] [PubMed] [Google Scholar]
- 52.Kiratli PO, Kiratli H, Ercan MT. Visualization of orbital retinoblastoma with technetium-99m (V) dimercaptosuccinic acid. Ann Nucl Med. 1998;12:157–9. doi: 10.1007/BF03164782. [DOI] [PubMed] [Google Scholar]
- 53.Kiratli H, Kiratli PO, Ercan MT, Bilgiç S. Technetium-99m (V) dimercaptosuccinic acid uptake by choroidal melanoma before and after iodine-125 brachytherapy. Aust N Z J Ophthalmol. 1998;26:225–9. doi: 10.1111/j.1442-9071.1998.tb01316.x. [DOI] [PubMed] [Google Scholar]
- 54.Kiratli PO, Kiratli H, Ercan MT, Kostakoglu L. Visualization of uveal amelanotic melanoma with technetium-99m(V) dimercaptosuccinic acid. Ann Nucl Med. 1997;11:147–9. doi: 10.1007/BF03164824. [DOI] [PubMed] [Google Scholar]
- 55.Hirano T, Otake H, Shibasaki T, Tamura M, Endo K. Differentiating histologic malignancy of primary brain tumors: Pentavalent technetium-99m-DMSA. J Nucl Med. 1997;38:20–6. [PubMed] [Google Scholar]
- 56.Hirano T, Otake H, Kazama K, Wakabayashi K, Zama A, Shibasaki T, et al. Technetium-99m(V)-DMSA and thallium-201 in brain tumor imaging: Correlation with histology and malignant grade. J Nucl Med. 1997;38:1741–9. [PubMed] [Google Scholar]
- 57.Lastoria S, Colao A, Vergara E, Ferone D, Varrella P, Merola B, et al. Technetium-99m pentavalent dimercaptosuccinic acid imaging in patients with pituitary adenomas. Eur J Endocrinol. 1995;133:38–47. doi: 10.1530/eje.0.1330038. [DOI] [PubMed] [Google Scholar]
- 58.Yamamura K, Suzuki S, Yamamoto I. Differentiation of pituitary adenomas from other sellar and parasellar tumors by 99mTc(V)-DMSA scintigraphy. Neurol Med Chir (Tokyo) 2003;43:181–6. doi: 10.2176/nmc.43.181. [DOI] [PubMed] [Google Scholar]
- 59.Colao A, Ferone D, Lombardi G, Lastoria S. (99m)Technetium pentavalent dimercaptosuccinic acid scintigraphy in the follow-up of clinically nonfunctioning pituitary adenomas after radiotherapy. Clin Endocrinol (Oxf) 2002;56:713–21. doi: 10.1046/j.1365-2265.2002.01537.x. [DOI] [PubMed] [Google Scholar]
- 60.Tsiouris S, Pirmettis I, Chatzipanagiotou T, Ptohis N, Papantoniou V. Pentavalent technetium-99m dimercaptosuccinic acid [99m Tc-(V)DMSA] brain scintitomography – a plausible non-invasive depicter of glioblastoma proliferation and therapy response. J Neurooncol. 2007;85:291–5. doi: 10.1007/s11060-007-9410-7. [DOI] [PubMed] [Google Scholar]
- 61.Hirano T, Otake H, Yoshida I, Endo K. Primary lung cancer SPECT imaging with pentavalent technetium-99m-DMSA. J Nucl Med. 1995;36:202–7. [PubMed] [Google Scholar]
- 62.Kao CH, Wang SJ, Wey SP, Shen LH, Ting G, Yeh SH. Using technetium-99m (V) dimercaptosuccinic acid to detect malignancies from single solid masses in the lungs. Eur J Nucl Med. 1992;19:890–3. doi: 10.1007/BF00168166. [DOI] [PubMed] [Google Scholar]
- 63.Atasever T, Gündogdu C, Vural G, Kapucu LO, Karalezli A, Unlü M. Evaluation of pentavalent Tc-99m DMSA scintigraphy in small cell and nonsmall cell lung cancers. Nuklearmedizin. 1997;36:223–7. [PubMed] [Google Scholar]
- 64.Ergün EL, Kara PO, Gedik GK, Kars A, Türker A, Caner B. The role of Tc-99m (V) DMSA scintigraphy in the diagnosis and follow-up of lung cancer lesions. Ann Nucl Med. 2007;21:275–83. doi: 10.1007/s12149-007-0017-z. [DOI] [PubMed] [Google Scholar]
- 65.Kobayashi H, Sakahara H, Hosono M, Shirato M, Konishi J, Kotoura Y, et al. Scintigraphic evaluation of tenosynovial giant-cell tumor using technetium-99m(V)-dimercaptosuccinic acid. J Nucl Med. 1993;34:1745–7. [PubMed] [Google Scholar]
- 66.Kobayashi H, Sakahara H, Hosono M, Shirato M, Endo K, Kotoura Y, et al. Soft-tissue tumors: Diagnosis with Tc-99m (V) dimercaptosuccinic acid scintigraphy. Radiology. 1994;190:277–80. doi: 10.1148/radiology.190.1.8259419. [DOI] [PubMed] [Google Scholar]
- 67.Papantoniou V, Sotiropoulou M, Stipsaneli E, Louvrou A, Feda H, Christodoulidou J, et al. Scintimammographic findings of in situ ductal breast carcinoma in a double-phase study with Tc-99m(V) DMSA and Tc-99m MIBI value of Tc-99m(V) DMSA. Clin Nucl Med. 2000;25:434–9. doi: 10.1097/00003072-200006000-00009. [DOI] [PubMed] [Google Scholar]
- 68.Massardo T, Alonso O, Kabasakal L, Llamas-Olier A, Shankar UR, Zhu H, et al. Diagnostic value of 99mTc-methylene diphosphonate and 99mTc-pentavalent DMSA compared with 99mTc-sestamibi for palpable breast lesions. J Nucl Med. 2002;43:882–8. [PubMed] [Google Scholar]
- 69.Papantoniou V, Christodoulidou J, Papadaki E, Valotassiou V, Souvatzoglou M, Louvrou A, et al. Uptake and washout of 99mTcV-dimercaptosuccinic acid and 99mTc-sestamibi in the assessment of histological type and grade in breast cancer. Nucl Med Commun. 2002;23:461–7. doi: 10.1097/00006231-200205000-00006. [DOI] [PubMed] [Google Scholar]
- 70.Ambrus E, Rajtár M, Ormándi K, Séra T, Tószegi A, Láng J, et al. Value of 99m-Tc MIBI and 99m-Tc(V) DMSA scintigraphy in evaluation of breast mass lesions. Anticancer Res. 1997;17:1599–605. [PubMed] [Google Scholar]
- 71.Papantoniou VJ, Souvatzoglou MA, Valotassiou VJ, Louvrou AN, Ambela C, Koutsikos J, et al. Relationship of cell proliferation (Ki-67) to 99mTc-(V)DMSA uptake in breast cancer. Breast Cancer Res. 2004;6:R56–62. doi: 10.1186/bcr751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Papantoniou V, Valsamaki P, Sotiropoulou E, Tsaroucha A, Tsiouris S, Sotiropoulou M, et al. Increased breast density correlates with the proliferation-seeking radiotracer (99m)Tc(V)-DMSA uptake in florid epithelial hyperplasia and in mixed ductal carcinoma in situ with invasive ductal carcinoma but not in pure invasive ductal carcinoma or in mild epithelial hyperplasia. Mol Imaging. 2011;10:370–6. doi: 10.2310/7290.2010.00056. [DOI] [PubMed] [Google Scholar]
- 73.Kobayashi H, Kotoura Y, Hosono M, Tsuboyama T, Nishijima N, Sakahara H, et al. Uptake of pentavalent technetium-99m dimercaptosuccinic acid in idiopathic synovial chondromatosis. Ann Nucl Med. 1995;9:153–5. doi: 10.1007/BF03165044. [DOI] [PubMed] [Google Scholar]
- 74.Lam AS, Kettle AG, O’Doherty MJ, Coakley AJ, Barrington SF, Blower PJ. Pentavalent 99Tcm-DMSA imaging in patients with bone metastases. Nucl Med Commun. 1997;18:907–14. doi: 10.1097/00006231-199710000-00003. [DOI] [PubMed] [Google Scholar]
- 75.Sahin M, Basoglu T, Bernay I, Yapici O, Canbaz F, Yalin T. Evaluation of metastatic bone disease with pentavalent 99Tc(m)-dimercaptosuccinic acid: A comparison with whole-body scanning and 4/24 hour quantitation of vertebral lesions. Nucl Med Commun. 2000;21:251–8. doi: 10.1097/00006231-200003000-00009. [DOI] [PubMed] [Google Scholar]
- 76.Zissimopoulos A, Zanglis A, Andreopoulos D, Baziotis N. The role of 99mTc(V)-DMSA scan as compared to 99mTc-MDP and CT scans in imaging the primary tumor and metastases of osteosarcoma. Hell J Nucl Med. 2005;8:162–4. [PubMed] [Google Scholar]
- 77.Choong PF, Kunisada T, Slavin J, Schlicht S, Hicks R. The role of thallium-201 and pentavalent dimercaptosuccinic acid for staging cartilaginous tumours. Int Semin Surg Oncol. 2004;1:10. doi: 10.1186/1477-7800-1-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Bandopadhyaya GP, Gupta P, Singh A, Shukla J, Rastogi S, Kumar R, et al. (99m)Tc-DMSA (V) in Evaluation of Osteosarcoma: Comparative Studies with (18)F-FDG PET/CT in Detection of Primary and Malignant Lesions. ISRN Oncol. 2012;2012:371830. doi: 10.5402/2012/371830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Basu S, Nair N, Awasare S, Tiwari BP, Asopa R, Nair C. 99Tc(m)(V) DMSA scintigraphy in skeletal metastases and superscans arising from various malignancies: Diagnosis, treatment monitoring and therapeutic implic ations. Br J Radiol. 2004;77:347–61. doi: 10.1259/bjr/72600472. [DOI] [PubMed] [Google Scholar]
- 80.Wang SJ, Lin WY, Wey SP, Shen LH, Ting G. Pentavalent Tc-99m dimercaptosuccinic acid imaging of hepatocellular carcinoma. Neoplasma. 1999;46:246–8. [PubMed] [Google Scholar]
- 81.Banci M, Bianchi PL, Gianni W, Romani AM, De Vincentis G, Ierardi M, et al. Preliminary evaluation of the usefulness of Tc-99m (V) DMSA in pancreatic neuroendocrine tumors. Clin Nucl Med. 1996;21:122–4. doi: 10.1097/00003072-199602000-00009. [DOI] [PubMed] [Google Scholar]
- 82.Lee BF, Chiu NT, Wu DC, Tsai KB, Liu GC, Yu HS, et al. Use of 99mTc (V) DMSA scintigraphy in the detection and localization of intestinal inflammation: Comparison of findings and colonoscopy and biopsy. Radiology. 2001;220:381–5. doi: 10.1148/radiology.220.2.r01au30381. [DOI] [PubMed] [Google Scholar]
- 83.Koutroubakis IE, Koukouraki SI, Dimoulios PD, Velidaki AA, Karkavitsas NS, Kouroumalis EA. Active inflammatory bowel disease: Evaluation with 99mTc (V) DMSA scintigraphy. Radiology. 2003;229:70–4. doi: 10.1148/radiol.2291020692. [DOI] [PubMed] [Google Scholar]
- 84.Javadi H, Amiriani T, Mirkarimi H, Besharat S, Semnani S, Abedi J, et al. Scintigraphy with 99mTc(V)-DMSA in monitoring patients with inflammatory bowel disease. Hell J Nucl Med. 2013;16:209–12. [PubMed] [Google Scholar]
- 85.Lee BF, Chiu NT, Chang JK, Liu GC, Yu HS. Technetium-99m(V)-DMSA and gallium-67 in the assessment of bone and joint infection. J Nucl Med. 1998;39:2128–31. [PubMed] [Google Scholar]
- 86.Akbunar AT, Orhan B, Alper E. Bone-scan-like pattern with 99Tcm(V)-DMSA scintigraphy in patients with osteomalacia and primary hyperparathyroidism. Nucl Med Commun. 2000;21:181–5. doi: 10.1097/00006231-200002000-00010. [DOI] [PubMed] [Google Scholar]
- 87.Ohta H, Endo K, Konishi J, Iwasaki R, Kotoura Y, Yamamuro T, et al. Scintigraphic evaluation of aggressive fibromatosis. J Nucl Med. 1990;31:1632–4. [PubMed] [Google Scholar]
- 88.Kobayashi H, Kotoura Y, Sakahara H, Yamamuro T, Endo K, Konishi J. Solitary muscular sarcoidosis: CT, MRI, and scintigraphic characteristics. Skeletal Radiol. 1994;23:293–5. doi: 10.1007/BF02412364. [DOI] [PubMed] [Google Scholar]
- 89.Sarikaya A, Sen S, Hacimahmutoglu S, Pekindil G. 99mTc(V)-DMSA scintigraphy in monitoring the response of bone disease to vitamin D3 therapy in renal osteodystrophy. Ann Nucl Med. 2002;16:19–23. doi: 10.1007/BF02995287. [DOI] [PubMed] [Google Scholar]
- 90.Koutsikos J, Athanasoulis T, Anagnostopoulos A, Velidaki A, Passadi M, Dimopoulos MA, et al. Combined use of 99mTc-sestamibi and 99mTc-V-DMSA in the assessment of chemotherapy effectiveness in patients with multiple myeloma. J Nucl Med. 2005;46:978–82. [PubMed] [Google Scholar]