

Abstract
Objectives:
Assess the added value of dual time point F-18-fluorodeoxyglucose positron emission tomography/computed tomography (DTP F-18-FDG-PET/CT) in the differentiation of malignant from a benign lesion in cancer patients.
Materials and Methods:
Totally, 140 F-18-FDG PET/CT scans of 60 cancer patients who underwent DTP protocol (early whole body PET/CT [E] at 60 min [range, 45–76 min] and delayed limited PET/CT [D] on areas of interest at 120 min [range, 108–153 min] after the tracer injection) were retrospectively reviewed. Visual and semi-quantitative analysis was performed on both early and delayed images. All findings were confirmed by histopathology and/or at least 3 months follow-up (F-18-FDG PET/CT, CT, or magnetic resonance imaging). The result was considered true positive (TP) if delayed standardized uptake value (SUV) of suspicious lesions increased and confirmed to be malignant, false positive (FP) if delayed SUV increased and confirmed to be benign, true negative (TN) if delayed SUV unchanged or decreased and confirmed to be benign, and false negative (FN) if delayed SUV unchanged or decreased and confirmed to be malignant.
Results:
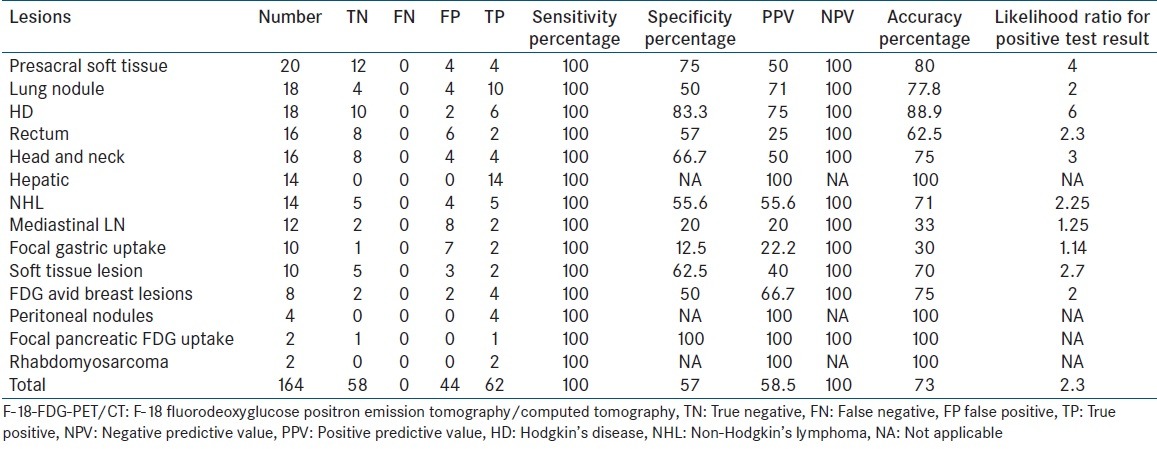
A total of 164 suspicious lesions were detected (20 presacral lesions, 18 lung nodules, 18 Hodgkin's disease (HD) lesions, 16 rectal lesions, 16 head and neck (H and N) lesions, 14 hepatic lesions, 14 non-Hodgkin's lymphoma (NHL) lesions, 12 mediastinal lymph nodes (LNs), 10 focal gastric uptake, 10 soft tissue lesions, 8 breast lesions, 4 peritoneal nodule, and 4 others). Sixty-four lesions were pathologically confirmed, and 100 lesions were confirmed based on 3–6 months follow-up. There were 62 TP lesions, 44 FP, 58 TN and no FN results. The overall sensitivity was 100% of DTP F-18-FDG PET/CT in detecting suspicious lesions. The specificity was 57% in differentiating malignant from benign lesions, and the accuracy was 73%. Positive predictive value was 59%, negative predictive value (NPV) 100%. All hepatic lesions were TP. Accuracy in metastatic hepatic lesions HD, presacral soft tissue, lung nodules, H, and N cancer, breast cancer, NHL and mediastinal LN was100%, 88.8%, 80%, 78%, 75%, 75%, 71%, and 33.3%, respectively.
Conclusions:
DTP F-18-FDG-PET/CT protocol does not always work in differentiation between benign and malignant lesions. However; it has high NPV, and promising results was noted in hepatic lesions, lymphoma, and recurrent rectal cancer.
Keywords: Delayed limited positron emission tomography/computed tomography, dual time point, F-18-fluorodeoxyglucose positron emission tomography/computed tomography
INTRODUCTION
F-18 fluorodeoxyglucose positron emission tomography/computed tomography (F-18-FDG PET/CT) has proved to be an accurate noninvasive imaging modality for differentiating malignant from benign lesions in cancer patients.[1,2] In general, a threshold for standardized uptake value (SUV) of > 2.5 has been proposed as the optimal threshold for differentiating between benign and malignant lesions.[3,4] However, the increased uptake of F-18-FDG has been found to be nonspecific for malignant lesions, and it can be seen in many benign lesions with high concentration of inflammatory cells, such as granulomas, fungal or bacterial infections, which potentially can result in false positive (FP) findings.[5,6,7]
Several reports have found that when SUV is measured sequentially, there is a correlation between the F-18-FDG uptake and time. In malignant lesions, there is continues increment of F-18-FDG uptake for several hours after F-18-FDG injection whereas such incremental uptake of F-18-FDG is rare in inflammatory/infectious or normal tissues. This may be due to the graded concentration of F-18-FDG in tumor cells, low glucose-6-phosphatase activity, and increase glucose uptake through glucose transporter in these cells.[8,9,10] Dual time point imaging (DTP) technique is a specialized protocol adopted in F-18-FDG PET/CT, claimed to be useful in facilitating the differentiation of malignant from benign lesions. Since the introduction of the DTP protocol, there were many studies assessed its value in different cancers and in different body regions. Some of these studies showed significant added value of DTP[8,9,10] while, others did not.[11,12,13,14]
Our study is a retrospective study aimed to assess the added value of DTP F-18-FDG-PET/CT in differentiation of malignant from benign lesions in cancer patients.
MATERIALS AND METHODS
Informed consent was not required for this retrospective study.
Patient population
Totally, 140 F-18-FDG PET/CT scans of 60 cancer patients who underwent DTP protocol and had suspicious F-18-FDG avid lesions (F-18-FDG uptake more than liver uptake in abdominal and pelvic lesions and more than mediastinal blood pool uptake in head and neck [H and N] and thoracic lesions) were retrospectively reviewed. There were 41 males and 19 females; mean age was 63 ± 10.4 years.
Dual-phase F-18-fluorodeoxyglucose positron emission tomography/computed tomography image acquisition and reconstruction
Early whole body F-18-FDG PET/CT (E) was acquired at 60 min (range, 45–76 min; mean, 61.7 ± 9.1 min), and delayed limited F-18-FDG PET/CT (D) on areas of interest was acquired at 120 min (range, 108–153 min; mean, 126.2 ± 12.6 min) after the tracer injection. All imaging and data acquisition were performed using a Gemini TF PET/CT scanner (Philips Medical Systems). The patients fasted for at least 4 h, and had blood glucose levels <165 mg immediately prior to administration of approximately 5.18 MBq/kg (0.14 mCi/kg) of F-18-FDG, with a maximum dose of 444 MBq (12 mCi) of F-18-FDG. During the subsequent 40–60 min between injection and scanning, patients were sitting calm in a quiet injection room without talking, covered with a blanket and without auditory stimuli, to avoid uptake of the radiotracer at physiological sites excited by these stimuli, which can result in artifacts that have false-positive interpretations. Patients were allowed to breathe normally during image acquisition without specific instructions. Emission data were acquired for 11–14 bed positions. Emission scans were acquired at 1 min/bed position always in a three-dimensional (3D) mode which may increase up to 2 or 3 min/bed position in case of obese patients dependent on the body mass index (BMI). The field of view (FOV) was from the base of the skull to mid-thigh with the arms above the head unless the patient cannot tolerate positioning the arm above the head, then, arms down position was used and if there was a significant truncation artifact from the arms in the pelvic region a localized PET/CT scan was done with the arms over the chest. The CT scans were used for attenuation correction purposes and to help in anatomic localization of F-18-FDG uptake. The 3D whole body acquisition parameters consisted of a 128 Χ 128 matrix and an 18 cm FOV with a 50% overlap.
The CT scan of the PET/CT scanner consisted of a 16 slices CT. Gantry allows for a patient port of 70 cm. CT parameters: It is a single sweep: 120–140 kV and 50–100 mA (based on BMI), 0.5 s per CT rotation, pitch - 1.675:1, slice thickness is 5 mm and 512 Χ 512 matrix. CT acquisition was performed before the emission acquisition. CT data were used for image fusion and the generation of the CT transmission map. No intravenous contrast was used. Breathing technique is breath hold after the normal expiration. If the patient cannot do it, then shallow breathing is acceptable.
Image analysis and semi-quantitative evaluation
Visual and semi-quantitative analysis was performed on both early and delayed images. F-18-FDG PET/CT scan or scans of each patient in our study population were reviewed by two nuclear medicine physician. Any suspicious F-18-FDG avid lesion in F-18-FDG PET/CT with F-18-FDG uptake more than liver uptake in abdominal and pelvic lesions and more than mediastinal blood pool uptake in head, neck, and thoracic lesions were evaluated and either correlated by biopsy or follow-up F-18-FDG PET/CT or other imaging modalities (CT and/or magnetic resonance imaging [MRI]) and recorded and tabulated. Interval changes in maximum SUV (SUVmax) between early PET/CT at 60 min postinjection (E) and delayed (D) limited PET/CT on areas of interest at 120 min postinjection were recorded. In the current study F-18-FDG avid lesions were analyzed as follows: True positive (TP) if SUVmax increased >0% in D images and confirmed to be malignant; FP if SUVmax increased >0% in D images and there was no evidence of malignancy on biopsy or follow-up; true negative (TN) if SUVmax unchanged or decreased in D images and there was no evidence of malignancy on biopsy or follow-up; false negative (FN) if SUVmax unchanged or decreased in D images and confirmed to be malignant.
Statistical analysis
All data were analyzed using MedCalc version 11 (MedCalc Software bvba, Mariakerke, Belgium). Data are presented as mean and standard deviation (SD) (mean ± SD). The sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), accuracy and the likelihood ratio for positive test result of the delayed F-18-FDG PET/CT imaging in differentiation between malignant and benign lesions were calculated. Nonpaired student t-test was used to compare mean percentage change in SUVmax (ΔSUVmax) between patients with confirmed malignant and those with benign lesions. Data were reanalyzed using 10% increment of SUVmax in D images as a threshold. P < 0.05 was considered as significant.
RESULTS
A total of 164 suspicious lesions were detected (20 presacral lesions, 18 lung nodules, 18 Hodgkin's disease (HD) lesions, 16 rectal lesions, 16 H and N lesions, 14 hepatic lesions, 14 non-Hodgkin's lymphoma (NHL) lesions, 12 mediastinal lymph nodes (LNs), 10 focal gastric uptake, 10 soft tissue lesions, 8 breast lesions, 4 peritoneal nodule, and 4 others). 64 lesions were pathologically confirmed, and 100 lesions were confirmed based on 3–6 months follow-up. All the 62 confirmed malignant lesions showed an increase in SUVmax >0% in delayed images resulted in 62 TP lesions [Figure 1]. There were 44 FP [Figure 2], 58 TN [Figure 3] and no FN results. The overall sensitivity was 100% of DTP F-18-FDG PET/CT in characterizing suspicious lesions. The specificity was 57% in differentiating malignant from benign lesions, the accuracy was 73%, PPV was 59%, and NPV was 100%. All hepatic lesions were TP. Accuracy in metastatic hepatic lesions, HD, presacral soft tissue, lung nodules, H and N cancer, breast cancer, NHL and mediastinal LN was 100%, 88.8%, 80%, 78%, 75%, 75%, 71%, and 33.3%, respectively. Diagnostic characteristics of DTP F-18-FDG-PET/CT in the differentiation of malignant from a benign lesion in cancer patients are summarized in Table 1.
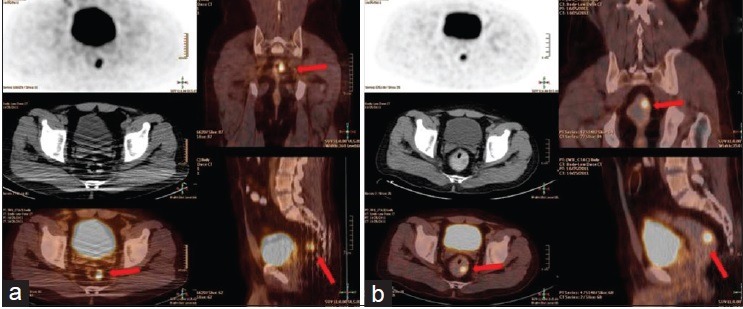
Figure 1.

True positive dual time point F-18-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT). A 46-year-old female who is a known case of breast Ca with pulmonary nodule. FDG PET/CT was done for characterization of the lung nodule. (a) Early FDG PET/CT fused images showed an FDG avid right lung apical density (white arrow) with maximum standardized uptake value (SUVmax) of 3.6 and a left supraclavicular brown fat FDG uptake (red arrow) with SUVmax of 8. (b) Two-hour delayed chest FDG PET/CT showed an increase of the SUVmax of the lung lesion to 5.6 and left supraclavicular brown fat to 9.8. CT guided biopsy, and pathological examination from the right apical lesion revealed metastases from breast cancer
Figure 2.
False positive dual time point F-18-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT). A 41-year-old male patient who is a known case of papillary thyroid carcinoma with negative I-131 whole body scan and elevated thyroglobulin (TG). FDG PET/CT was done to unmask the source of TG. Accidentally there was an FDG avid lesion protruded from the rectal wall (arrows) with maximum standardized uptake value was 6.2 in the early images (a) and increased to 9.7 in the 2-h delayed limited pelvic PET/CT with rectal enema (b). Polypectomy was done, and pathological examination revealed tubulovillous adenoma
Figure 3.
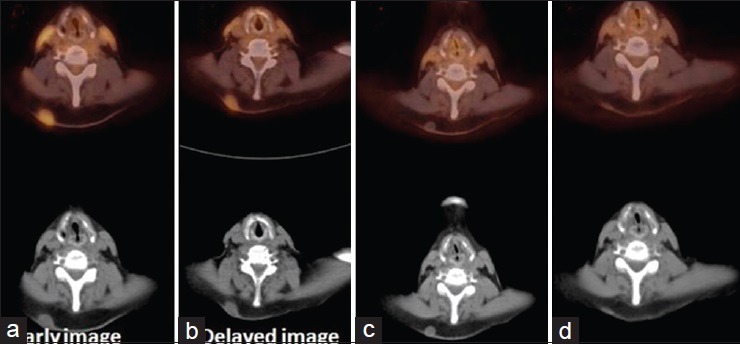
True negative dual time point F-18-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT). A 75-year-old male patient who is a known case of recurrent laryngeal carcinoma. Postchemotherapy FDG PET/CT; early (a) and 2-h delayed axial images (b) FDG avid subcutaneous nodule with early maximum standardized uptake value of 3.7 decreased to 2.5 in delayed image. Axial images of follow-up FDG PET/CT after 3 months (c) interval decrease in the size of the subcutaneous nodule with insignificant FDG uptake. Axial images of follow-up FDG PET/CT after 6 months (d) further interval decrease in the size of the subcutaneous nodule with insignificant FDG uptake without interval treatment suggesting benign nature of the subcutaneous nodule
Table 1.
Diagnostic characteristics of dual time point F-18-FDG-PET/CT in the differentiation of malignant from a benign lesion in 100 cancer patients
In the 58 TN lesions, SUVmax was either unchanged or decreased in delayed scans with percentage change of SUVmax ranged from 0% to 35.7% decrease in SUVmax, with average of 14.6% ± 12.8% decrease in SUVmax. In the 62 TP lesions, there was an increment of SUVmax in delayed scans ranged from 10% to 53.85%, with average increment of 31.5% ± 13.6%, and in the 44 FP lesions there was an increment of SUVmax in delayed scans ranged from 3.8% to 48.8%, with average increment of 32.5% ± 12.4%. There was no statistically significant difference between ΔSUVmax of TP lesions and FP lesions (P = 0.85).
There was no significant improvement of specificity or PPV after use of >10% increment of SUVmax in D images as a supplementary criterion. When an SUV increase of >10% was used as the threshold, the sensitivity, specificity, PPV, and NPV were 100%, 60%, 60%, and 100%, respectively. Therefore, the specificity and PPV of DTP F-18-FDG PET/CT in differentiating malignant from benign lesions remained quite low.
DISCUSSION
Fluorine-18-fluorodeoxyglucose PET/CT is widely used for differentiating malignant from benign lesions in cancer patients.[1,2,3,4] However, differentiation between malignant and benign inflammatory/infectious process is challenging as both can show increased F-18-FDG uptake.[15,16] Moreover, there is a considerable overlap between the SUVmax of malignant and benign lesions, causing FP results of F-18-FDG PET/CT.[17,18,19] Fortunately, malignant and inflammatory lesions exhibit a differential F-18-FDG uptake pattern over time. The gradual F-18-FDG uptake by a malignant tumor may be related to the relatively decreased expression of glucose-6-phosphatase rather than to increased hexokinase expression, resulting in a high hexokinase/phosphatase ratio. [20] In contrast, mononuclear cells, which represent the major cell population in chronic inflammation and infection, express high levels of glucose-6-phosphatase [21] and, therefore, have a relatively low ratio of hexokinase/phosphatase. Consequently, in mononuclear cells, F-18-FDG-6-phosphate can be rapidly dephosphorylated and cleared after reaching a certain level. [20] Based on the previous differences between malignant and inflammatory cells the DTP F-18-FDG PET/CT protocol and delayed F-18-FDG PET imaging have gained a considerable interest in the recent literature as an important diagnostic approach to improve the overall sensitivity, specificity, and accuracy of F-18-FDG PET/CT in differentiating malignant from benign lesions. [22] Although the usefulness of DTP F-18-FDG PET/CT protocol in differentiation of malignant from benign lesions has been reported in some studies of certain body regions and certain cancer types,[8,9,10] other studies reported a limited value in other body regions and other cancers.[11,12,13,14]
Our study assessed the sensitivity, specificity, PPV, NPV and accuracy of DTP F-18-FDG PET/CT protocol in some cancer types and some body regions. Table 1 summarize the results of our study and showed that the highest accuracy of DTP F-18-FDG PET/CT protocol of 100% is in focal hepatic lesions followed by 89%, 80%, 78%, 75%, 75% in F-18-FDG avid HD, presacral soft tissue lesions in rectal cancer, lung nodules, head or neck lesions in H and N cancer, and breast lesions in breast cancer. Accuracy of 100% was found in peritoneal nodules, pancreatic lesions, and rhabdomyosarcoma lesions, however; these lesions were represented by a few numbers which render accurate statistical analysis for these lesions difficult.
In our study all the 62 malignant lesions showed increased in SUVmax >0% in delayed images which corresponding with a study by Lan et al., [23] who assessed the value of DTP imaging in 96 patients with variable types of cancers, the authors reported that 54 of 59 (92%) patients with malignant lesions showed an increase in SUVmax in delayed images.
In our study, the overall sensitivity of DTP F-18-FDG PET/CT in detecting suspicious lesions was 100% which is similar to the sensitivity reported by Matthies et al., [24] for the evaluation of pulmonary nodules using DTP F-18-FDG PET protocol, and similar to that reported by Ma et al. [25] in the setting of cervical cancer, where DTP F-18-FDG PET protocol and delayed F-18-FDG PET improved the detection of para-aortic nodes (especially in the lower chains) whereas other modalities such as MRI showed FP results due to inflammation, edema, or scar tissue associated with radiation or postsurgical changes. Our results also comparable with Farghaly et al., [26] who studied the added value of DTP F-18-FDG PET/CT scanning in detection of local recurrence in rectal cancer and reported sensitivity, specificity, PPV, NPV and accuracy of delayed PET/CT to detect local recurrence based on ΔSUVmax >0% were 100%, 71.4%, 50%, 100%, and 77.8%, respectively.
The specificity of DTP F-18-FDG PET/CT scanning in differentiating malignant from benign lesions was 57%, the accuracy was 73%, PPV was 59%, and NPV was 100%. The low specificity and PPV of DTP likely result from the overlap between benign and malignant lesions in DTP F-18-FDG PET/CT imaging protocol which could be explained based on that F-18-FDG uptake in benign tumors was correlated with glucose transporter-1 expression, [27] and the retention index of F-18-FDG showed a positive correlation with the expression of hexokinase Type II. [28] These two factors have been suggested to be involved in the F-18-FDG accumulation mechanism in tumor tissues, may have influenced the high value of retention index in the benign lesions.
Our study showed that although the average increment in SUV max in delayed images of DTP F-18-FDG PET/CT in the TP malignant lesions was considerable (31.5 ± 13.6%), there was no statistically significant difference between ΔSUVmax in delayed images of DTP F-18-FDG PET/CT of TP and FP lesions. This indicates that the increment of SUVmax in delayed images of DTP F-18-FDG PET/CT protocol might have limited value in differentiation of benign from malignant lesions in cancer patients. This result corresponds with the findings from Sathekge et al., [11] who assessed the diagnostic accuracy of DTP F-18-FDG PET/CT for differentiating benign from malignant solitary pulmonary nodules in a tuberculosis-endemic area. They found that the mean percentage change in SUVmax from early to delayed F-18-FDG PET/CT images of benign lesions did not differ significantly from that of malignant lesions (17.1 ± 16.3% vs. 19.4 ± 23.7%), and thus suggested that DTP F-18-FDG PET/CT cannot distinguish malignancy from tuberculoma and, therefore, cannot reliably be used to reduce biopsy/thoracotomy. Shum et al. [13] investigated the value of the DTP F-18-FDG PET/CT in the assessment of the primary tumor, loco-regional LN and distant metastasis in patients with esophageal squamous cell carcinoma. The preliminary results of this study demonstrated that DTP F-18-FDG PET/CT had limited value in the detection of the primary tumor and loco-regional LN metastasis. For the distant metastasis, the sensitivity and specificity would be improved if retention index ≥10% is used as a supplemental criterion. Miyake et al. [14] adopted the DTP F-18-FDG PET/CT protocol for the evaluation of 44 patients with known or suspected colorectal cancer. The early scan at 1-h postinjection was, followed by early delayed scan (D-1) at 85 ± 7 min postinjection and delayed scan (D-2) at 124 ± 7 min postinjection. The clinical value of D-1 was evaluated by comparing diagnostic performance with D-2 for differentiating physiologic from pathological uptake and for staging colorectal cancer. They concluded that neither D-1 nor D-2 improved staging of colorectal cancer. However, D-1 scans yielded information useful for differentiating physiologic uptake from pathological uptake and may provide comparable efficacy with D-2 in the bowel.
On the other hand, other reports showed a clear distinction between benign and malignant lesions using DTP F-18-FDG PET/CT imaging protocol. Matthies et al. [24] adopted the DTP F-18-FDG PET protocol for the evaluation of pulmonary nodules in 36 patients with 38 known or suspected malignant pulmonary nodules. The early imaging time point was performed at an average of 70 min after F-18-FDG injection (range, 56–110 min) and the delayed imaging time point was performed at an average of 123 min after the tracer injection (range, 100–163 min). The percent increase in SUV in the malignant lesions over time was 20.5 ± 8.1%. In contrast, the majority of benign lesions either had a stable level of F-18-FDG uptake or declined over time. Kumar et al. [8] assessed the utility of DTP F-18-FDG PET imaging for identifying malignant lesions in the breast in 54 breast cancer patients with 57 breast lesions. They found increasing uptake of F-18-FDG over time in breast malignancies, whereas the uptake of F-18-FDG in inflammatory lesions and normal breast tissues decreases over time. They concluded that a percent change of + 3.75 or more in SUVmax over time is highly sensitive and specific in differentiating inflammatory lesions from malignant lesions.
In the current study, we found that all lesions that had unchanged or decreased SUVmax in delayed images are TN lesions, and no single FN lesion detected in current study. NPV of DTP F-18-FDG PET/CT scanning in cancer patients was 100%, which means that DTP F-18-FDG PET/CT scanning is highly reliable to rule out malignancy and when DTP F-18-FDG PET/CT scanning is negative it is unlikely that the lesion is malignant, and thus spare patients from unnecessary treatment. However, it has poor PPV so that when it is positive, it could be malignant or benign.
Our study included 164 suspicious lesions from different types of cancers and different body regions, and the accuracy of DTP F-18-FDG PET/CT were widely different between cancer types and body regions as shown in Table 1. The accuracy ranged from 100% in hepatic lesions to 30% in the focal gastric uptake. Hence, DTP protocol should not be used for all cancer patients, however; the decision should be based on the type and site of cancer.
CONCLUSIONS
Dual time point F-18-FDG-PET/CT protocol does not always work in differentiation between benign and malignant lesions. However; it has a high NPV denoting its high reliability to rule out malignancy. Promising results were noted in hepatic lesions, lymphoma, and recurrent rectal cancer.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Lee HJ, Lee J. Differential diagnosis of adrenal mass using imaging modality: Special emphasis on f-18 fluoro-2-deoxy-d-glucose positron emission tomography/computed tomography. Endocrinol Metab (Seoul) 2014;29:5–11. doi: 10.3803/EnM.2014.29.1.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kim SK, Allen-Auerbach M, Goldin J, Fueger BJ, Dahlbom M, Brown M, et al. Accuracy of PET/CT in characterization of solitary pulmonary lesions. J Nucl Med. 2007;48:214–20. [PubMed] [Google Scholar]
- 3.Charest M, Hickeson M, Lisbona R, Novales-Diaz JA, Derbekyan V, Turcotte RE. FDG PET/CT imaging in primary osseous and soft tissue sarcomas: A retrospective review of 212 cases. Eur J Nucl Med Mol Imaging. 2009;36:1944–51. doi: 10.1007/s00259-009-1203-0. [DOI] [PubMed] [Google Scholar]
- 4.Demura Y, Tsuchida T, Ishizaki T, Mizuno S, Totani Y, Ameshima S, et al. 18F-FDG accumulation with PET for differentiation between benign and malignant lesions in the thorax. J Nucl Med. 2003;44:540–8. [PubMed] [Google Scholar]
- 5.Kapucu LO, Meltzer CC, Townsend DW, Keenan RJ, Luketich JD. Fluorine-18-fluorodeoxyglucose uptake in pneumonia. J Nucl Med. 1998;39:1267–9. [PubMed] [Google Scholar]
- 6.Goo JM, Im JG, Do KH, Yeo JS, Seo JB, Kim HY, et al. Pulmonary tuberculoma evaluated by means of FDG PET: Findings in 10 cases. Radiology. 2000;216:117–21. doi: 10.1148/radiology.216.1.r00jl19117. [DOI] [PubMed] [Google Scholar]
- 7.Igai H, Gotoh M, Yokomise H. Computed tomography (CT) and positron emission tomography with [18F] fluoro-2-deoxy-D-glucose (FDG-PET) images of pulmonary cryptococcosis mimicking lung cancer. Eur J Cardiothorac Surg. 2006;30:837–9. doi: 10.1016/j.ejcts.2006.09.022. [DOI] [PubMed] [Google Scholar]
- 8.Kumar R, Loving VA, Chauhan A, Zhuang H, Mitchell S, Alavi A. Potential of dual-time-point imaging to improve breast cancer diagnosis with (18) F-FDG PET. J Nucl Med. 2005;46:1819–24. [PubMed] [Google Scholar]
- 9.Nakayama M, Okizaki A, Ishitoya S, Sakaguchi M, Sato J, Aburano T. Dual-time-point F-18 FDG PET/CT imaging for differentiating the lymph nodes between malignant lymphoma and benign lesions. Ann Nucl Med. 2013;27:163–9. doi: 10.1007/s12149-012-0669-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tian R, Su M, Tian Y, Li F, Li L, Kuang A, et al. Dual-time point PET/CT with F-18 FDG for the differentiation of malignant and benign bone lesions. Skeletal Radiol. 2009;38:451–8. doi: 10.1007/s00256-008-0643-0. [DOI] [PubMed] [Google Scholar]
- 11.Sathekge MM, Maes A, Pottel H, Stoltz A, van de Wiele C. Dual time-point FDG PET-CT for differentiating benign from malignant solitary pulmonary nodules in a TB endemic area. S Afr Med J. 2010;100:598–601. doi: 10.7196/samj.4082. [DOI] [PubMed] [Google Scholar]
- 12.Kaneko K, Sadashima E, Irie K, Hayashi A, Masunari S, Yoshida T, et al. Assessment of FDG retention differences between the FDG-avid benign pulmonary lesion and primary lung cancer using dual-time-point FDG-PET imaging. Ann Nucl Med. 2013;27:392–9. doi: 10.1007/s12149-013-0698-4. [DOI] [PubMed] [Google Scholar]
- 13.Shum WY, Hsieh TC, Yeh JJ, Chen JH, Su CC, Liang JA, et al. Clinical usefulness of dual-time FDG PET-CT in assessment of esophageal squamous cell carcinoma. Eur J Radiol. 2012;81:1024–8. doi: 10.1016/j.ejrad.2011.03.018. [DOI] [PubMed] [Google Scholar]
- 14.Miyake KK, Nakamoto Y, Togashi K. Dual-time-point 18F-FDG PET/CT in patients with colorectal cancer: Clinical value of early delayed scanning. Ann Nucl Med. 2012;26:492–500. doi: 10.1007/s12149-012-0599-y. [DOI] [PubMed] [Google Scholar]
- 15.Patz EF, Jr, Lowe VJ, Hoffman JM, Paine SS, Burrowes P, Coleman RE, et al. Focal pulmonary abnormalities: Evaluation with F-18 fluorodeoxyglucose PET scanning. Radiology. 1993;188:487–90. doi: 10.1148/radiology.188.2.8327702. [DOI] [PubMed] [Google Scholar]
- 16.Hübner KF, Buonocore E, Gould HR, Thie J, Smith GT, Stephens S, et al. Differentiating benign from malignant lung lesions using “quantitative” parameters of FDG PET images. Clin Nucl Med. 1996;21:941–9. doi: 10.1097/00003072-199612000-00005. [DOI] [PubMed] [Google Scholar]
- 17.Sonet A, Graux C, Nollevaux MC, Krug B, Bosly A, Vander Borght T. Unsuspected FDG-PET findings in the follow-up of patients with lymphoma. Ann Hematol. 2007;86:9–15. doi: 10.1007/s00277-006-0167-4. [DOI] [PubMed] [Google Scholar]
- 18.Zinzani PL, Tani M, Trisolini R, Fanti S, Stefoni V, Alifano M, et al. Histological verification of positive positron emission tomography findings in the follow-up of patients with mediastinal lymphoma. Haematologica. 2007;92:771–7. doi: 10.3324/haematol.10798. [DOI] [PubMed] [Google Scholar]
- 19.Maayan H, Ashkenazi Y, Nagler A, Izbicki G. Sarcoidosis and lymphoma: Case series and literature review. Sarcoidosis Vasc Diffuse Lung Dis. 2011;28:146–52. [PubMed] [Google Scholar]
- 20.Zhuang H, Pourdehnad M, Lambright ES, Yamamoto AJ, Lanuti M, Li P, et al. Dual time point 18F-FDG PET imaging for differentiating malignant from inflammatory processes. J Nucl Med. 2001;42:1412–7. [PubMed] [Google Scholar]
- 21.Suzuki S, Toyota T, Suzuki H, Goto Y. Partial purification from human mononuclear cells and placental plasma membranes of an insulin mediator which stimulates pyruvate dehydrogenase and suppresses glucose-6-phosphatase. Arch Biochem Biophys. 1984;235:418–26. doi: 10.1016/0003-9861(84)90215-7. [DOI] [PubMed] [Google Scholar]
- 22.Basu S, Alavi A. Partial volume correction of standardized uptake values and the dual time point in FDG-PET imaging: Should these be routinely employed in assessing patients with cancer? Eur J Nucl Med Mol Imaging. 2007;34:1527–9. doi: 10.1007/s00259-007-0467-5. [DOI] [PubMed] [Google Scholar]
- 23.Lan XL, Zhang YX, Wu ZJ, Jia Q, Wei H, Gao ZR. The value of dual time point (18) F-FDG PET imaging for the differentiation between malignant and benign lesions. Clin Radiol. 2008;63:756–64. doi: 10.1016/j.crad.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 24.Matthies A, Hickeson M, Cuchiara A, Alavi A. Dual time point 18F-FDG PET for the evaluation of pulmonary nodules. J Nucl Med. 2002;43:871–5. [PubMed] [Google Scholar]
- 25.Ma SY, See LC, Lai CH, Chou HH, Tsai CS, Ng KK, et al. Delayed (18) F-FDG PET for detection of paraaortic lymph node metastases in cervical cancer patients. J Nucl Med. 2003;44:1775–83. [PubMed] [Google Scholar]
- 26.Farghaly H, Nasr H, Nabulsi J. Diagnostic accuracy of 18F-FDG PET/CT in detection of local recurrence in rectal cancer and the added value of dual time point scanning. Egypt J Nucl Med. 2013;8:15–29. [Google Scholar]
- 27.Horiuchi C, Tsukuda M, Taguchi T, Ishiguro Y, Okudera K, Inoue T. Correlation between FDG-PET findings and GLUT1 expression in salivary gland pleomorphic adenomas. Ann Nucl Med. 2008;22:693–8. doi: 10.1007/s12149-008-0162-z. [DOI] [PubMed] [Google Scholar]
- 28.Higashi T, Saga T, Nakamoto Y, Ishimori T, Mamede MH, Wada M, et al. Relationship between retention index in dual-phase (18) F-FDG PET, and hexokinase-II and glucose transporter-1 expression in pancreatic cancer. J Nucl Med. 2002;43:173–80. [PubMed] [Google Scholar]