

Abstract
Introduction:
Nausea is the worst and most prevalent chemotherapy-induced complication experienced by 70–80% of patients despite mediation therapy. Reduction of nausea is one of the most important roles of oncologist nurses. Today, complementary therapies in addition to classic medicine, because of their lower costs, receive much attention. Nonetheless, their safety and effectiveness are not yet proven. The purpose of this research was to investigate the effect of therapeutic touch plan as a complementary therapy on acute nausea in women with breast cancer in 2012–2013 in Isfahan, Iran.
Materials and Methods:
A quasi-experimental, single-blind, randomized control trial with three groups (control, placebo and intervention) was performed at the Isfahan Seyedolshohada (AS) Teaching Hospital, Isfahan, in 2012–2013. The intervention was therapeutic touch plan on women with breast cancer, with the three groups receiving the same medicine regimen. Information was recorded by a checklist after infusion of chemotherapy drugs. Data analysis was performed by SPSS, ANOVA and Kruskal–Wallis tests.
Results:
The ANOVA test showed that the therapeutic touch plan was significantly effective in reducing the duration of nausea compared with the control and placebo groups (P < 0.001). The Kruskal–Wallis test showed that the frequency of occurrence of nausea was also reduced in the intervention and placebo groups compared with the control group (P < 0.001). The therapeutic touch plan was significantly effective in delaying the onset of nausea compared with the control and placebo groups (P < 0.001).
Conclusion:
This research showed that the therapeutic touch plan is effective in reducing acute chemotherapy-induced nausea; thus, education and implementation of the therapeutic touch plan is proposed for clinical nurses.
Keywords: Acute nausea, breast cancer, chemotherapy, therapeutic touch
INTRODUCTION
It is estimated that among all cancers in the country, the incidence of breast cancer ranks first among women.[1,2] According to the latest available statistics of the Isfahan province, Iran, breast cancer included 28% of cancer cases in women, and it has the second place for incidence of cancer in the province.[3]
Various treatments are used to control and treat cancer. Chemotherapy is one of the oldest and most common treatments for cancer, but being a systemic treatment, it causes numerous side-effects.[4,5] Nausea is the most common, the worst and the most troublesome complication, and is experienced by 70–80% of the patients. Therefore, the success of this treatment has been largely criticized.[5,6,7] The nurses are a key element of care, prevention and alleviation of chemotherapy-induced side-effects (in terms of primary and secondary prevention).[4]
Given the limited effectiveness and serious side-effects associated with conventional antiemetic drugs, one of the basic and low-risk measures is the use of complementary and alternative medicine.[8] Various researches have been conducted on the impact of different branches of alternative medicine on chemotherapy-induced nausea. Ebrahimi has confirmed, in his study, the effects of ginger on nausea induced by chemotherapy,[4] while Ghanbari et al., have not confirmed the effectiveness of ginger on nausea.[9] Molassiotis et al., in their study, have confirmed the effect of acupressure on these patients, while Joseph did not confirm the effect of electrical stimulation on nausea and vomiting in cancer patients.[10]
However, several studies in the field of complementary medicine for nausea caused by chemotherapy have had mixed results. Of the various complementary alternative medicinal methods, therapeutic touch has a unique position, as this method is essentially completed by one nurse.[11] Therapeutic touch was first founded by Dora Kunz and Dolores Krieger according to the “energy transfer” through “touching” in 1972. On the other hand, it is an independent action of a nurse that has been used for about 25 years, both in research and in clinical practice.[12,13,14,15,16,17,18,19,20] This technique is a form of art therapy where the therapist uses a form of focused consciousness and his/her hands as the center for creating balance and coordination in the field of bilateral energy of the patient and environment.[13]
The therapeutic touch technique has a wide range of uses, including reducing stress and anxiety, relieving pain (acute, chronic and neurological origin), reduction and control of cardiac arrhythmias, blood pressure, reduction of fatigue, increasing blood hemoglobin, carpal tunnel syndrome and abdominal cramping recovery, fever reduction, increasing speed of healing of wounds and fractures, premenstrual syndrome and insomnia. The above-mentioned symptoms have proven the positive effects of therapeutic touch. In addition to these signs, another sign that touch therapy has an effect on is nausea.[13,14,16,21,22,23] The literature review indicated that so far the effect of therapeutic touch on nausea induced by chemotherapy has not been assessed; therefore, this study aimed to evaluate the effect of therapeutic touch on nausea caused by chemotherapy based on specific predesigned programs. This study aimed to determine the effect of therapeutic touch on nausea in women with breast cancer undergoing chemotherapy.
MATERIALS AND METHODS
This was an experimental, single-blind, clinical trial (patients were not aware of their group regarding placebo or test). It consisted of three groups of control, placebo and experiment, and was carried out in 2012–2013. Initial sampling was purposive non-probability sampling, and then the subjects were randomly allocated into three groups. Then, by specifying the sampling frame of 108 patients, numbers 1–108 were written on cards and were placed in a ball. Then, the numbers were randomly drawn and allocated to the control, experiment and placebo groups, and, based on the subjects’ numbers, they were placed into the groups. The intervention included the use of therapeutic touch technique (meaning of therapeutic touch is touching the energy aura around the body) on women with breast cancer undergoing chemotherapy with the same medication regimen (cyclophosphamide, epirubicin, dexamethasone, plasil, kytril and emend) to relieve the symptoms of nausea and vomiting caused by chemotherapy.
Data collection tools for this study consisted of a form of demographic data, time record and frequency of nausea (the state of mind that is felt by the back of the throat and epigastric that may or may not lead to vomiting) checklist in four stages of morning, afternoon, evening and night in the acute phase (immediately after chemotherapy until the morning after).[24]
Demographic information included age, education, occupation, marital status, clients’ or head of household's income, number of children (if married), duration of illness, number of courses of chemotherapy, having a certain gastrointestinal disease and having or not having metastasis. All the cases (except the last case that was recorded in the patient's record) were completed by the patient. This checklist was prepared after library review and similar thesis review.[4,5] Later, the checklist was given to 10 professors and the required changes were applied, and then the face and content validity was obtained. The reliability of the checklist was measured by the researchers via test–retest, with an interval of 2 weeks, and the Pearson correlation coefficient was 85%.
The research environment was the Imam Reza Clinic, Isfahan Seyedolshohada (AS) Teaching Hospital, Isfahan, Iran. The subjects included 18–55-year-old patients with breast cancer with or without metastases (except metastasis of the central nervous system and gastrointestinal tract, which can lead to nausea and vomiting). Because of the large number of samples, the chemotherapy period was not limited; however, after sampling, Chi-square test was performed in the three groups to ensure uniform distribution of data.
The sample size was determined based on Altman's nomogram. This nomogram is a method for determining the sample size for the intervention study using test power and standard deviation of the considered variable in a similar study and calculating the parameter called clinical differences. This formula is calculated by dividing the difference that the researcher intends to provide in the standard deviation of the dependent variable over the standard deviation of the similar article by the standard deviation of the similar article. The similar study used was the article by Ebrahimi (2010), which assessed the effect of ginger (as an alternative medicinal treatment group) on the severity of nausea and vomiting caused by chemotherapy in cancer patients.[4] The frequency of standard deviation in this study was 5.1, and the researcher tried to reduce this amount to 1 in his study (difference of 4.1). By placing these numbers in the mentioned formula, the difference of 0.83 was obtained.

In Altman's nomogram, the left vertical axis corresponds to the clinical difference and the right vertical axis represents test power. By connecting these two numbers on the chart, the sample size in each group was determined. The test power was considered to be 0.7. The reason for considering 0.7 as the test power was that by considering a higher test power, such as 0.8, a much higher sample size in each group was achieved, which, because of the three groups, being interventional, and the need for follow-up for collecting the checklists, made the time of sampling impossible. The time limitation that the researchers were faced with during the interventions was increased due to the limited time for completing the students’ thesis. However, time spent with the same power (0.7) was almost 5 months. Therefore, the test power of 0.7 was confirmed by a statistic specialist followed by the Tarbiat Modares University Research Council. This matter was mentioned in the final section of the paper as one of the limitations of the research.
The researcher learned the different stages of therapeutic touch techniques under the supervision of a qualified professor (professor of nursing, who had also obtained the therapeutic touch technique certificate), theoretically (about philosophy and the nature of therapeutic touch techniques, and the different energy layers of the body) and practically, simultaneously. After approval by the professor regarding the ability to apply the right techniques on a patient, the researcher started the intervention on the patients in the hospital.
Groups were matched in terms of demographic variables (education level, patient and household income, the patient's occupation, marital status and age) through randomized allocation. The researcher started sampling in the sampling environment after introducing himself/herself and the content and purpose of the study, obtaining written informed consent from the patients and explaining about the checklist and how to complete it.
The subjects were selected from among those referring to the chemotherapy section for their treatment and according to the inclusion criteria and the order of their visits. After determining which group the patient was placed in (with respect to the sequence of visiting as previously described), in the control group, the patients received routine treatment (receiving chemotherapy-predetermined medications, identical to the experiment and placebo groups, including cyclophosphamide, epirubicin, dexamethasone, plasil, kytril and emend) and the questionnaire and checklist were completed. The demographic data form was completed by the researcher. In addition, the checklist was handed to the patient if literate and the explanations regarding how to complete it were given until the morning after chemotherapy. If they were not literate, it was given to their family member or friend accompanying the patient. In either case, the form and how to complete it were also taught to the accompanying person.
The therapeutic touch program was performed as follows:
In the experiment group, the patients were taken to a quiet room and those accompanying them could also join them. The patients were asked to sit on a chair, close their eyes and start breathing slowly and deeply and not to think about anything. After focusing, the researcher started to explore the first layer of energy on the solar chakra with his hands, 12–15 cm away from the body, from top to bottom with focus. Then, the researcher readjusted any disruption in energy and reassessed the modification and energy balance. This stage was performed once for each patient immediately before receiving chemotherapy for 15–20 min.[11,23] In the placebo group, for the same amount of time, the hands were placed around the body as a gesture, with more distance from the body, and were moved without a certain order. Then, the checklist was given to the patient to record the duration and frequency of nausea for up to 24 h after chemotherapy and to bring along in the next therapy session. The patients’ phone number was saved and, to ensure the completing and returning of the checklist, they would be contacted if they did not return the form after 1 month. Sampling lasted a total of 5 months.
Data were analyzed using SPSS for Windows (version 16, SPSS Inc., Chicago, IL, USA), ANOVA test and Kruskal–Wallis test. The present research was extracted from a Master's thesis in nursing supported by the Tarbiat Modares University of Tehran (Iran). It was recorded in a clinical trial website with the code IRCT 2013080311136N2.
RESULTS
In this study, 108 women with breast cancer, with or without metastases (excluding metastases of the central nervous system and gastrointestinal tract, which can lead to nausea and vomiting), were divided into groups of control, placebo and experiment (36 subjects each). There was no loss of samples with follow-up regarding the return of the questionnaires. Demographic data showed that the three groups were matched for demographic characteristics. Chi-square test showed no statistically significant differences (P > 0.05). Demographic characteristics of the patients are listed in Table 1.
Table 1.
Frequency distribution of demographic characteristics of patients in the three groups
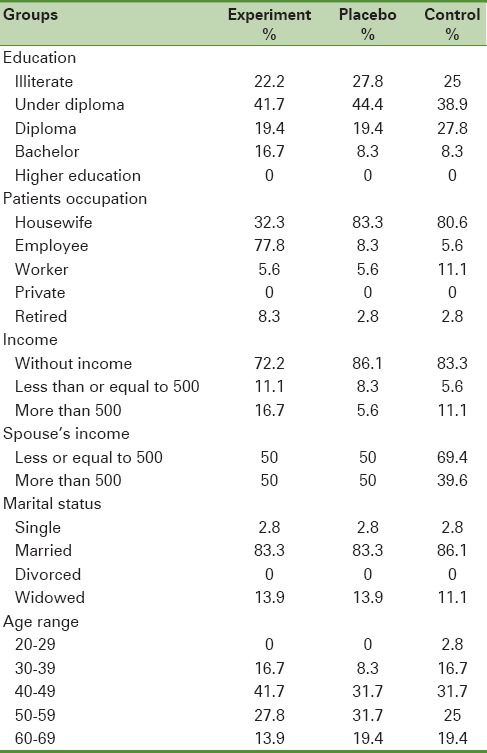
Mean age of the subjects was 49.7 ± 9.2. Most subjects in all three groups were married, housewives, had no independent income and education level under diploma. Most of them had no history of gastrointestinal disease and had no metastasis. In reviewing the time of nausea, it was shown that in the experimental group, 47.2% were nauseated at night and morning, 63.9% in the placebo group during the evening and night and 41.7% in the control group in the midday and evening.
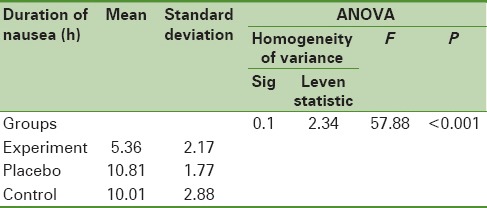
The ANOVA test, regarding the time of nausea, showed that the average time of nausea was not similar among the three groups (P < 0.001). Tukey's test in comparing each of the two groups showed that duration of nausea in the intervention group was significantly lower than the placebo and control groups. The mean duration of nausea in the three groups are presented in Table 2.
Table 2.
Comparison of the duration of nausea in the three groups-experimental, placebo and control-during the acute phase
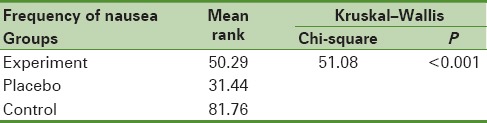
Regarding the frequency of nausea in the acute phase, the Kruskal–Wallis analysis showed that the frequency of nausea varies significantly between the three groups (P < 0.001). Pair-wise comparison of the groups (post hoc) showed that there were significant differences between the experiment and control groups. Furthermore, there were statistically significant differences among the placebo and control groups (P < 0.001) [Table 3].
Table 3.
Comparison of frequency of nausea in the three groups-experimental, placebo and control-during the acute phase
DISCUSSION
This study aimed to determine the effect of therapeutic touch on nausea induced by chemotherapy in breast cancer patients. The findings showed that therapeutic touch intervention significantly reduced the duration of nausea compared with the placebo and control groups. On the other hand, the pair-wise comparison of the groups showed that the duration of nausea in the placebo group was the same as the control group (P = 0.3). Pretending did not cause a reduction in the duration of nausea in patients in the placebo group compared with the intervention group.
In a study in 2000, progressive muscle relaxation interventions on patients with cancer receiving chemotherapy showed that intervention in the experiment group resulted in a significant reduction in the duration of nausea during chemotherapy (acute phase) (P < 0.05).[5] This was consistent with the findings of the present study.
Billhult et al.,[25] examined the effect of massage and Ghazlaje and Rahimiha,[26] in 2004, reported the impact of foot massage as a complementary therapy in the management of chemotherapy-induced nausea. The findings of these studies were consistent with the results of the present study. However, in a study conducted at the University of Minnesota, USA, on 230 cancer patients receiving chemotherapy, therapeutic touch had no significant effect on nausea in these patients.[27] From the researcher's perspective, differences in the type of chemotherapy regimen, therapeutic touch techniques, medication and cancer type can be considered as possible causes of this paradox.
Regarding the frequency of nausea, although the experimental group had a significantly decreased frequency of nausea, patients in the placebo group also experienced reduced frequency of nausea. In 2009, Ghanbari et al., also reported that the use of ginger was not effective in reducing nausea in the intervention group compared with the control group.[9] Roscoe et al., in 2010 reached the same conclusion regarding the effect of electrical stimulation.[28]
However, Molassiotis et al., in their study in 2013 showed the positive effects of acupressure on relieving nausea in cancer patients compared with the control group and the placebo group.[10] In this regard, Suzanne et al., in a study on 160 women with breast cancer undergoing chemotherapy demonstrated that acupressure leads to a significant reduction in delayed nausea in these patients.[29] This was consistent with the findings of the present study. In this regard, Shen and Glaspy evaluated the effect of acupressure on nausea and vomiting induced by chemotherapy in patients with gastric cancer and reached similar results.[30]
In explaining these findings of the research from the perspective of traditional Chinese medicine, nausea and vomiting are due to the disruption in energy balance in one of the body orbits called the pericardium. In addition, with touch therapy, the therapist is trying to restore the energy balance. Researchers believe that touch therapy can relieve physical tension and create relaxation, and has a significant impact on reducing nausea in the subjects. The findings of this study also confirm these beliefs.
Regarding the time of nausea among the three groups after the intervention, it was found that touch therapy delays the onset of nausea, while the majority of patients in the control group were nauseated from morning or afternoon. This, itself, is a milestone in controlling nausea because the absence of nausea immediately after completion of chemotherapy, as the patient expects it, could be promising for the patients.
The results showed that the use of the therapeutic touch program, complementary therapy conducted with the defined conditions, has a positive impact on reducing the duration of acute nausea and delaying its onset. Therefore, the results of this intervention can be widely used as a practical, complementary therapy in similar cases. However, it is important to note that when performing therapeutic touch, the patient is inactive and should sit quietly and not think about anything. This is very important regarding cancer patients who have some degree of weakness, fatigue and depression due to their illness.[31] It is important to note that anyone who has the ability and desire to help others (even family members of patients) can perform it after receiving training.[32]
CONCLUSION
The results of the use of the therapeutic touch program showed that this type of complementary therapy conducted with the defined conditions has a positive impact on reducing the duration of acute nausea and delaying its onset. Therefore, the results of this intervention can be used in similar cases (for breast cancer patients treated with cyclophosphamide regimen, epirubicin, dexamethasone, plasil, kytril and emend), and also as operational procedures after training oncology nurses about the use of therapeutic touch.
A limitation of the present study was that the late phase of intervention was not examined in this study because there was no possibility of performing the intervention again for the late phase. Patients came from different cities and far destinations, and readmission of many was not possible. Also, fatigue and weakness were also other reasons. To prevent sample loss as a result of occurrence of bias in this phase, intervention and review was avoided in this phase. If the clinical nurses obtained the skills for the techniques presented in this program, given the proof of their effectiveness, they can perform it in addition to the doctor's medical treatment. Moreover, they can accelerate patients’ recovery and eliminate bothersome symptoms, especially nausea and vomiting, using the program presented in this study and without any treatment-related side-effects. On the other hand, because this technique involves learning relaxation exercises and yoga, it also has positive effects on the nurses. Training clinical nurses and introducing the program developed in this paper are possible through in-service training programs and workshops using the experiences of trained teachers and in the universities as workshops using touch therapy experts. Furthermore, training nursing students can also be very helpful. Today, therapeutic touch is taught in more than 100 colleges of nursing in Europe and the United States. In addition, it is recognized by the American Nurses Association (ANA), National League for Nurses and American Holistic Nurses Association. The North American Nursing Diagnosis (NANDA) has recorded the disruptions in the energy field as a standard diagnosis of nursing, and it is estimated that over 40,000 nurses in the United States perform therapeutic touch.[33]
Because of the innocuous and noninvasive characteristics of touch therapy and its being simple to learn, it is recommended that this approach, as a complementary nursing intervention in the management of nausea resulting from chemotherapy, be taught to students and nurses. It is hoped that nurses use this simple, inexpensive and uncomplicated method as a complementary treatment to antiemetic drugs in clinical use.
Because the therapeutic touch program introduced in this paper was effective on nausea caused by chemotherapy in patients with breast cancer, learning and performing this program is recommended for chemotherapy units. It is also suggested that future research be performed on the effect of therapeutic touch on the delayed phase of nausea caused by chemotherapy and on other disturbing factors in cancer patients, such as insomnia, or compare therapeutic touch with other complementary therapies on chemotherapy-induced nausea and vomiting. The findings of the present study should be considered together with the limitations of the study. The number of breast cancer patients participating in the study reduces the coefficient of generalizability of the study results. It should be noted that the approximate time for this number of the samples (108 patients) to be entered in the study was 5 months. Moreover, the time limit for this intervention was another limitation for this study as for this student thesis.
Another limitation of this study was the research environment limitation. Because of this limitation, it was not possible to study other breast cancer patients in other hospitals at the same time. In fact, the research environment was the only research center affiliated to the Isfahan University of Medical Sciences that covers Isfahan and the surrounding cities. Due to the limitations of this study (including its small sample size, conducting this study in just one hospital, and the problems of generalizability of results), it is recommended that similar studies with larger sample sizes be performed at other hospitals.
ACKNOWLEDGMENT
This article is derived from master thesis of nursing. This research is registered in IRCT site as 2013080311136N2.
Footnotes
Source of Support: The Tarbiat Modares University, Tehran, Iran
Conflict of Interest: All authors declare that they have no conflict of interest
REFERENCES
- 1.Khodabakhshi R, Gohari MR, Fard ZM, Foadzi H, Vahabi N. Survival without disease in breast cancer patients and investigation of factors. Razi Med Sci J. 2012;18:28–33. [Google Scholar]
- 2.Gajizade SE, Najme ET. Investigation breast cancer risk factors by branch grapies. Iranian journal of nursing vision. 2011;77:61–8. [Google Scholar]
- 3.1th ed. Tehran: Ministery of Health and Medical Education; 2007. National report of cancer records, Ministery of Health and Medical Education, Center of Disease control and Preventation, Non-contagious Deputy, Cancer organ, The cancer organ. [Google Scholar]
- 4.Seied ME. Ms thesis. Tehran, Iran: Medical science Tehran University; 2011. Investigation effect of ginger on nausea and vomiting of cancer patients receiving chemotherapy. [Google Scholar]
- 5.Bakhshi M. Ms thesis. Tehran, Iran: Tarbiat Modares University; 2002. Effect of progressive muscle relaxation on acute and delayed emesis in cancer patients under chemotherapy in Institute cancer of Tehran at 2001. [Google Scholar]
- 6.Sontakke S, Thawani V, Naik M. Ginger as an antiemetic in nausea and vomiting induced by chemotherapy: A randomized, cross-over, double blind study. Indian J Pharm. 2003;35:32–6. [Google Scholar]
- 7.Cohen L, De Moor CA, Eisenberg P, Ming EE, Hu H. Chemotherapy-induced nausea and vomiting-incidence and impact on patient quality of life at community oncology settings. Support Care Cancer. 2007;15:497–503. doi: 10.1007/s00520-006-0173-z. [DOI] [PubMed] [Google Scholar]
- 8.Hickok JT, Roscoe JA, Morrow GR, Ryan JL. A phase II/III randomized, placebo-controlled, double-blind clinical trial of ginger (Zingiber officinale) for nausea caused by chemotherapy for cancer: A currently accruing URCC CCOP Cancer Control Study. Support Cancer Ther. 2007;4:247–50. doi: 10.3816/SCT.2007.n.022. [DOI] [PubMed] [Google Scholar]
- 9.Ghanbari A, Montazeri A, Niknami M, Atrkar Z, Sobhani A, Najafi B. Effect of using ginger beside routine treatment on nausea and vomiting of cancer patients in Razi hospital dependent to Medical scientific university of Rasht. Ardebil J. 2011;10:352–61. [Google Scholar]
- 10.Molassiotis A, Russell W, Hughes J, Breckons M, Lloyd-Williams M, Richardson J, et al. The Effectiveness of Acupressure for the Control and Management of Chemotherapy-Related Acute and Delayed Nausea: A Randomized Controlled Trial. J Pain Symptom Manage. 2014;47:12–25. doi: 10.1016/j.jpainsymman.2013.03.007. [DOI] [PubMed] [Google Scholar]
- 11.Ravanipour M. Ms thsis. Tehran, Iran: Tarbiat Modares university. Tehran; 1999. Effect of therapeutic touch before venipuncture on anxiety of school age children in medical centers of Bushehr city, 1998-99. [Google Scholar]
- 12.Freeman L. Mosby Elsevier publication; 2001. Complementary and alternative medicine: A research base approach; p. 456. [Google Scholar]
- 13.Zare Z. Ms thesis. Isfahan, Iran: Isfahan University; 2007. Investigation effect of therapeutic touch on level of anxiety before coronary artery bypass graft in Shiraz Namazi hospital 2005-2006. [Google Scholar]
- 14.Rankin D. The nurse handbook of complementary therapies. London: Bailliere Tindall; 2001. pp. 267–72. [Google Scholar]
- 15.Carpenter DS, Ambrose M, Holmes N. Professional guide to complementary and alternative therapy. United States: Spring house; 2002. pp. 475–7. [Google Scholar]
- 16.McCabe P. North Melbourne, Australia: Ausmed Education; 2001. Complementary therapy in nursing and midwifery, from vision to practice; pp. 497–504. [Google Scholar]
- 17.Movafaghi Z. Teherapeutic touch and its role in nursing. Mashhad Nurs Midwifery Fac J. 2006;18:66–9. [Google Scholar]
- 18.Zolfaghari M. Ms thesis. Tehran, Iran: Medical Scientific University of Tehran; 1999. Compariance of progressive muscle relaxation and therapeutic touch on anxiety, vital science and dysrhythmia under heart cathethrism. [Google Scholar]
- 19.Coakley AB, Barron AM. Energy Therapies in Oncology Nursing. Semin Oncol Nurs. 2012;28:55–63. doi: 10.1016/j.soncn.2011.11.006. [DOI] [PubMed] [Google Scholar]
- 20.Authers GO. Nurse's Handbook of alternative and complementary therapies. 8th ed. Philadelphia: Lippincott Williams and Wilkins; 2003. [Google Scholar]
- 21.Kuhn MA. Complementry for health care providers. Philadelphia: Lippincott and Williams; 1999. pp. 341–51. [Google Scholar]
- 22.DiNucci EM. Energy healing: A complementary treatment for orthopaedic and other conditions. Orthop Nurs. 2005;24:259–69. doi: 10.1097/00006416-200507000-00006. [DOI] [PubMed] [Google Scholar]
- 23.Bernand A. In: Halo therapy by remedial hands. Jalaliani, Mahyar, editors. Ketab: Donyaye Ketab Publication; 1377. pp. 20–45. [Google Scholar]
- 24.Smeltzer SC Bb, Hinke JL, Cheere KH, Kluwer W. Brunner and Sudarth's textbook of medical-surgical nursing. 12th ed. Philadelphia: Lippincot Williams and Wilkins; 2010. p. 337. (1460-1700). [Google Scholar]
- 25.Billhult A, Bergbom I, Stener-Victorin E. Massage relieves nausea in women with breast cancer who are undergoing chemotherapy. J Altern Complement Med. 2007;13:53–7. doi: 10.1089/acm.2006.6049. [DOI] [PubMed] [Google Scholar]
- 26.Najafi Ghazlaje, Rahimiha F. Investigation effect of foot massage on intensity of nausea at cancer patients. Breasr Dis J. 2004;3:14–8. [Google Scholar]
- 27.Post-White J, Kinney ME, Savik K, Gau JB, Wilcox C, Lerner I. Therapeutic Massage and Healing Touch Improve Symptoms in Cancer. Integr Cancer Ther. 2003;2:332–44. doi: 10.1177/1534735403259064. [DOI] [PubMed] [Google Scholar]
- 28.Roscoe JA, O’Neill M, Jean-Pierre P, Heckler CE, Kaptchuk TJ, Bushunow P, et al. An exploratory study on the effects of an expectancy manipulation on chemotherapy-related nausea. J Pain Symptom Manage. 2010;40:379–90. doi: 10.1016/j.jpainsymman.2009.12.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Dibble SL, Luce J, Cooper BA, Israel J, Cohen M, Nussey B, et al. Acupressure For Chemotherapy-Induced Nausea And Vomiting: A Randomized Clinical Trial. Oncol Nurs Soc. 2007;34:1–8. doi: 10.1188/07.ONF.xxx-xxx. [DOI] [PubMed] [Google Scholar]
- 30.Shen J, Glaspy J. Acupuncture: Evidence and implications for cancer supportive care. Cancer Pract. 2002;9:147–50. doi: 10.1046/j.1523-5394.2001.009003147.x. [DOI] [PubMed] [Google Scholar]
- 31.Matory P. Iran: Tarbiat Modares University; 2012. Investigation effects of therapeutic touch plane on induced-nausea in breast cancer women in 1391-92 in Isfahan Ms thesis. [Google Scholar]
- 32.Lewis H, Dirksen, O’Brien, Bucher . Mosby Elsevier; 2007. Medical surgical Nursing. 7. [Google Scholar]
- 33.Moafaghi Z. Therapeutic touch and nursing. Mashhad Nurs Midwifery Fac J. 2003;5:66–9. [Google Scholar]