

Abstract
Background:
Prevalence of work-related musculoskeletal disorders (WMSDs) is high among computer users. The study investigates the effect of three ergonomic interventions on the incidence of musculoskeletal disorders among the staff of Isfahan Province Gas Company, including training, sport, and installation of software.
Materials and Methods:
The study was performed in the summer of 2013 on 75 (52 men, 23 women) Isfahan Province Gas Company employees in three phases (phase 1: Evaluation of present situation, phase 2: Performing interventions, and phase 3: Re-evaluation). Participants were divided into three groups (training, exercise, and software). The Nordic Musculoskeletal Questionnaire (NMQ) and rapid upper limb assessment (RULA) were used. Data collected were analyzed using SPSS software and McNemar test, t-test, and Chi-square test.
Results:
Based on the evaluations, there was a decrease in musculoskeletal symptoms among the trained group participants after they received the training. McNemar test showed that the lower rate of pain in low back, neck, knee, and wrist was significant (P < 0.05). The results obtained from the RULA method for evaluation of posture showed an average 25 points decrease in the right side of the body and 20 points decrease in the left side of the body in the group subjected to training. Based on t-test, the decrease was significant.
Conclusion:
The study demonstrated that majority of the participants accepted interventions, which indicates that most of the people were unsatisfied with the work settings and seeking improvement at the workplace. Overall, the findings show that training, chair adjustment, and arrangement in workplace could decrease musculoskeletal disorders.
Keywords: Musculoskeletal risk, office ergonomic intervention, training
INTRODUCTION
Work-related musculoskeletal disorders (WMSDs) result from the workplace risk factors and are well known by the terms such as cumulative trauma disorders and repetitive strains injuries.[1] For people who spend a great deal of their time working on computer, these symptoms are common problems. Excessive computer usage results in increase of pain, itching, and numbness in shoulders, elbow, wrist, and hand.[2] In recent years, the use of computers has become necessary in jobs and there are very few occupations that do not require the use of computers.[3] The published scientific reports and papers show that the incidence of musculoskeletal disorders among computer users is much more than in other occupations.[4] Although there is a high interest shown in improving workplace conditions, there are very few longitudinal field trials that focus on the ergonomic interventions for the individual health of staff and individual productivity.[5]
Low back pain (LBP) is common among office workers in whom its incidence ranges from 23 to 38%.[6,7] The main cause of back pain is not entirely clear, but it seems that its origin is multi-factorial, and individual factors also, such as physical and mental health of an individual, can lead to its development and persistence.[8] The findings of one study showed that PC use increased risk of developing musculoskeletal disorders. Such an increase is mediated by ergonomic factors such as mouse use, remaining seated for prolonged periods, adoption of inadequate or uncomfortable postures, performing certain PC tasks, and psychosocial factors.[9] Sitting for more than half a day in an awkward position increases the likelihood of having LBP.[10]
A cross-sectional observational study assessed the pattern of musculoskeletal disorders suffered by bank workers in Kuwait. Of 750 employees, 80% suffered at least one episode of musculoskeletal disorders during the previous year and 42% suffered at least one disabling episode. The most affected body parts were the neck (53.5%), lower back (51.1%), shoulders (49.2%), and upper back (38.4%).[11] Jensen et al. showed that neck symptoms were the most common (53%) among female call center workers, followed by shoulder (42%) and hand/wrist (30%) symptoms.[12]
Improper design of work station has been shown to significantly contribute to LBP.[13] Various psychosocial problems, such as low job satisfaction,[13] high stress,[14] and effort–reward imbalance,[15] also contribute to an increased occurrence of LBP.
Chiung-Yu Cho et al. examined musculoskeletal symptoms and associated risk factors among office workers with high workload computer use. The three leading regions of musculoskeletal symptoms among the computer users were the shoulder (73%), neck (71%), and upper back (60%) areas. Similarly, the three leading regions of musculoskeletal symptoms among the computer users with high workload were shoulder (77.3%), neck (75.6%), and upper back (63.9%) regions.[16]
Few studies have been performed about the most effective ergonomic interventions to reduce musculoskeletal disorders and injuries.[17]
Several studies have examined various interventions. However, their effectiveness has been found to be different. Levels of evidence for interventions associated with positive effects were: Moderate evidence for arm supports and limited evidence for ergonomics training plus workstation adjustments, new chair, and rest breaks. Levels of evidence for interventions associated with “no effect” were: Strong evidence for workstation adjustment alone, moderate evidence for biofeedback training and job stress management training, and limited evidence for cognitive behavioral training. No interventions were associated with “negative effects.”[17]
Andersen et al. showed that specific resistance training and all-round physical exercise for office workers caused reduction in musculoskeletal pain symptoms in exposed regions of the upper body.[18]
Considering the above-mentioned issues, it is confirmed that continuously working on the computer for performing and accomplishing tasks in a sitting and sedentary position is considered one of the risk factors for the incidence of musculoskeletal disorders. Due to the prevalence of musculoskeletal problems in the Isfahan Province Gas Company staff, this study was designed. Hence, the present study was done among Isfahan Province Gas Company staff who had to spend a great deal of daily working time on computers to complete their work-related tasks. Because of the rising statistics of musculoskeletal complaints among employees of the company, on the gas company's request, this study was designed to determine the best method for reducing musculoskeletal problems.
The objective of this study was to find the best and most effective intervention, considering the ease of usage and work circumstances of the gas company.
MATERIALS AND METHODS
In this quasi-experimental study, 75 office employees of Isfahan Province Gas Company (52 men and 23 women) with at least 1 year work history were selected from the list of employees provided by human resources in the summer of 2013 with full consent.
The randomization process (without replacement) was performed by drawing numbered cards, each associated with a single potential participant.
Individuals participated in this study with complete willingness. In this study, unit staff headquarters, regions Khorasgan, Buildings 2 and 3, participated in this study. Attempts were made to balance demographic information, workload, and job descriptions as much as possible across the three groups. Workers were not randomly assigned to the study groups; our goal was to minimize the knowledge received about ergonomics and communication among the groups. Participants were, therefore, assigned to groups based on geographic separation by different units, floors, and buildings. People with previous history of health problems and accidents that had consequences on musculoskeletal disorders were excluded from our sample. Our study population worked in sitting position at least 6 h daily and spent 5 h of their working time doing computer tasks. Participants were divided into three groups of 25 individuals each, which are as follows:
Group subjected to training (T)
Group subjected to sport (S)
Software user group (N).
The first group (T) was subjected to a training session on the principles of ergonomics. For the second group (S), a period of exercises in pool was considered, and for the third group, software was installed to remind them of exercises during tasks in workplace, which are meant for a specific period of time.
In this study, the effects of three ergonomic interventions were assessed on lowering the musculoskeletal problems among computer users of the gas company. The study had three phases:
First phase: Assessment of existent situation (for 2 months)
Second phase: Applying interventions (2.5 months)
Third phase: Re-evaluation (2.5 months).
The assessment tools in this study were body posture evaluation by use of rapid upper limb assessment (RULA) method and Nordic Questionnaire. Previous studies have proven their reliability and validity.
In order to assess the incidence of musculoskeletal disorders, the standardised Nordic questionnaires for the analysis of musculoskeletal symptoms by Kuorinka and et al. was applied. Nowadays, this questionnaire is known as Nordic Questionnaire.[19]
RULA: The Rapid Upper Limb Assessment (RULA) is an observation-based screening tool that has been used to assess postural risks. In this method, coding and scoring are carried out by giving numbers or scribing letters and giving scores for body posture and parts of body such as neck, back, shoulders, elbow, wrist, low back, limb, knee, and ankles. The obtained scores from these sheets are the evidences to risk factors of the working position.[20] In this scheme, photography and taking picture were applied to record the individual posture.
In the first phase of the study, the Nordic Questionnaire was distributed among all participants and was collected a week later. Questionnaire information was analyzed using SPSS 18, McNemar test, t-test, and Chi-square test. After collecting the questionnaires, Photographs were taken of participants and the photos were evaluated by using RULA method. The second phase started and finished in 2.5 months after collecting information in the first phase and the interventions were done separately for each group.
Training intervention
Conducting various training courses is an important step toward creating an effective ergonomics platform in offices. Therefore, a training program based on the educational needs and previous training provided by the company is necessary. The objectives of the training were as follows: (1) Understanding office ergonomics principles;(2) self-evaluation of workplace conditions; and (3) arranging and organizing personal workspace. Multi-media presentation was provided for the trainees. The primary media presentation included PowerPoint slides showing pictures of various trainees’ computer workspaces. Trainees learned appropriate adjustments of chair and RULA method for 4 h.
Software using intervention
Prolonged sitting on a chair results in muscle weakness and pressure on the spine. By doing proper exercises during work time, it is possible to eliminate most of the work-related ergonomic injures. These exercises are designed keeping in mind the constraints in workplaces and should be done in a short period of time (even a few seconds) and, for many of them, there is no need to get up and stand. Therefore, after coordination with the company computer unit, the mentioned software was installed on the systems for the software user group. At regular intervals, the application reminds the user to exercise.
Sport intervention
For this group, a sport program was considered for 2–3 times a week with the consultation of a physiotherapist and the participants were made to perform specific exercises in water for 20 min by trained instructors. The main objective of this exercise was to strengthen the muscles around the spine.
In the third phase, first phase of the study was repeated after all interventions were applied completely. So, the sitting positions of all participants were photographed and images were assessed using RULA method. Also, Nordic questionnaires were distributed among participants and the collected information was analyzed for the second time. All obtained information and data and results were compared before and after the interventions. Three observers, all with a background in ergonomics, were trained on the RULA observational instrument. Observers were trained by one of the authors.
RESULTS
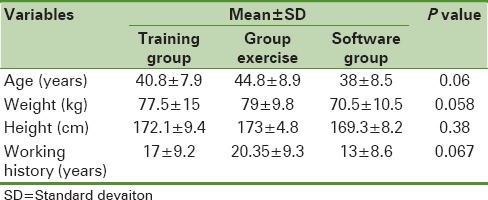
Some demographic information of the study population is presented in Table 1. Obtained data by Nordic Questionnaire from the first phase showed 53.3% of participants working 4–8 h and 15.6% working more than 8 h on computer daily.
Table 1.
Some demographic information of the sample groups (N=74)
There was no significant difference between the groups in terms of the level of education. Based on the results presented in Table 2, pain occurrence in low back and wrist in the previous 3 months and previous week was similar, which means the pain was chronic and is considered as an occupational risk factor. It has been shown that 58% and 39% of participants associated their job with pain in neck and LBP, respectively, and there was 24% and 15.2% absenteeism from work due to LBP and neck pain, respectively.
Table 2.
Results obtained from Nordic Questionnaire in phase 1 for the four groups

Also, it was found that 28.3% and 22.2% of physician office visits were due to LBP and neck pain, respectively.
Based on Chi-square test, there was a significant correlation between gender and prevalence of musculoskeletal disorders in shoulder and wrist (P = 0.038), that is, the reported complaints were higher among females compared to males.
The results for the incidence of musculoskeletal disorders for various body parts have been presented in Table 3. The results confirmed that training has the highest effect on lowering musculoskeletal problems. The decrease specifically was significant for low back, neck, knee, wrist, and back, based on McNemar test.
Table 3.
Incidence of musculoskeletal disorders before and after ergonomic interventions

To the questionnaires distributed in phase 3, some questions were added. One of the questions was “What is your idea about the intervention in which you are participating?”
The answers were categorized based on Likert scale; 99% of the group subjected to training showed their agreement with the intervention, 77% of the software using group approved the use of intervention, and 97% of the sport group showed agreement with the intervention.
The results obtained from the RULA method for evaluation of posture showed an average 25 points decrease in the right side of the body and 20 points decrease in the left side of the body in the group subjected to training. Based on paired samples t-test, the decrease in scores was significant (P ≤ 0.05), that is, an improvement in workplace was observed after the training intervention, but there was not any change in the other groups. With regard to the ergonomic training intervention questionnaire, the knowledge level of group T reached 83% from 13%, which resulted in workplace improvement (such as adjusting the height of chair, workload done, monitor and mouse adjustment, etc.). Based on Chi-square test, there was a significant correlation between knowledge and workplace improvement in group T, but there was no significant correlation found in the other groups that did not undergo under proper training with the workplace improvement [Figure 1].
Figure 1.
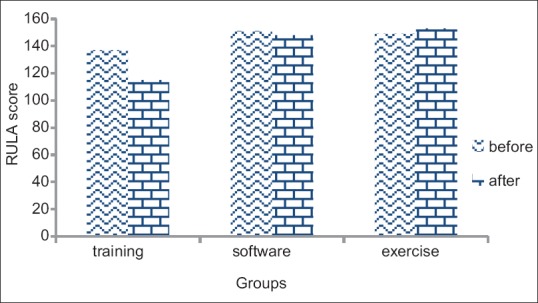
Change of RULA scores before and after intervention
DISCUSSION AND CONCLUSION
The study investigated the incidence of musculoskeletal disorders and the effects of ergonomic interventions to eliminate these disorders among the employees of Isfahan Province Gas Company. The study shows there is a high rate of musculoskeletal disorders in some body parts such as low back, neck, knee, and upper parts of the body. The higher rate of musculoskeletal disorders in these body parts is due to sedentary tasks and repetitive works. In many studies, sedentary and repetitive movements are considered as the major risk factor for the incidence of this type of disorders.[16,21]
Education intervention was effective in reducing pain in the lower back, neck, knee, wrist, and back, except shoulder. Also, software intervention was effective in reducing LBP and neck pain. Exercise intervention was effective in reducing pain in the lower back, wrist, and back.
Table 2 shows that back pain is the main cause of absenteeism from work. It provides a great deal of information to managers and demonstrates that preventing musculoskeletal-related factors could achieve higher productivity and job satisfaction among employees.
Also, comparing the results of the two groups, sport and software users (both interventions were exercise related), the question arises: “What is the reason for higher decrease in musculoskeletal problems observed in the sport group compared to the software users group?”
Sport and muscle strengthening is better done out of the workplace for companies with a high number of customers or high workload. Relying on only using the software and expecting improvement is not completely achievable, since it has been observed that during periods of high workload, computer users disconnect the program. However, we could not observe a significant correlation between sport and incidence of musculoskeletal disorders, but there was a significant positive correlation between sport and neck pain relief.[21]
Taieb-maimon et al. studied an intervention to examine the effectiveness of an innovative self-modeling photo-training method for reducing musculoskeletal risk among office workers using computers. They discovered that training had a greater effect on older workers and on workers suffering from higher degree of musculoskeletal pain.[22]
Robertson et al. showed that an educational intervention may possibly change the behaviors, mitigate symptoms, and enhance performance through training combined with a sit–stand workstation, which has implications for preventing discomfort among office workers.[23]
Kim et al. designed a participatory approach for improving the work environment. The purpose of this study was to develop an intervention to prevent WMSDs in hospital nurses using the participatory approach. The final intervention protocol consisted of a series of structured participant workshop, follow-up visits, and presentation of achievements.[23]
These results are consistent with those of Paolo Pillastrini et al. who showed that ergonomic intervention at the workstation improved work-related posture and was effective in reducing LBP point prevalence both in the first study period and after crossover.
In a study by Mesbah et al.,[24] no significant correlation was observed between sport and musculoskeletal disorders. Furthermore, it seems in the group subjected to training, there is a chance to cause proper changes with use of proper hand and wrist pattern and decrease of repetitive movement; the results show conformity with the results obtained by Ketola et al.[25] Also, Boor (2000) showed that receiving training could decrease musculoskeletal disorders and mental stress in the experimental group compared to control group. However, it has not been understood clearly whether this difference in the rate of pain and stress is the result of proper arrangement or improvement of body posture.[26]
In another study, a combination of many interventions was studied. These interventions included risk factor elimination, engineering control, managerial control, and training and increasing knowledge, and it has been approved that combination of interventions is more effective and results in decrease of musculoskeletal disorders.[27] The subject may pave the path for further research.
It may well be concluded that use of adjustable chairs in Isfahan Province Gas Company increases the effect of training and better sitting position and reduces WMSD signs. In the training group, the employees were encouraged to achieve an ergonomic fit with their chairs, as well as set up and arrange their workstations components, which was in conformity to the study done in one of the tax department of USA.[28] With the participant's increased knowledge, the RULA scores improved. Therefore, there is the potential to reduce musculoskeletal disorders. Participants in the training group created more appropriate behavioral changes in their workstation compared to those in the other groups.
It is noteworthy that most participants agreed with the intervention, which shows they were unsatisfied with the workplace conditions and were seeking changes. Even in the software using group in which there was the lowest rate of effectiveness, 77% showed their agreement to programs, and the highest rate of agreement was toward educational and training program (99%), which results in easier changes and further and extended interventions for the whole organization.
Overall, our findings demonstrate giving instructions on chair adjustment and proper arrangement in workplace may decrease musculoskeletal disorders. Many of the employees did not know the method of adjusting their chair before training and had been using them as they received them. Also, they did not use the capabilities of ergonomic chair. Because these chairs have great design capabilities and a person can adjust them to their own characteristics, adequate knowledge is required in the precise regulation of these seats.
Adjustment the workstation alone is not useful in reducing musculoskeletal problems, it must be accompanied with ergonomics training.[17]
The research provided evidences that ergonomic intervention should result in knowledge, body posture improvement, better workplace, and decrease of musculoskeletal disorders among office workers, and the findings could help in designing workplace interventions. This study may also be a preface for more investigations for the development of factors influencing the design of workplace.[29,30,31,32,33]
Limited time of personnel to participate in training courses, non-ergonomic desks, and low funding were the limitations of the project. Conflicting results on the impact of interventions suggest that it is better for any organization to choose the best ergonomic intervention considering its functionality and features.
Financial support and sponsorship
This is a research project funded by Isfahan Province Gas Company (research department).
Conflicts of interest
None declared.
Acknowledgments
This research was performed with the support and help of Isfahan Province Gas Company (research department). We acknowledge their assistance and efforts and show our appreciation to all Isfahan Province Gas Company employees for their support and participation in this research.
REFERENCES
- 1.Bernaards CM, Ariens GA, Hildebrandt VH. The (cost-) effectiveness of a lifestyle physical activity intervention in addition to a work style intervention on the recovery from neck and upper limb symptoms in computer workers. BMC Musculoskelet Disord. 2006;7:80. doi: 10.1186/1471-2474-7-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rempel D, Tittiranonda P, Burastero S, Hudes M, So Y. Effect of keyboard key-switch design on hand pain. J Occup Environ Med. 1999;41(2):111–9. doi: 10.1097/00043764-199902000-00006. [DOI] [PubMed] [Google Scholar]
- 3.poorghsemi A. Articles Collections of National Ergonomics Conference in Tehran manufacturing; 2002. Summary of Computer Applications in Ergonomics and introduction to some modeling software; p. 399. [Google Scholar]
- 4.Gerr F, Marcus M, Monteilh C. Epidemiology of musculoskeletal disorders among computer users: Lesson learned from the role of posture and keyboard use. Journal of Electromyography and Kinesiology. 2004;14:25–31. doi: 10.1016/j.jelekin.2003.09.014. [DOI] [PubMed] [Google Scholar]
- 5.Brewer S, Van Eerd D, Amick BC, III, Irvin E, Daum K, Gerr F, et al. Workplace interventions to prevent musculoskeletal and visual symptoms and disorders among computer users: A systematic review. J Occup Rehab. 2006;16:3. doi: 10.1007/s10926-006-9031-6. [DOI] [PubMed] [Google Scholar]
- 6.Janwantanakul P, Pensri P, Jiamjarasrangsri W, Sinsongsook T. Prevalence of self-reported musculoskeletal symptoms among office workers. Occup Med (Lond) 2008;58:436–8. doi: 10.1093/occmed/kqn072. [DOI] [PubMed] [Google Scholar]
- 7.Juul-Kristensen B, Sogaard K, Stroyer J, Jensen C. Computer users’ risk factors for developing shoulder, elbow and back symptoms. Scand J Work Environ Health. 2004;30:390–8. doi: 10.5271/sjweh.827. [DOI] [PubMed] [Google Scholar]
- 8.Manchikanti L. Epidemiology of low back pain. Pain Physician. 2000;3:167–92. [PubMed] [Google Scholar]
- 9.Ortiz-Hernández L, Tamez-González S, Martínez-Alcántara S, Méndez-Ramírez I. Computer use increases the risk of musculoskeletal disorders among newspaper office workers. Arch Med Res. 2003;34:331–41. doi: 10.1016/S0188-4409(03)00053-5. [DOI] [PubMed] [Google Scholar]
- 10.Lis AM, Black KM, Korn H, Nordin M. Association between sitting and occupational LBP. Eur Spine J. 2007;16:283–98. doi: 10.1007/s00586-006-0143-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Akrouf QAS, Crawford JO, Al-Shatti AS, Kamel MI. Musculoskeletal disorders among bank office workers in Kuwait. Eastern Mediterranean Health Journal. 2010:6. [PubMed] [Google Scholar]
- 12.Jensen C, Finsen L, Søgaard K, Christensen H. Musculoskeletal symptoms and duration of computer and mouse use. International Journal of Industrial Ergonomics. 2002;30(4):265–75. [Google Scholar]
- 13.Spyropoulos P, Papathanasiou G, Georgoudis G, Chronopoulos E, Koutis H, Koumoutsou F. Prevalence of low back pain in Greek public office workers. Pain Physician. 2007;10:651–9. [PubMed] [Google Scholar]
- 14.Yip YB, Ho SC, Chan SG. Socio-psychological stressors as risk factors for low back pain in Chinese middle-aged women. J Adv Nurs. 2001;36:409–16. doi: 10.1046/j.1365-2648.2001.01988.x. [DOI] [PubMed] [Google Scholar]
- 15.Rugulies R, Krause N. Effort-reward imbalance and incidence of low back and neck injuries in San Francisco transit operators. Occup Environ Med. 2008;65:525–33. doi: 10.1136/oem.2007.035188. [DOI] [PubMed] [Google Scholar]
- 16.Cho C-Y, Hwang Y-S, Cherng R-J. Musculoskeletal Symptoms and Associated Risk Factors Among Office Workers With High Workload Computer Use. Journal of Manipulative and Physiological Therapeutics. 2012;35(7):534–40. doi: 10.1016/j.jmpt.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 17.Kennedy CA, Amick BC, Dennerlein JT, Brewer S, Catli S, Williams R, et al. Systematic Review of the Role of Occupational Health and Safety Interventions in the Prevention of Upper Extremity Musculoskeletal Symptoms, Signs, Disorders, Injuries, Claims and Lost Time. 2010;20(2):127–62. doi: 10.1007/s10926-009-9211-2. [DOI] [PubMed] [Google Scholar]
- 18.Andersen LL, Christensen KB, Holtermann A, Poulsen OM, Sjøgaard G, Pedersen MT, et al. Effect of physical exercise interventions on musculoskeletal pain in all body regions among office workers: A one-year randomized controlled trial. Manual Therapy. 2010;15(1):100–4. doi: 10.1016/j.math.2009.08.004. [DOI] [PubMed] [Google Scholar]
- 19.Korinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sorensen F, Andersson G, et al. Standardized nordic questionnaires for the analysis of musculoskeletal symptoms. Applied Ergonomics. 1987;18(3):233–7. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 20.McAtamney L, Corlett E, Rula N. A survey method for the investigation of work-related upper limb disorders. Applied Ergonomics. 1993;24(2):91–9. doi: 10.1016/0003-6870(93)90080-s. [DOI] [PubMed] [Google Scholar]
- 21.Kennedy CA, Amick BC, Dennerlein JT, Brewer S, Catli S, Williams R, et al. Systematic Review of the Role of Occupational Health and Safety Interventions in the Prevention of Upper Extremity Musculoskeletal Symptoms, Signs, Disorders, Injuries, Claims and Lost Time. Journal of Occupational Rehabilitation. 2010;20(2):127–62. doi: 10.1007/s10926-009-9211-2. [DOI] [PubMed] [Google Scholar]
- 22.Taieb-Maimon M, Cwikel J, Shapira B, Orenstein I. The effectiveness of a training method using self-modeling webcam photos for reducing musculoskeletal risk among office workers using computers. Applied Ergonomics. 2012;43(2):376–85. doi: 10.1016/j.apergo.2011.05.015. [DOI] [PubMed] [Google Scholar]
- 23.Kim S-L, Lee J-E. Development of an intervention to prevent work-related musculoskeletal disorders among hospital nurses based on the participatory approach Applied ergonomics. 2010;41(3):454–60. doi: 10.1016/j.apergo.2009.09.007. [DOI] [PubMed] [Google Scholar]
- 24.Mesbah F, Choobineh A, Tozihian Ms, Peyman J, Naghibalhosseini F, Shidmosavi M, et al. Ergonomic intervention effect in reducing musculoskeletal disorders in staff of Shiraz Medical School. Iran occupational health. 2012;9:1. [Google Scholar]
- 25.Ketola R, Toivonen R, Hakkanen M, Luukkonen R, Takala E, Viikari-Juntura E, et al. Effects of ergonomic intervention in work with video display units. Scand JWork Environ Health. 2002;28(1):18–24. doi: 10.5271/sjweh.642. [DOI] [PubMed] [Google Scholar]
- 26.Bohr P. Efficacy of office ergonomics education. J Occup Rehab. 2000;10(4):243–55. [Google Scholar]
- 27.Stetler CB, Burns M, Sander-Buscemi K. Use of evidence for prevention of work-related musculoskeletal injuries. Journal of Orthop Nurs. 2003;22(1):32–41. doi: 10.1097/00006416-200301000-00010. [DOI] [PubMed] [Google Scholar]
- 28.Robertson M, Amick BC, DeRango K, Rooneyd T, Bazzanid L, Harriste R, et al. The effects of an office ergonomics training and chair intervention on worker knowledge, behavior and musculoskeletal risk. Applied ergonomics. 2009;40:124–35. doi: 10.1016/j.apergo.2007.12.009. [DOI] [PubMed] [Google Scholar]
- 29.Habibi E, Soury S, Hasanzadeh A. Precise Evaluation of Anthropometric 2D Software Processing of Hand in Comparison with Direct Method. J Med Sign Sens. 2012;3(195):256–61. [PMC free article] [PubMed] [Google Scholar]
- 30.Habibi E, Zare M, Amini NR, Pourabdian S, Rismanchian M. Macroergonomic conditions and job satisfaction among employees of an industry. Int J Env Health Eng. 2012;1:34. [Google Scholar]
- 31.Habibi E, Pourabdian S, Atabaki AK, Hoseini M. Evaluation of workrelated psychosocial and ergonomics factors in relation to low back discomfort in emergency unit nurses. Int J Prev Med. 2012;3:564–8. [PMC free article] [PubMed] [Google Scholar]
- 32.Habibi E, Zare M, Haghi A, Habibi P, Hassanzadeh A. Assessment of physical risk factors among artisans using occupational repetitive actions and Nordic questionnaire. Int J Env Health Eng. 2013;2:14. [Google Scholar]
- 33.Azmoon H, Dehghan H, Akbari J, Soury S. The Relationship between Thermal Comfort and Light Intensity with Sleep Quality and Eye Tiredness in Shift Work Nurses. Journal of Environmental and Public Health 2013. 2013:5. doi: 10.1155/2013/639184. [DOI] [PMC free article] [PubMed] [Google Scholar]