

Abstract
Background
As the U.S. population grows older, there is greater need to examine physical independence. Previous studies have assessed risk factors in relation to either disability or mortality, but an outcome that combines both is still needed.
Methods and Results
The Cardiovascular Health Study is a population‐based, prospective study where participants underwent baseline echocardiogram, measurement of carotid intima‐media thickness (IMT), and various biomarkers, then followed for up to 18 years. Years of able life (YAL) constituted the number of years the participant was able to perform all activities of daily living. Linear regression was used to model the relationship between selected measures and outcomes, adjusted for confounding variables. Among 4902 participants, mean age was 72.6±5.4 years, median YAL for males was 8.8 (interquartile range [IQR], 4.3 to 13.8) and 10.3 (IQR, 5.8 to 15.8) for females. Reductions in YAL in the fully adjusted model for females and males, respectively, were: −1.34 (95% confidence interval [CI], −2.18, −0.49) and −1.41 (95% CI, −2.03, −0.8) for abnormal left ventricular (LV) ejection fraction, −0.5 (95% CI, −0.78, −0.22) and −0.62 (95% CI, −0.87, −0.36) per SD increase in LV mass, −0.5 (95% CI, −0.7, −0.29) and −0.79 (95% CI, −0.99, −0.58) for IMT, −0.5 (95% CI, −0.64, −0.37) and −0.79 (95% CI, −0.94, −0.65) for N‐terminal pro‐brain natriuretic peptide, −1.08 (95% CI, −1.34, −0.83) and −0.73 (95% CI, −0.97, −0.5) for high‐sensitivity troponin‐T, and −0.26 (95% CI, −0.42, −0.09) and −0.23 (95% CI, −0.41, −0.05) for procollagen‐III N‐terminal propeptide. Most tested variables remained significant even after adjusting for incident cardiovascular (CV) disease.
Conclusions
In this population‐based cohort, variables obtained by CV imaging and biomarkers of inflammation, coagulation, atherosclerosis, myocardial injury and stress, and cardiac collagen turnover were associated with YAL, an important outcome that integrates physical ability and longevity in older persons.
Keywords: activities of daily living, aging, biomarkers, imaging
Introduction
The concept of “healthy” or “successful” aging has been the subject of research for decades. It lacks a universal definition, however, because older adults’ perception of healthy aging is heterogeneous and might not be in complete accord with scientific definitions.1–2 Nevertheless, maintenance of physical ability remains a consistent component in any definition. Given that the number of persons 85 and older is projected to double and reach 19 million by 2025,3 investigating determinants of mortality is of great importance—but preserving physical ability, a marker of independence, is a key goal for healthy aging. In fact, older persons rank maintaining independence as more important than staying alive as a health outcome.4 Cardiovascular (CV) well‐being is at the center of this paradigm.
Functional decline undermines quality of life and causes substantial social and economic strain on patients and their families. Impairment of physical ability can occur at any point in time in individuals with chronic diseases. This varies depending on the burden of comorbidities and many other complex factors that are poorly understood.5 Although many traditional risk factors correlate with mortality, untangling their role in developing functional impairment has proven difficult because diseases that lead to death often accelerate functional decline.6 Thus, devising a health outcome that combines both longevity and functional ability is more relevant to patient interests than either alone. Furthermore, this health outcome should preferably take into account that some subjects move in and out of the disabled state.
Disability results from complex and heterogeneous processes in older persons. We hypothesized that CV imaging measures of left ventricular (LV) structure and function, carotid intima thickness, and biomarkers of inflammation, coagulation, atherosclerosis, myocardial injury and stress, and cardiac extracellular collagen turnover are not only associated with mortality, but also with the likelihood of maintaining physical ability in a large sample of community‐dwelling older persons.
Methods
Study Population
The Cardiovascular Health Study (CHS) is a community‐based, prospective, observational study that recruited adults ≥65 years to study risk factors and long‐term outcomes for CV disease (CVD). The cohort included 5888 participants (5201 were recruited in 1989–1990; an additional 687 African Americans were recruited in 1992–1993). The institutional review board at each center approved the study, and all participants provided informed consent. Participants underwent baseline clinical examinations, which included medical history, physical examination, assessment of activities of daily living (ADLs), and various imaging and laboratory procedures. Participants were contacted every 6 months for follow‐up, alternating between a telephone interview and a clinic visit through 1999, and only phone calls thereafter (Figure). The design, rationale, and examination details of the CHS have been published elsewhere.7
Figure 1.
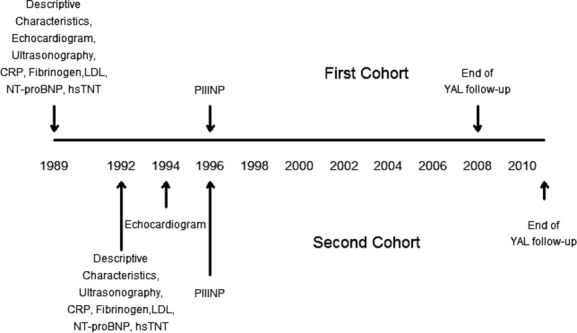
Time chart of enrollment of the first cohort and second (African‐American) cohort, in addition to timing of performing the cardiovascular imaging and measurement of the biomarkers in the Cardiovascular Health Study. CRP indicates C‐reactive protein; hsTNT, high‐sensitivity cardiac troponin‐T; LDL, low‐density lipoprotein; NT‐proBNP, N‐terminal probrain natriuretic peptide; PIIINP, procollagen III N‐terminal propeptide; YAL, years of able life.
Imaging Procedures
Transthoracic echocardiograms were obtained in 1989–1990 for the original cohort and 1994–1995 for the African‐American cohort. Semiquantitative LV ejection fraction (LVEF), left atrial (LA) diameter, transmitral mitral peak early (E) velocity, peak atrial (A) velocity, and E/A ratio, LV relative wall thickness (LV RWT), and LV mass were defined using previously specified criteria.8
The carotid arteries were evaluated at baseline with high‐resolution B‐mode ultrasonography. A composite measure that combined the maximum common carotid artery intima media thickness (IMT) and maximum internal IMT was obtained by averaging these 2 measurements after standardization. When present, focal plaques were included in measurement of the maximum IMT.9
Biomarker Assays
Biomarkers used in this study were obtained from baseline blood samples, except for procollagen III N‐terminal propeptide (PIIINP), which was assayed from blood collected in 1996–1997. Samples were immediately centrifuged at 3000g for 10 minutes at 4°C. Aliquots of plasma were stored in a central laboratory at −70°C. C‐reactive protein (CRP) was measured by a high‐sensitivity (hs) immunoassay, with an interassay coefficient of variation of 6.25%.
N‐terminal probrain natriuretic peptide (NT‐proBNP) was measured with the Elecsys 2010 system (Roche Diagnostics, Indianapolis, IN) with a coefficient of variation of 2% to 5%. High‐sensitivity cardiac troponin‐T (hsTNT) concentrations were measured with reagents on an Elecsys 2010 analyzer (Roche Diagnostics, Indianapolis, IN), with an analytical measurement range of 3 to 10 000 pg/mL. The value at the 99th percentile cutoff from a healthy reference population (n=616) was 13.5 pg/mL. PIIINP was determined by a coated‐tube radioimmunoassay as described previously using commercial antisera specifically directed against the amino terminal peptide (Orion Diagnostica, Espoo, Finland). Inter‐ and intraassay variations for determining PIIINP are both approximately 5%. Sensitivity (lower detection limit) is 1.5 ng/mL.
Clinical Endpoints and Variable Definitions
The primary outcome, years of able life (YAL), was defined as the number of years that the participant is able to perform all 6 ADLs without difficulty: walking around the home; getting out of bed or a chair; eating; dressing; and bathing or showering or using the toilet. This definition allows for recovery from difficulty. We chose ADLs because difficulty to perform any of them makes it unlikely that a person is able to maintain physical independence. Years of life (YOL) was defined as years of observed life from enrollment to death or end of follow‐up (maximum 18 years).
Data on mortality and self‐reported limitations in ADLs were collected every 6 months, with some exceptions mentioned in Data S1. Calculation and imputation of YOL and YAL are also included in Data S1. Given that many of the tested variables have been associated with mortality and/or physical disability, we evaluated the secondary outcome, the percentage of YAL:YOL, which was defined as the percentage of observed years spent free of impairment in ADLs (Data S1).
Statistical Analysis
We excluded participants who reported any ADL difficulty at baseline (N=436) or did not have LVEF, LA dimension, peak E velocity, or peak A velocity measures (N=550). We did not exclude participants with prevalent coronary heart disease (CHD) because many of these participants had preserved ADL, and including them is more representative of older cohorts who have higher burden of disease. The analysis set was therefore composed of 4902 participants. Previously imputed data were employed for missing covariate data (Data S1). Further exclusions were made based on the availability of biomarker and echocardiography data: LV mass and LV RWT measures were available for 3374 participants, NT‐proBNP was available for 3776 participants, hsTnT was available for 3694 participants, and PIIINP was available for 3173 participants.
We used multiple linear regression procedures to model the relationship between exposures of interest and outcome measures YAL and YOL, stratified by sex. For each outcome, we ran 2 sets of models. The first set was adjusted for age, race, body mass index (BMI), and BMI‐squared. The second set was additionally adjusted for prevalent smoking, arthritis, diabetes, cancer, glomerular filtration rate (eGFR), systolic blood pressure (SBP), antihypertensive medication use, stroke, congestive heart failure (CHF), and CHD, which included myocardial infarction (MI), angina, and revascularization (see Data S1 for definitions). LVEF, LA dimension, peak E velocity, peak A velocity, E/A ratio, LV mass, LV RWT, carotid IMT, hsCRP, fibrinogen, low‐density lipoprotein (LDL) cholesterol, NT‐proBNP, PIIINP, and hsTNT were evaluated in separate models one at a time. Because the associations of interest have not been shown previously, we wanted to look at each marker individually. No significant multicollinearity was detected in the models. Outliers did not exert significant leverage, and in cases where inference changed, the values of outliers were deemed reasonable and were retained in the models.
PIIINP was evaluated at 7 and 4 years after baseline for the original and minority cohorts, respectively (year 1996–1997) for 3173 participants. Thus, YAL could only have a maximum of 11 years in the PIIINP analyses, as compared with 18 years for the other analyses.
Additionally, sensitivity analysis by the time to the first ADL difficulty using Cox proportional hazard models was performed, adjusted for the 2 sets of covariates used in the primary analysis, and further adjusted for incident CHF, MI, and stroke. Compared to the primary analysis, this approach would fail to capture persons who regain physical ability after an acute insult (e.g., MI or stroke), but would allow us to adjust for incident disease, which would help to rule out associations that were solely owing to incident events. A total of 1099 participants had an incident CVD before developing ADL difficulty.
Results
Baseline Characteristics
For the 4902 participants in our study, mean (±SD) age was 72.6±5.4 years. Median YAL was 8.8 (interquartile range [IQR], 4.3 to 13.8) years for males and 10.3 (IQR, 5.8 to 15.8) years for females. Median YOL was 11.8 (IQR, 6.8 to 17.8) years for males and 15.3 (IQR, 9.8 to 18) years for females.
At baseline, 18.4% of the participants had CHD (24.6% in males and 13.5% in females) and 3.55% had CHF (4.6% in males and 2.7% in females), whereas 13.5% of men and 4.7% of women had abnormal LVEF.
Baseline characteristics of participants per categories of YAL are shown in Tables 1 and 2. Compared to the lowest category, subjects in the highest category of YAL were younger (69.9 vs. 76 years for males and 69.5 vs. 75.4 years for females), never smoked, and had less prevalent CHD, CHF, stroke, diabetes, hypertension (HTN), hypertensive medication use, and arthritis. Additionally, subjects in the highest category of YAL had smaller IMT and lower detectable values of all biomarkers, except LDL, which was higher.
Table 1.
Baseline Characteristics by Categories of Years of Able Life for Male and Female Participants in CHS
| Characteristics at Baseline | Categories of Years of Able Life | |||||||
|---|---|---|---|---|---|---|---|---|
| Males (n=2133) | Females (n=2769) | |||||||
| 0 to <5 | 5 to <10 | 10 to <15 | 15 to 18 | 0 to <5 | 5 to <10 | 10 to <15 | 15 to 18 | |
| n=586 | n=660 | n=397 | n=490 | n=551 | n=814 | n=614 | n=790 | |
| Age, y±SD | 76±6.4 | 73.7±5.5 | 71.8±4.3 | 69.9±3.4 | 75.4±6 | 73.3±5.3 | 71.2±4.2 | 69.5±3.4 |
| Black, n (%) | 54 (9.2) | 82 (12.4) | 34 (8.6) | 57 (11.6) | 81 (14.7) | 113 (13.9) | 73 (11.9) | 96 (12.2) |
| BMI (kg/m2), mean±SD | 26.1±3.8 | 26.3±3.7 | 26.8±3.6 | 26.3±3.2 | 26.5±5.5 | 26.6±5.2 | 26.6±4.8 | 26.2±4.2 |
| Smoking status, n (%) | ||||||||
| Never | 172 (29.4) | 201 (30.5) | 133 (33.5) | 190 (38.8) | 298 (54.1) | 450 (55.3) | 353 (57.5) | 472 (59.7) |
| Former | 345 (58.9) | 387 (58.6) | 225 (56.7) | 271 (55.3) | 167 (30.3) | 262 (32.2) | 193 (31.4) | 231 (29.2) |
| Current | 69 (11.8) | 72 (10.9) | 39 (9.8) | 29 (5.9) | 86 (15.6) | 102 (12.5) | 68 (11.1) | 87 (11) |
| CHD, n (%) | 209 (35.7) | 168 (25.5) | 77 (19.4) | 72 (14.7) | 127 (23) | 125 (15.4) | 71 (11.6) | 51 (6.5) |
| CHF, n (%) | 58 (9.9) | 29 (4.4) | 6 (1.5) | 5 (1) | 38 (6.9) | 23 (2.8) | 10 (1.6) | 5 (0.6) |
| Stroke, n (%) | 52 (8.9) | 33 (5) | 9 (2.3) | 9 (1.8) | 32 (5.8) | 17 (2.1) | 8 (1.3) | 3 (0.4) |
| Diabetes ADA status, n (%) | ||||||||
| Normal | 355 (60.6) | 437 (66.2) | 284 (71.5) | 390 (79.6) | 370 (67.2) | 614 (75.4) | 478 (77.9) | 649 (82.2) |
| IFG | 74 (12.6) | 87 (13.2) | 64 (16.1) | 56 (11.4) | 63 (11.4) | 87 (10.7) | 75 (12.2) | 88 (11.1) |
| Diabetes | 157 (26.8) | 136 (20.6) | 49 (12.3) | 44 (9) | 118 (21.4) | 113 (13.9) | 61 (9.9) | 53 (6.7) |
| SBP | 140±22.7 | 137.9±21 | 135.3±20.3 | 132.7±19.4 | 143±24.1 | 139.2±21.9 | 135.9±20.3 | 132.1±19.3 |
| Hypertensive medication, n (%) | 314 (53.6) | 293 (44.4) | 167 (42.1) | 169 (34.5) | 316 (57.4) | 410 (50.4) | 258 (42) | 289 (36.6) |
| eGFR by creatinine | 62.7±19.4 | 66.4±16.8 | 69.4±15.7 | 70.7±15.2 | 66.1±19.9 | 69.6±18.8 | 69.8±16.8 | 71.5±15.7 |
| Arthritis, n (%) | 295 (50.3) | 270 (40.9) | 178 (44.8) | 157 (32) | 347 (63) | 440 (54.1) | 356 (58) | 344 (43.5) |
| Cancer, n (%) | 104 (17.8) | 96 (14.6) | 48 (12.1) | 69 (14.1) | 101 (18.3) | 130 (16.0) | 68 (11.1) | 79 (10.0) |
ADA indicates American Diabetes Association; BMI, body mass index; CHD, coronary heart disease (myocardial infarction, angina, coronary artery bypass grafting, or angioplasty); CHF, congestive heart failure; CHS, Cardiovascular Health Study; eGFR, estimated glomerular filtration rate; IFG, impaired fasting glucose; SBP, systolic blood pressure.
Table 2.
Baseline Cardiovascular Imaging and Biomarkers by Categories of Years of Able Life for Male and Female Participants in CHS
| Categories of Years of Able Life | ||||||||
|---|---|---|---|---|---|---|---|---|
| Males (n=2133) | Females (n=2769) | |||||||
| 0 to <5 | 5 to <10 | 10 to <15 | 15 to 18 | 0 to <5 | 5 to <10 | 10 to <15 | 15 to 18 | |
| n=586 | n=660 | n=397 | n=490 | n=551 | n=814 | n=614 | n=790 | |
| Cardiovascular imaging | ||||||||
| Abnormal LVEF (<55%), n (%) | 119 (20.31) | 94 (14.24) | 40 (10.08) | 35 (7.14) | 54 (9.8) | 38 (4.67) | 22 (3.58) | 16 (2.03) |
| LA dimension (mm), mean±SD | 4.14±0.76 | 4±0.71 | 4.02±0.59 | 3.94±0.58 | 3.87±0.74 | 3.78±0.63 | 3.75±0.61 | 3.67±0.57 |
| Peak E velocity (m/s), mean±SD | 0.69±0.21 | 0.67±0.18 | 0.67±0.15 | 0.69±0.15 | 0.75±0.24 | 0.74±0.18 | 0.74±0.18 | 0.73±0.16 |
| Peak A velocity (m/s), mean±SD | 0.77±0.27 | 0.75±0.22 | 0.72±0.19 | 0.71±0.18 | 0.89±0.26 | 0.85±0.22 | 0.81±0.22 | 0.78±0.19 |
| E/A ratio, n (%) | ||||||||
| <0.7 | 183 (31.23) | 143 (21.67) | 45 (11.34) | 51 (10.41) | 159 (28.86) | 176 (21.62) | 97 (15.8) | 98 (12.41) |
| 0.7, 1.5 | 339 (57.85) | 471 (71.36) | 326 (82.12) | 402 (82.04) | 356 (64.61) | 601 (73.83) | 492 (80.13) | 658 (83.29) |
| ≥1.5 | 64 (10.92) | 46 (6.97) | 26 (6.55) | 37 (7.55) | 36 (6.53) | 37 (4.55) | 25 (4.07) | 34 (4.3) |
| LV mass (g/m2), mean±SD | 190.6±68.2 | 177.1±53.4 | 169.3±46.8 | 162.9±42.2 | 147.6±56.7 | 135.7±42.9 | 131.2±33.2 | 127.0±30.7 |
| LV RWT, mean±SD | 0.36±0.1 | 0.35±0.08 | 0.34±0.08 | 0.34±0.07 | 0.37±0.11 | 0.36±0.08 | 0.35±0.07 | 0.34±0.07 |
| IMT (mm), mean±SD | 1.5±0.4 | 1.3±0.3 | 1.3±0.3 | 1.2±0.3 | 1.3±0.4 | 1.2±0.3 | 1.1±0.3 | 1.1±0.3 |
| Biomarkers | ||||||||
| hsCRP (mg/L), median IQR |
2.23 1.15 to 4.09 |
1.75 0.88 to 3.47 |
1.72 0.92 to 2.86 |
1.38 0.68 to 2.44 |
2.46 1.22 to 4.64 |
1.97 0.92 to 3.45 |
1.88 0.94 to 3.25 |
1.72 0.88 to 3.00 |
| Fibrinogen (mg/dL), mean±SD | 334±75.3 | 314.7±67 | 315.4±63.1 | 304.2±59.3 | 330.9±72.6 | 321.9±61.3 | 324.7±64.6 | 315.4±59.2 |
| LDL (mg/dL), mean±SD | 119.9±36.1 | 120.2±32.5 | 125.7±33.1 | 128.9±32.3 | 132.6±38.9 | 133.8±37.9 | 132.9±37.2 | 137.9±35.8 |
| NT‐proBNP (pg/mL), median IQR |
210 105 to 546 |
118 56 to 239 |
80 38 to 153 |
60 35 to 119 |
186 83 to 378 |
134 72 to 241 |
104 63 to 179 |
82 46 to 145 |
| hsTNT (ng/mL), median IQR |
11.25 6.70 to 18.76 |
8.90 4.95 to 14.68 |
6.58 2.99 to 10.07 |
5.78 2.99 to 8.99 |
6.62 2.99 to 12.23 |
4.48 2.99 to 7.78 |
3.45 2.99 to 5.87 |
2.99 2.99 to 4.26 |
| PIIINP (ng/mL), mean±SD | 5.18±1.98 | 4.98±1.70 | 4.71±1.90 | — | 4.94±1.92 | 4.63±1.55 | 4.38±1.29 | — |
A indicates atrial filling; CHS, Cardiovascular Health Study; E, early filling; hsCRP, high‐sensitivity C‐reactive protein; hsTNT, high‐sensitivity troponin‐T; IMT, carotid intima‐media thickness; IQR, interquartile range; LA, left atrium; LDL, low‐density lipoprotein; LV, left ventricular; LVEF, left ventricular ejection fraction; NT‐proBNP, N‐terminal probrain natriuretic peptide; PIIINP, procollagen III N‐terminal Propeptide; LV RWT, left ventricular relative wall thickness.
Imaging
An abnormal LVEF was associated with 2.49 and 2.38 fewer observed YAL and 3.14 and 2.51 fewer observed YOL in females and males, respectively (P<0.001), after adjustment for age, race, and BMI (Tables 3 and 4). This association remained strong and statistically significant after adjustment for chronic health conditions at baseline. Persons with abnormal LVEF had 1.34 and 1.41 fewer observed YAL and 2.08 and 1.41 fewer observed YOL in females and males, respectively (P<0.01). Furthermore, male participants with an abnormal LVEF spent 3.6% less of their observed years of life being able (P=0.01). However, this relationship was not significant for female participants (P=0.3; Table S1).
Table 3.
Linear Regression Results of Adjusted Cardiovascular Imaging Risk Factors for YAL and YOL for Female Participants in CHS (n=2769)
| Cardiovascular Imaging | Years of Able Life | Years of Life | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||
| Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | |
| Abnormal LVEF (<55%) | −2.49 (−3.35, −1.64) | <0.001 | −1.34 (−2.18, −0.49) | 0.002 | −3.14 (−3.93, −2.36) | <0.001 | −2.08 (−2.85, −1.31) | <0.001 |
| LA dimension (per SD=0.67) | −0.37 (−0.57, −0.17) | <0.001 | −0.2 (−0.4, 0) | 0.045 | −0.32 (−0.5, −0.13) | 0.001 | −0.16 (−0.34, 0.02) | 0.08 |
| Peak E velocity (per SD=0.19) | −0.27 (−0.45, −0.09) | 0.003 | −0.15 (−0.32, 0.03) | 0.097 | −0.24 (−0.41, −0.08) | 0.004 | −0.13 (−0.28, 0.03) | 0.115 |
| Peak A velocity (per SD=0.23) | −0.45 (−0.64, −0.26) | <0.001 | −0.3 (−0.49, −0.12) | 0.001 | −0.45 (−0.62, −0.27) | <0.001 | −0.31 (−0.48, −0.14) | <0.001 |
| E/A ratio | <0.001 | 0.027 | <0.001 | <0.001 | ||||
| <0.7 | −0.98 (−1.46, −0.51) | <0.001 | −0.58 (−1.04, −0.12) | 0.013 | −1.2 (−1.63, −0.76) | <0.001 | −0.82 (−1.23, −0.4) | <0.001 |
| 0.7, <1.5 | Ref | — | Ref | — | Ref | — | Ref | — |
| ≥1.5 | −1.18 (−2.03, −0.33) | 0.007 | −0.54 (−1.36, 0.28) | 0.198 | −1.63 (−2.41, −0.85) | <0.001 | −1.07 (−1.83, −0.32) | 0.005 |
| LV mass (per SD=51.17) | −0.91 (−1.19, −0.63) | <0.001 | −0.5 (−0.78, −0.22) | 0.001 | −1.09 (−1.34, −0.84) | <0.001 | −0.76 (−1.02, −0.51) | <0.001 |
| LV RWT (per SD=0.08) | −0.26 (−0.48, −0.04) | 0.019 | −0.17 (−0.38, 0.04) | 0.12 | −0.31 (−0.51, −0.11) | 0.002 | −0.22 (−0.41, −0.03) | 0.023 |
| IMT (per SD=0.34) | −0.89 (−1.09, −0.69) | <0.001 | −0.5 (−0.7, −0.29) | <0.001 | −0.92 (−1.1, −0.73) | <0.001 | −0.53 (−0.72, −0.34) | <0.001 |
Model 1 adjusted for age, race, and BMI. Model 2 additionally adjusted for prevalent smoking, arthritis, cancer, diabetes ADA status, eGFR, antihypertensive medication use, systolic blood pressure, congestive heart failure, stroke, and coronary heart disease (myocardial infarction, angina, coronary artery bypass grafting, or angioplasty). A indicates atrial filling; ADA, American Diabetes Association; BMI, body mass index; CHS, Cardiovascular Health Study; CI, confidence interval; E, early filling; eGFR, estimated glomerular filtration rate; IMT, carotid intima‐media thickness; LA, left atrium; LVEF, left ventricular ejection fraction; LV RWT, left ventricular relative wall thickness; YAL, years of able life; YOL, years of life.
Table 4.
Linear Regression Results of Adjusted Cardiovascular Imaging Risk Factors for YAL and YOL for Male Participants in CHS (n=2133)
| Cardiovascular Imaging Variables | Years of Able Life | Years of Life | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||
| Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | |
| Abnormal LVEF (<55%) | −2.38 (−3.01, −1.76) | <0.001 | −1.41 (−2.03, −0.8) | <0.001 | −2.51 (−3.13, −1.89) | <0.001 | −1.41 (−2.02, −0.8) | <0.001 |
| LA dimension (per SD=0.67) | −0.49 (−0.71, −0.27) | <0.001 | −0.24 (−0.45, −0.04) | 0.022 | −0.52 (−0.73, −0.3) | <0.001 | −0.24 (−0.45, −0.03) | 0.026 |
| Peak E velocity (per SD=0.19) | −0.17 (−0.39, 0.06) | 0.146 | −0.01 (−0.22, 0.2) | 0.93 | −0.25 (−0.47, −0.02) | 0.032 | −0.08 (−0.29, 0.13) | 0.46 |
| Peak A velocity (per SD=0.23) | −0.28 (−0.5, −0.06) | 0.014 | −0.14 (−0.35, 0.07) | 0.18 | −0.31 (−0.53, −0.09) | 0.006 | −0.19 (−0.4, 0.02) | 0.072 |
| E/A ratio | <0.001 | <0.001 | <0.001 | <0.001 | ||||
| <0.7 | −1.93 (−2.48, −1.37) | <0.001 | −1.35 (−1.88, −0.83) | <0.001 | −2.18 (−2.73, −1.63) | <0.001 | −1.6 (−2.12, −1.08) | <0.001 |
| 0.7, <1.5 | Ref | — | Ref | — | Ref | — | Ref | — |
| ≥1.5 | −1.58 (−2.37, −0.8) | <0.001 | −0.88 (−1.62, −0.13) | 0.021 | −1.98 (−2.76, −1.2) | <0.001 | −1.18 (−1.92, −0.44) | 0.002 |
| LV mass (per SD=51.17) | −1 (−1.26, −0.74) | <0.001 | −0.62 (−0.87, −0.36) | <0.001 | −1.11 (−1.36, −0.85) | <0.001 | −0.72 (−0.97, −0.47) | <0.001 |
| LV RWT (per SD=0.08) | −0.15 (−0.42, 0.12) | 0.287 | −0.16 (−0.42, 0.1) | 0.225 | −0.13 (−0.4, 0.14) | 0.35 | −0.13 (−0.38, 0.12) | 0.312 |
| IMT (per SD=0.34) | −1.27 (−1.47, −1.06) | <0.001 | −0.79 (−0.99, −0.58) | <0.001 | −1.32 (−1.52, −1.12) | <0.001 | −0.85 (−1.06, −0.65) | <0.001 |
Model 1 adjusted for age, race, and BMI. Model 2 additionally adjusted for prevalent smoking, arthritis, cancer, diabetes ADA status, eGFR, antihypertensive medication use, systolic blood pressure, congestive heart failure, stroke, and coronary heart disease (myocardial infarction, angina, coronary artery bypass grafting, or angioplasty). A indicates atrial filling; ADA, American Diabetes Association; BMI, body mass index; CHS, Cardiovascular Health Study; CI, confidence interval; E, early filling; eGFR, estimated glomerular filtration rate; IMT, carotid intima‐media thickness; LA, left atrium; LVEF, left ventricular ejection fraction; LV RWT, left ventricular relative wall thickness; YAL, years of able life; YOL, years of life.
Each SD (0.34 mm) higher carotid IMT was associated with 0.5 and 0.79 fewer observed YAL in females and males, respectively, in the fully adjusted model (P<0.001). Higher LA dimension (for males only), higher peak A velocities (for females only), E/A ratio outside of the range 0.7 to 1.5, and higher LV mass were inversely related to YAL and YOL, but not YAL:YOL percentage. Results for the pooled cohort of men and women are in Data S1 (Tables S3 and S4). Sensitivity analysis of time to first ADL difficulty adjusting for incident CHF, MI, and stroke, in addition to the aforementioned confounders, showed persistence of the association between the variables and incident disability (Table S5).
Biomarkers
Higher levels of hsCRP (for females only), fibrinogen (for males only), NT‐proBNP, hsTNT, and PIIINP were inversely and strongly associated with observed YAL, YOL, and YAL:YOL percentage (Tables 5, 6, and S2). A 2‐fold increase in hsTNT in females and males was associated with 1.08 and 0.73 fewer YAL, 1.05 and 0.82 fewer YOL (P<0.001), and 3.5% and 1.4% fewer YAL:YOL (P<0.02), respectively.
Table 5.
Linear Regression Results of Adjusted Biomarkers Risk Factors for YAL and YOL for Female Participants in CHS (n=2769)
| Biomarkers | Years of Able Life | Years of Life | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||
| Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | |
| hsCRP (per 2‐fold increase) | −0.48 (−0.61, −0.35) | <0.001 | −0.29 (−0.42, −0.16) | <0.001 | −0.43 (−0.55, −0.31) | <0.001 | −0.25 (−0.37, −0.14) | <0.001 |
| Fibrinogen (per SD=65.80) | −0.27 (−0.46, −0.08) | 0.006 | −0.12 (−0.3, 0.06) | 0.196 | −0.32 (−0.49, −0.15) | <0.001 | −0.15 (−0.32, 0.01) | 0.074 |
| LDL (per SD=36.41) | 0.18 (0.01, 0.36) | 0.042 | 0.17 (0, 0.34) | 0.05 | 0.07 (−0.09, 0.23) | 0.41 | 0.09 (−0.06, 0.25) | 0.245 |
| NT‐proBNP (per 2‐fold increase) | −0.65 (−0.78, −0.51) | <0.001 | −0.5 (−0.64, −0.37) | <0.001 | −0.63 (−0.75, −0.5) | <0.001 | −0.51 (−0.63, −0.38) | <0.001 |
| hsTNT (per 2‐fold increase) | −1.45 (−1.69, −1.2) | <0.001 | −1.08 (−1.34, −0.83) | <0.001 | −1.38 (−1.61, −1.16) | <0.001 | −1.05 (−1.29, −0.82) | <0.001 |
| PIIINP (per SD=1.79) | −0.4 (−0.58, −0.24) | <0.001 | −0.26 (−0.42, −0.09) | 0.003 | −0.32 (−0.47, −0.18) | <0.001 | −0.21 (−0.35, −0.07) | 0.003 |
Model 1 adjusted for age, race, BMI, and BMI‐squared. Model 2 additionally adjusted for prevalent smoking, arthritis, cancer, diabetes ADA status, eGFR, antihypertensive medication use, systolic blood pressure, congestive heart failure, stroke, and coronary heart disease (myocardial infarction, angina, coronary artery bypass grafting, or angioplasty). ADA indicates American Diabetes Association; BMI, body mass index; CHS, Cardiovascular Health Study; CI, confidence interval; eGFR, estimated glomerular filtration rate; hsCRP, high‐sensitivity C‐reactive protein; hsTNT, high‐sensitivity troponin‐T; LDL, low‐density lipoprotein; NT‐proBNP, N‐terminal probrain natriuretic peptide; PIIINP, procollagen III N‐terminal propeptide; YAL, years of able life; YOL, years of life.
Table 6.
Linear Regression Results of Adjusted Biomarkers Risk Factors for YAL and YOL for Male Participants in CHS (n=2133)
| Biomarkers | Years of Able Life | Years of Life | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||
| Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | Coefficient (95% CI) | P Value | |
| hsCRP (per 2‐fold increase) | −0.66 (−0.8, −0.51) | <0.001 | −0.36 (−0.5, −0.22) | <0.001 | −0.69 (−0.83, −0.54) | <0.001 | −0.39 (−0.53, −0.25) | <0.001 |
| Fibrinogen (per SD=65.80) | −0.67 (−0.88, −0.46) | <0.001 | −0.39 (−0.59, −0.19) | <0.001 | −0.65 (−0.86, −0.44) | <0.001 | −0.37 (−0.56, −0.17) | <0.001 |
| LDL (per SD=36.41) | 0.41 (0.17, 0.64) | 0.001 | 0.23 (0.01, 0.44) | 0.042 | 0.31 (0.08, 0.54) | 0.009 | 0.13 (−0.09, 0.35) | 0.237 |
| NT‐proBNP (per 2‐fold increase) | −1.01 (−1.14, −0.87) | <0.001 | −0.79 (−0.94, −0.65) | <0.001 | −1.05 (−1.19, −0.92) | <0.001 | −0.79 (−0.94, −0.65) | <0.001 |
| hsTNT (per 2‐fold increase) | −1.18 (−1.42, −0.94) | <0.001 | −0.73 (−0.97, −0.5) | <0.001 | −1.31 (−1.54, −1.07) | <0.001 | −0.82 (−1.06, −0.58) | <0.001 |
| PIIINP (per SD=1.79) | −0.33 (−0.52, −0.14) | 0.001 | −0.23 (−0.41, −0.05) | 0.007 | −0.31 (−0.48, −0.13) | <0.001 | −0.20 (−0.36, −0.04) | 0.015 |
Model 1 adjusted for age, race, BMI, and BMI‐squared. Model 2 additionally adjusted for prevalent smoking, arthritis, cancer, diabetes ADA status, eGFR, antihypertensive medication use, systolic blood pressure, congestive heart failure, stroke, and coronary heart disease (myocardial infarction, angina, coronary artery bypass grafting, or angioplasty). ADA indicates American Diabetes Association; BMI, body mass index; CHS, Cardiovascular Health Study; CI, confidence interval; eGFR, estimated glomerular filtration rate; hsCRP, high‐sensitivity C‐reactive protein; hsTNT, high‐sensitivity troponin‐T; LDL, low‐density lipoprotein; NT‐proBNP, N‐terminal probrain natriuretic peptide; PIIINP, procollagen III N‐terminal propeptide; YAL, years of able life; YOL, years of life.
Discussion
Men and women above the age of 65 years who had a favorable CV profile determined by echocardiography, carotid IMT, or biomarkers of inflammation, atherosclerosis, myocardial injury and stress, and cardiac extracellular collagen turnover spent more years, and a higher percentage of the end of their lives, without difficulty in ADLs. By definition, YAL integrates the number of years alive with the number of years they spend without any ADL difficulty, a prime goal for elderly persons. Furthermore, in a sensitivity analysis adjusting for incident CHF, MI, and stroke, the results remained statistically significant, concluding that these variables are strongly associated with YAL irrespective of incident CVD.
As the number of comorbidities increases, prevalence of disability (defined as any ADL difficulty) increases.10 Having a higher number of risk factors at middle age (smoking, HTN, obesity, hyperlipidemia, and minor electrocardiogram [EKG] abnormalities) has been associated with a shorter time to disability.6,11 Furthermore, subclinical disease has been associated with the quality of years alive beyond the age of 65. Asymptomatic CHS participants with subclinical vascular disease defined as any common or internal IMT above the 80th percentile, maximum stenosis of the internal carotid artery >25%, ankle‐arm index ≤0.9, major EKG abnormality, or Rose questionnaire positive for angina or claudication were found to be less likely to be free of incident CVD, cancer, chronic obstructive pulmonary disease, or new and persistent physical disability or cognitive decline.12
With the shift toward personalized and patient‐centered care, patient preferences are playing a growing role in clinical decision making and risk assessment. In a survey of 357 older adults living in senior centers and an assisted living facility, with the main outcome being a person's prioritization of 4 health outcomes: “keeping you alive, maintaining independence, reducing or eliminating pain, and reducing or eliminating other symptoms (eg, dizziness, fatigue, shortness of breath)”; 76% ranked maintaining independence as the most important health outcome; notably, staying alive was the least important.4 Likewise, this pattern of preference was demonstrated in seriously ill patients above the age of 60.13 Accordingly, we analyzed these variables in a large sample of community dwellers and followed them for up to 18 years.
Disability has many causes. The variables chosen in the analysis have been shown to be associated with development of morbidity (that could lead to disability) or mortality. Our study incorporated CV structural and functional assessment and measurement of biomarkers of various systems. Furthermore, we focused our outcome into a fundamental and a global assessment of basic physical function, which, without any of its components, a person is markedly less likely to be able to maintain physical independence.
Our finding that most echocardiographic parameters in the fully adjusted model were associated with the YAL, but were no longer significant when assessing the YAL:YOL percentage, suggests that these variables might be associated with longevity to a greater extent than physical ability.14 In other words, death occurs relatively rapidly for subjects with unfavorable measures. LA volume has been correlated with exercise capacity.15 LV mass is known to predict incident CHF, stroke, and CVD.16–17 Carotid IMT has been extensively studied as a risk prediction tool and found to predict future stroke and MI, but generally adds modest benefit when combined with the traditional risk scores (such as the Framingham Risk Score).18–19
Measures of inflammation and coagulation in relation to physical function have been assessed in several observational cohorts. hsCRP has been linked to total and CV mortality (CVM), although modestly, and has been associated with physical performance in older adults.20–21 Fibrinogen, among other coagulation biomarkers, has been implicated in the development of disability.22 The relationship between total cholesterol and functional ability in older adults is controversial. Some studies have suggested a negative and others a positive, relationship.23–25 LDL, however, has not been evaluated in prospective cohorts. Our finding that LDL is negatively associated with YAL, but not YOL or YAL:YOL percentage—irrespective of statin use—is difficult to explain. Low LDL could be a marker of “frailty” or could be owing to other unmeasured comorbidities or genetic factors.
NT‐proBNP predicts total and CVM, MI, stroke, and CHF.26–28 Whereas physical activity has been shown to decrease the likelihood of an elevation in NT‐proBNP and subsequent development of clinical CHF,29 it is demonstrated that subclinical elevation in NT‐proBNP is a marker for development of functional decline and mortality. The cardiac‐specific biomarker, troponin, measured by a high‐sensitivity assay, is a marker of chronic myocardial injury and a predictor for future risk of CHF and CV death in community‐dwelling older adults.30 Our findings extend the value of hsTNT beyond the traditional outcomes. hsTNT could be a marker of overall muscular‐functional decline and warrants further research. PIIINP, a marker of collagen turnover, has been linked to the development of death and heart failure.31–32 To our knowledge, we demonstrate, for the first time, that elevation of this biomarker is correlated with lower disability‐free survival in community dwellers. This might be part of a phenotype of systemic collagenous turnover that predates functional decline before death.
Some of these variables might be associated with future development of comorbidities, which, in turn, accelerate functional decline. However, the relationship between these variables and YAL remained significant even after adjusting for incident CV outcomes, indicating that these variables are associated with maintenance of physical ability, irrespective of development of CVD. In fact, some have argued that, despite developing comorbidities, some centenarians are able to achieve exceptional age and avoid disability.5 The observed associations could be modified by other unmeasured variables. For example, participants with abnormal LVEF could develop other morbidities, which, in turn, lead to disability, before developing clinical CVD. Further research is needed to explore the role of these biomarkers and CV structural variables in “channeling” persons into one of the pathways of aging.
Our study has several strengths. We examined a large sample size from a relevant cohort of older community dwellers. The follow‐up time was long and the outcomes highly relevant for older people. Our study also has several limitations. First, LV mass and LV RWT and the biomarkers were not performed on the entire cohort and, in the case of PIIINP, was performed later in the study, thus limiting the follow‐up time to 11 years. Differential absence of these measures could theoretically have introduced bias. However, only 550 subjects did not have these echo measures at baseline. Second, there could be residual confounding that we could not account for in our models. Third, although there was no significant interaction in statin use for the LDL variable, our power to detect a difference is limited, given that only 2.1% of the cohort used statins at the baseline because their use in clinical practice was not robust at the time. Fourth, upon interpretation of the P values, multiple comparisons should be taken into account. Nevertheless, with 30 comparisons for the primary outcome at the P=0.05 level of significance, we would expect 1.5 to be significant owing to chance alone. Fifth, in the sensitivity analysis, whereas Cox regression is focusing on first occurrence and YAL encompasses all occurrences, because both are getting at a measure of disability, we would expect similarities in risk factors.
Conclusion
Favorable echocardiographic measures, carotid intima thickness, and biomarkers of inflammation, coagulation, atherosclerosis, myocardial injury and stress, and extracellular collagen turnover measured in persons above the age of 65 were associated with the number of years of able life and independence, irrespective of development of CVD, in a large national cohort followed for up to 18 years. Development of predictive models and the utility of targeting these variables in clinical interventions with the goal to improve the quality of life of older persons above and beyond mitigation of disease remain to be further evaluated.
Supplementary Material
Appendix Supplementary Methods.
Sources of Funding
This research was supported by contracts HHSN268201200036C, HHSN268200800007C, N01 HC55222, N01HC85079, N01HC85080, N01HC85081, N01HC85082, N01HC85083, N01HC85086, and grant HL080295 from the National Heart, Lung, and Blood Institute (NHLBI), with an additional contribution from the National Institute of Neurological Disorders and Stroke. Additional support was provided by AG023629 from the National Institute on Aging. A full list of principal CHS investigators and institutions can be found at CHS‐NHLBI.org.
Disclosures
Dr Gardin received honoraria on the Speakers’ Bureau from Gilead Sciences. All other authors have nothing to disclose.
References
- Layte R, Sexton E, Savva G. Quality of life in older age: evidence from an Irish cohort study. J Am Geriatr Soc. 2013; 61:S299-S305. [DOI] [PubMed] [Google Scholar]
- Bryant LL, Corbett KK, Kutner JS. In their own words: a model of healthy aging. Soc Sci Med. 2001; 53:927-941. [DOI] [PubMed] [Google Scholar]
- Population Division USCB. Projections of the population by age and sex for the United States: 2010 to 2050 (np2008‐t12). 2008. Available at: http://www.Aoa.Gov/aoaroot/aging_statistics/future_growth/future_growth.Aspx#age. Accessed December 2014.
- Fried TR, Tinetti ME, Iannone L, O'Leary JR, Towle V, Van Ness PH. Health outcome prioritization as a tool for decision making among older persons with multiple chronic conditions. Arch Intern Med. 2011; 171:1856-1858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terry DF, Sebastiani P, Andersen SL, Perls TT. Disentangling the roles of disability and morbidity in survival to exceptional old age. Arch Intern Med. 2008; 168:277-283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vita AJ, Terry RB, Hubert HB, Fries JF. Aging, health risks, and cumulative disability. N Engl J Med. 1998; 338:1035-1041. [DOI] [PubMed] [Google Scholar]
- Fried LP, Borhani NO, Enright P, Furberg CD, Gardin JM, Kronmal RA, Kuller LH, Manolio TA, Mittelmark MB, Newman A, O'Leary DH, Psaty B, Rautaharju P, Tracy RP, Weiler PG. The Cardiovascular Health Study: design and rationale. Ann Epidemiol. 1991; 1:263-276. [DOI] [PubMed] [Google Scholar]
- Gardin JM, Wong ND, Bommer W, Klopfenstein HS, Smith VE, Tabatznik B, Siscovick D, Lobodzinski S, Anton‐Culver H, Manolio TA. Echocardiographic design of a multicenter investigation of free‐living elderly subjects: the Cardiovascular Health Study. J Am Soc Echocardiogr. 1992; 5:63-72. [DOI] [PubMed] [Google Scholar]
- O'Leary DH, Polak JF, Wolfson SK, Bond MG, Bommer W, Sheth S, Psaty BM, Sharrett AR, Manolio TA. Use of sonography to evaluate carotid atherosclerosis in the elderly. The Cardiovascular Health Study. CHS Collaborative Research Group. Stroke. 1991; 22:1155-1163. [DOI] [PubMed] [Google Scholar]
- Lunney JR, Lynn J, Foley DJ, Lipson S, Guralnik JM. Patterns of functional decline at the end of life. JAMA. 2003; 289:2387-2392. [DOI] [PubMed] [Google Scholar]
- Daviglus ML, Liu K, Pirzada A, Yan LL, Garside DB, Feinglass J, Guralnik JM, Greenland P, Stamler J. Favorable cardiovascular risk profile in middle age and health‐related quality of life in older age. Arch Intern Med. 2003; 163:2460-2468. [DOI] [PubMed] [Google Scholar]
- Newman AB, Arnold AM, Naydeck BL, Fried LP, Burke GL, Enright P, Gottdiener J, Hirsch C, O'Leary D, Tracy R. “Successful aging”: effect of subclinical cardiovascular disease. Arch Intern Med. 2003; 163:2315-2322. [DOI] [PubMed] [Google Scholar]
- Fried TR, Bradley EH, Towle VR, Allore H. Understanding the treatment preferences of seriously ill patients. N Engl J Med. 2002; 346:1061-1066. [DOI] [PubMed] [Google Scholar]
- Gardin JM, McClelland R, Kitzman D, Lima JA, Bommer W, Klopfenstein HS, Wong ND, Smith VE, Gottdiener J. M‐mode echocardiographic predictors of six‐ to seven‐year incidence of coronary heart disease, stroke, congestive heart failure, and mortality in an elderly cohort (the Cardiovascular Health Study). Am J Cardiol. 2001; 87:1051-1057. [DOI] [PubMed] [Google Scholar]
- Kusunose K, Motoki H, Popovic ZB, Thomas JD, Klein AL, Marwick TH. Independent association of left atrial function with exercise capacity in patients with preserved ejection fraction. Heart. 2012; 98:1311-1317. [DOI] [PubMed] [Google Scholar]
- Bikkina M, Levy D, Evans JC, Larson MG, Benjamin EJ, Wolf PA, Castelli WP. Left ventricular mass and risk of stroke in an elderly cohort. JAMA. 1994; 272:33-36. [PubMed] [Google Scholar]
- de Simone G, Gottdiener JS, Chinali M, Maurer MS. Left ventricular mass predicts heart failure not related to previous myocardial infarction: the Cardiovascular Health Study. Eur Heart J. 2008; 29:741-747. [DOI] [PubMed] [Google Scholar]
- Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima‐media thickness: a systematic review and meta‐analysis. Circulation. 2007; 115:459-467. [DOI] [PubMed] [Google Scholar]
- Simon A, Megnien J‐L, Chironi G. The value of carotid intima‐media thickness for predicting cardiovascular risk. Arterioscler Thromb Vasc Biol. 2010; 30:182-185. [DOI] [PubMed] [Google Scholar]
- Oluleye OW, Folsom AR, Nambi V, Lutsey PL, Ballantyne CM. Troponin T, B‐type natriuretic peptide, C‐reactive protein, and cause‐specific mortality. Ann Epidemiol. 2013; 23:66-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jenny NS, French B, Arnold AM, Strotmeyer ES, Cushman M, Chaves PH, Ding J, Fried LP, Kritchevsky SB, Rifkin DE, Sarnak MJ, Newman AB. Long‐term assessment of inflammation and healthy aging in late life: the Cardiovascular Health Study All Stars. J Gerontol A Biol Sci Med Sci. 2012; 67:970-976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McClure CK, El Khoudary SR, Karvonen‐Gutierrez CA, Ylitalo KR, Tomey K, Vopham T, Sternfeld B, Cauley JA, Harlow S. Prospective associations between inflammatory and hemostatic markers and physical functioning limitations in mid‐life women: longitudinal results of the Study of Women's health Across the Nation (SWAN). Exp Gerontol. 2014; 49:19-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strandberg TE, Strandberg A, Rantanen K, Salomaa VV, Pitkala K, Miettinen TA. Low cholesterol, mortality, and quality of life in old age during a 39‐year follow‐up. J Am Coll Cardiol. 2004; 44:1002-1008. [DOI] [PubMed] [Google Scholar]
- Okamura T, Hayakawa T, Hozawa A, Kadowaki T, Murakami Y, Kita Y, Abbott RD, Okayama A, Ueshima H. Lower levels of serum albumin and total cholesterol associated with decline in activities of daily living and excess mortality in a 12‐year cohort study of elderly Japanese. J Am Geriatr Soc. 2008; 56:529-535. [DOI] [PubMed] [Google Scholar]
- Schalk BW, Visser M, Deeg DJ, Bouter LM. Lower levels of serum albumin and total cholesterol and future decline in functional performance in older persons: the Longitudinal Aging Study Amsterdam. Age Ageing. 2004; 33:266-272. [DOI] [PubMed] [Google Scholar]
- Di Angelantonio E, Chowdhury R, Sarwar N, Ray KK, Gobin R, Saleheen D, Thompson A, Gudnason V, Sattar N, Danesh J. B‐type natriuretic peptides and cardiovascular risk: systematic review and meta‐analysis of 40 prospective studies. Circulation. 2009; 120:2177-2187. [DOI] [PubMed] [Google Scholar]
- Kistorp C, Raymond I, Pedersen F, Gustafsson F, Faber J, Hildebrandt P. N‐terminal pro‐brain natriuretic peptide, C‐reactive protein, and urinary albumin levels as predictors of mortality and cardiovascular events in older adults. JAMA. 2005; 293:1609-1616. [DOI] [PubMed] [Google Scholar]
- Wallen T, Landahl S, Hedner T, Nakao K, Saito Y. Brain natriuretic peptide predicts mortality in the elderly. Heart. 1997; 77:264-267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klenk J, Denkinger M, Nikolaus T, Peter R, Rothenbacher D, Koenig WActi FESG. Association of objectively measured physical activity with established and novel cardiovascular biomarkers in elderly subjects: every step counts. J Epidemiol Community Health. 2013; 67:194-197. [DOI] [PubMed] [Google Scholar]
- deFilippi CR, de Lemos JA, Christenson RH, Gottdiener JS, Kop WJ, Zhan M, Seliger SL. Association of serial measures of cardiac troponin T using a sensitive assay with incident heart failure and cardiovascular mortality in older adults. JAMA. 2010; 304:2494-2502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barasch E, Gottdiener JS, Aurigemma G, Kitzman DW, Han J, Kop WJ, Tracy RP. The relationship between serum markers of collagen turnover and cardiovascular outcome in the elderly: the Cardiovascular Health Study. Circ Heart Fail. 2011; 4:733-739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Velagaleti RS, Gona P, Sundstrom J, Larson MG, Siwik D, Colucci WS, Benjamin EJ, Vasan RS. Relations of biomarkers of extracellular matrix remodeling to incident cardiovascular events and mortality. Arterioscler Thromb Vasc Biol. 2010; 30:2283-2288. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix Supplementary Methods.