

Abstract
Noncompaction ventricular myocardium is an unusual cause of cardiomyopathy. It is association with congenital heart defects, most often with outflow obstructive lesions or coronary anomalies. However, no factor could explain the arrest of development of myocardial structure (isolated form). The pathogenesis of isolated noncompaction is thought to be an arrest in endomyocardial morphogenesis. It has been reported that myocardial noncompaction could present as acquired disease. The most common site of involvement is the left ventricle, with right ventricular involvement being reported in a few cases. In this report, we present a case with noncompaction of the right ventricle (RV). Cardiac computed tomography angiography and magnetic resonance imaging demonstrated morphological abnormalities of the RV.
Keywords: Multidetector computed tomography, Magnetic resonance imaging, Isolated noncompaction of the ventricular myocardium
Introduction
Noncompaction of ventricular myocardium (NVM) is considered as an unusual cause of cardiomyopathy. Dense trabecular meshwork and deep intertrabecular recesses are seen on the ventricle wall.1) Etiology of NVM is thought to be due to arrest of myocardial morphogenesis.2) The prevalence of left ventricular noncompaction is about 0.01% in adults and 0.14% in pediatric patients.3),4) The most common site of involvement is the left ventricle (LV), with right ventricular involvement being reported in a few cases.5),6) In this report, we present a case with noncompaction of the right ventricle (RV). Magnetic resonance imaging (MRI) and cardiac computed tomography angiography (CCTA) demonstrated morphological and functional abnormalities of the RV.
Case
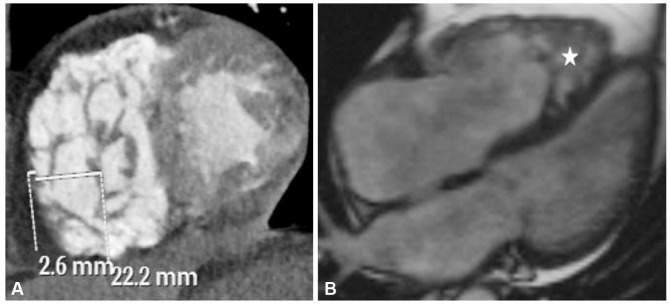
A 72-year-old male presented mild chest discomfort and palpitation sense with effort. In his medical history, he had hypertension, hyperlipidemia, and diabetes mellitus. He had 3 stents placed at the coronary arteries. He had no relevant history of familial heart disease or history of smoking. On admission, his blood pressure was 157/85 mm Hg with pulse rate at 84 beats/min. Physical examination revealed no abnormality. Transthoracic echocardiogram reveal-ed a hypertrabeculated and spongiform appearance of the right ventricular apical segment. A color doppler echocardiographic examination revealed the presence of blood flow in the deep intertrabecular recesses. On four chamber view, end-diastolic basal diameter of the RV was measured at 4 cm (normal <4.2 cm). RV systolic function was observed as normal with tricuspid annular plane systolic excursion of 2 cm and myocardial performance index of 0.35. CCTA revealed two stents located at the proximal segment of the left anterior descending artery and one stent located at mid-segment of the circumflex artery. Mild intimal hyperplasia was reported at the intimal surface of the stents. Additionally, a prominent trabecular meshwork and deep intertrabecular recesses were observed at the apex of the RV. Noncompacted thickness (NC) of the RV in diastole was 22.2 mm at the apical level with compacted thickness (C) of 2.6 mm (NC/C ratio 8.5) (Fig. 1A). Cardiac MRI was performed for functional assessment. Wall hypokinesis was observed at the mid and distal anterior wall segments of the LV. No visible wall hypokinesis was observed at the RV. Noncompacted wall segments of the RV were well depicted on four-chamber static image of the cine-MRI (Fig. 1B).
Fig. 1. A 72-year old male with noncompaction of right ventricle. A: short axis view of the ventricles on computed tomography imaging showing deep intertrabecular recesses within the right ventricle with a noncompacted to compacted myocardium ratio of 8.5. B: true fast imaging with steady-state precession (true-FISP) cine four-chamber magnetic resonance image delineating noncompaction in the apical region of the right ventricle (star).
Discussion
Noncompaction of ventricular myocardium is an uncommon disorder with uncertain etiology. It is being reported with increasing frequency as a cause of ventricular failure in adults and children. It has been described in association with congenital heart defects, most often with outflow obstructive lesions or coronary anomalies. However, no factor could explain the arrest of the development of the myocardial structure (isolated form).7) Isolated ventricular non-compaction (IVNC) is considered as unclassified cardiomyopathy.1) The pathogenesis of IVNC is thought to be an arrest in endomyocardial morphogenesis. Approximately between fetal week 5 to week 8, intertrabecular spaces are compressed, resulting in compaction from the base towards the apex and from epicardium to endocardium. An arrest in this process results in noncompaction. It has been reported that myocardial noncompaction could present as acquired disease.8) Since the coronary arterial circulation is normal in IVNC, extramural myocardial blood supply is not likely the cause.9) The cause and pathogenesis of acquired disease still remains unknown, but a few hypothesis have been proposed to explain the etiopathogenesis 10): 1) Noncompaction results from an insufficient attempt of hypertrophy of the ventricular myocardium; 2) Noncompaction results from an attempt to enlarge the endocardial surface to move large volumes with less contractility in volume overload; 3) Noncompaction results from multiple dissections of the myocardium caused by decreased adhesion of cardiac cells.10) We considered the case as an isolated form. The usual location of involvement is the LV. However, participation of both ventricles and rarely isolated involvement of the RV can be seen. Noncompaction was reported to affect exclusively LV in a series of 34 adults.3) RV noncompaction has been depicted only in a few cases of newborns with congenital heart defects and in adult patients.11),12)
MRI has been proposed to be an important diagnostic tool in NVM. The ratio of noncompacted to compacted myocardium (NC/C ratio) has been reported as a diagnostic criterion. A diastolic NC/C ratio >2.3 was reported to have high diagnostic accuracy for distinguishing pathological left ventricular noncompaction from other degrees of trabeculation observed in healthy, dilated, and hypertrophied hearts.13) However, no specific criterion has been proposed for the diagnosis of noncompaction of RV. This is likely due to its small number of cases and less performed CCTA and MRI for diagnosis in the past. In our case, noncompacted to compacted myocardium (NC/C ratio) ratio was 8.5. Arrhythmias, heart failure, and thromboembolic events may be seen as morbidity during long-term follow-up. Heart failure is caused by systolic and diastolic dysfunction.3)
In summary, CCTA and MRI are ex-cellent diagnostic tools for NVM, especially in noncompaction of RV.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Richardson P, McKenna W, Bristow M, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation. 1996;93:841–842. doi: 10.1161/01.cir.93.5.841. [DOI] [PubMed] [Google Scholar]
- 2.Taylor GP. Developmental Pathology of the Embryo and Fetus. In: Dimmick JE, Kalousek DK, editors. Cardiovascular system. Philadelphia, PA: Lippincott; 1992. pp. 467–508. [Google Scholar]
- 3.Oechslin EN, Attenhofer Jost CH, Rojas JR, Kaufmann PA, Jenni R. Long-term follow-up of 34 adults with isolated left ventricular noncompaction: a distinct cardiomyopathy with poor prognosis. J Am Coll Cardiol. 2000;36:493–500. doi: 10.1016/s0735-1097(00)00755-5. [DOI] [PubMed] [Google Scholar]
- 4.Pignatelli RH, McMahon CJ, Dreyer WJ, et al. Clinical characterization of left ventricular noncompaction in children: a relatively common form of cardiomyopathy. Circulation. 2003;108:2672–2678. doi: 10.1161/01.CIR.0000100664.10777.B8. [DOI] [PubMed] [Google Scholar]
- 5.Alehan D, Dogan OF. Right ventricular noncompaction in a neonate with complex congenital heart disease. Cardiol Young. 2005;15:434–436. doi: 10.1017/S1047951105000910. [DOI] [PubMed] [Google Scholar]
- 6.Hruda J, Sobotka-Plojhar MA, Fetter WP. Transient postnatal heart failure caused by noncompaction of the right ventricular myocardium. Pediatr Cardiol. 2005;26:452–454. doi: 10.1007/s00246-004-0752-z. [DOI] [PubMed] [Google Scholar]
- 7.Ritter M, Oechslin E, Sütsch G, Attenhofer C, Schneider J, Jenni R. Isolated noncompaction of the myocardium in adults. Mayo Clin Proc. 1997;72:26–31. doi: 10.4065/72.1.26. [DOI] [PubMed] [Google Scholar]
- 8.Stöllberger C, Winkler-Dworak M, Blazek G, Finsterer J. Age-dependency of cardiac and neuromuscular findings in left ventricular noncompaction. Int J Cardiol. 2006;111:131–135. doi: 10.1016/j.ijcard.2005.08.009. [DOI] [PubMed] [Google Scholar]
- 9.Chin TK, Perloff JK, Williams RG, Jue K, Mohrmann R. Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation. 1990;82:507–513. doi: 10.1161/01.cir.82.2.507. [DOI] [PubMed] [Google Scholar]
- 10.Song ZZ, Ma J. A rare combination of left ventricular noncompaction and a right coronary artery-to-right ventricle fistula: echocardiographic features. J Ultrasound Med. 2007;26:547–550. doi: 10.7863/jum.2007.26.4.547. [DOI] [PubMed] [Google Scholar]
- 11.Sert A, Aypar E, Aslan E, Odabas D. Isolated right ventricular noncompaction in a newborn. Pediatr Cardiol. 2013;34:1896–1898. doi: 10.1007/s00246-012-0435-0. [DOI] [PubMed] [Google Scholar]
- 12.Acar G, Alizade E, Yazıcıoğlu MV, Bayram Z. A rare unclassified cardiomyopathy: isolated right ventricle noncompaction. Turk Kardiyol Dern Ars. 2013;41:267. doi: 10.5543/tkda.2013.27095. [DOI] [PubMed] [Google Scholar]
- 13.Petersen SE, Selvanayagam JB, Wiesmann F, et al. Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging. J Am Coll Cardiol. 2005;46:101–105. doi: 10.1016/j.jacc.2005.03.045. [DOI] [PubMed] [Google Scholar]