

Abstract
Background:
Previous publications reported that an individual's month of birth (MOB) might have an important correlation to that consequent risk of multiple sclerosis (MS).
Aim:
The aim of this preliminary study was to investigate the distribution of different MOBs inpatients with MS in Isfahan, Iran.
Materials and Methods:
This investigation was conducted to the Isfahan Neurosciences Research Centre. 1283 patients with MS were studied. Clinical data were recorded in d-Base and analyzed using SPSS (version 18) for Windows.
Results:
Of the total population studied there were 979 females and 304 males. The mean age of all the patients was 34.6 years (range 10-87 years). Within the total population, the MOBs in the 62% of patients were in the season's spring and summer, and in 38% of patients they were in the season's autumn and winter. As the MOB might be recognized to have a bearing on an individual's risk of contracting MS, the highest and lowest correlations seem to be linked with April, September, May (↑), and November (↓), respectively.
Conclusions:
The seasonal relationship between MOBs and MS risk might be pointed toward a potential function for vitamin D throughout pregnancy or the early life of the newborn. Further studies are needed to confirm these correlations.
Keywords: Iranian population, month of birth, multiple sclerosis, spring
INTRODUCTION
Multiple sclerosis (MS) is a recurrent tentative disease of the central nervous system (CNS) that typically follows a deteriorating course, with accumulation of plaques associated with the demyelination of axons and the loss of oligodendrocytes. It is hypothesized that the loss of axons is the main mechanism underlying progressive disability. Escalating data suggest there are two main types of risk factors for MS, genetic and environmental, likely with complex interactions between them and effects that may be harmful or protective, depending on the patient.[1,2,3]
Month of birth (MOB) has formerly been expressed as a risk question for MS. Torkildsen et al., presented an update regarding the MOB as a risk factor for MS. The outcome appears to be mainly important in high-risk regions for the disease, particularly in districts with low sunlight exposure. No MOB effects or insignificant correlation in districts with high sunshine exposure have been reported.[4] Disanto et al., documented that the risk of different immune-mediated diseases in the UK might be considerably prejudiced by the season of birth, suggesting the effect of gestational ultraviolet B and vitamin D exposure.[5] The association of spring birth with the risk of MS has been confirmed by Saastamoinen et al.[6] Studies related to the association between MOB and MS incidence in Southern Iran recognized that the outcomes are comparable to those detailed by many earlier studies.[7] It has also been documented that in the nonexistence of sufficient control for confusing features such as year and place of birth, the previous report for the involvement of MS with MOB might possibly include false positives.[8] Regarding Latin America and Portugal, a recent study showed the nonexistence of a seasonality model relating the risk of MS to MOB.[9] Another study related the risk of MS in different latitudes of South America to MOB showed that MS patients born to mothers who were pregnant at different southern latitudes do not follow the seasonal pattern observed at higher northern latitudes.[10] The Isfahan MS Society (IMSS) reported a period prevalence of 73.3/100,000 between April 2003 and July 2010, and an incidence rate of 9.1/100,000 in the year 2009. A recent study confirmed a prevalence of 93.6for Isfahan, Iran.[11,12,13,14] The aim of this study was to investigate the distribution of MOB in patients with MS in Isfahan, Iran.
MATERIALS AND METHODS
A retrospective study was performed on 1283 patients with MS, those attended MS clinic located at the Isfahan Kashani Hospital. The study was conducted to the Isfahan Neurosciences Research Centre (INRC). Demographic and clinical data together with the date of birth including MOB, gender, and age were recorded in d-Base. The statistical analysis of the data was performed using SPSS (version 18) for Windows.
RESULTS
Figure 1 shows that 76% of the total population studied were females (n = 979) and 24% were males (n = 304). The mean age of all patients was 34.6 years (range10-87 years). Figure 2 shows that the age of 87% of patients ranged 20-49 years. Figure 3 shows the distribution of patients according to MOBs. The highest and lowest associations could be linked to April and November, respectively. The MOBs in 62% (n = 609) of patients were in spring-summer and in 38% (n = 370) were in autumn-winter.
Figure 1.
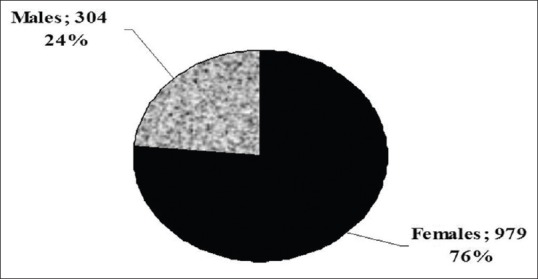
Fraction of gender in population studied (n=1283)
Figure 2.
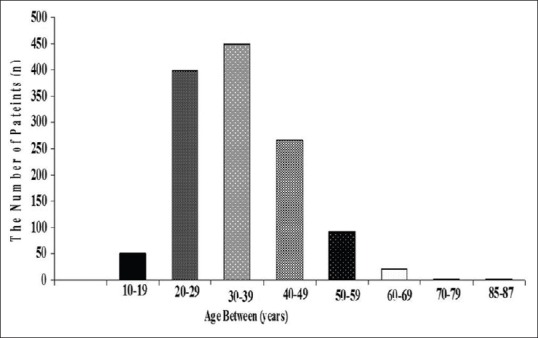
Distribution of age in population studied (n=1283)
Figure 3.
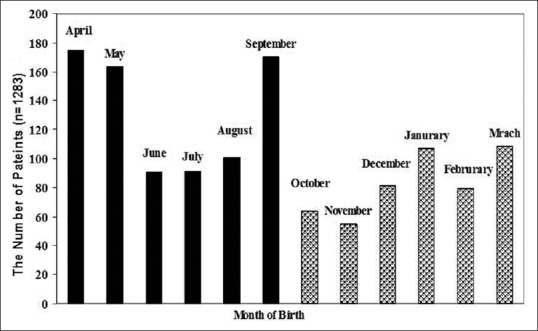
Distribution of patients according to month of birth
A further analysis related to gender showed that in the male population (n = 304), the MOBs in 59% were in spring-summer and in 41% (n = 124) were in autumn-winter [Figure 4].
Figure 4.
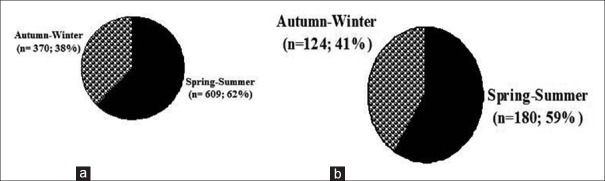
Distribution of (a) females and (b) males according to their month of birth
The mean age of male patients was 36.9 years (range 14-85 years). The mean age of females was 33.9 years (range 10-87 years). In the females the highest population of MS (62%) was linked to spring-summer as follows: September (n = 137), April (n = 127), and May (n = 125).
DISCUSSION
The result of this preliminary analysis of MOB in patients with MS in Isfahan, Iran is in agreement with previous publications,[7,15] as the MOB with the highest population of MS was ranked in spring months such as April and May. Previous publications reported that Isfahan could be considered as an area with a medium to high risk of MS.[3,11,12,13,14] Furthermore, the results of this survey also supported that the highest rate of patient population could be linked to the age group of 20-39 (67%), followed by 30-39 (36%), and 40-49 (22%) years. This is in agreement with earlier publications that reported an increasing incidence of MS within the younger population, which results in a major economic burden on the patient, their family, the health system, and society.[16,17,18,19]
In the present study, the MOBs in 62% of patients were in September, April, and May. Numerous investigations have pointed toward MOBs as an indicator of the risk feature for MS susceptibility and disease progression. Previous publication reported also a higher risk of MS for those born in April (ratio 1.07, P = 0.002) and May (ratio 1.11, P = 0.0006), and a lower risk for those born in October (ratio 0.94, P = 0.004) and November (ratio 0.88, P = 0.0002).[15] The seasonal association between MOB and the risk of MS might be explained by the relationship between geographic latitude and risk, as the effect appears to be most important in high-risk regions, particularly in regions with low ultraviolet light exposure and low maternal vitamin D levels. Exposure to sunlight during pregnancy or early childhood might be associated with the risk of MS, as low exposure could mean a lower amount of vitamin D.[20,21,22] Finally, in order to move further toward the prediction of: (1) Prevention aspects in the first important step (2) therapeutic and pharmacotherapy management in the second step additional advance studies, to analyze many features from maternity to maturity and the environmental geographies that are coupled with susceptibility to MS are recommended in Isfahan, Iran.
Footnotes
Source of Support: Nil
Conflict of Interest: The authors declare that there is no conflict of interest.
REFERENCES
- 1.Bradford CM, Ramos I, Cross AK, Haddock G, McQuaid S, Nicholas AP, et al. Localisation of citrullinated proteins in normal appearing white matter and lesions in the central nervous system in multiple sclerosis. J Neuroimmunol. 2014;273:85–95. doi: 10.1016/j.jneuroim.2014.05.007. [DOI] [PubMed] [Google Scholar]
- 2.Shaygannejad V, Tolou-Ghamari Z. What is the real fate of vitamin D in multiple sclerosis? Int J Prev Med. 2013;4(Suppl 2):S159–64. [PMC free article] [PubMed] [Google Scholar]
- 3.Tolou-Ghamari Z, Shaygannejad V, Ashtari F. Preliminary study related the incidence of methylprednisolone pulse therapy in patients visited multiple sclerosis clinic located at the Isfahan Kashani Hospital. Int J Prev Med. 2013;4(Suppl 2):S274–8. [PMC free article] [PubMed] [Google Scholar]
- 4.Torkildsen O, Grytten N, Aarseth J, Myhr KM, Kampman MT. Month of birth as a risk factor for multiple sclerosis: An update. Acta Neurol Scand Suppl. 2012:58–62. doi: 10.1111/ane.12040. [DOI] [PubMed] [Google Scholar]
- 5.Disanto G, Chaplin G, Morahan JM, Giovannoni G, Hyppönen E, Ebers GC, et al. Month of birth, vitamin D and risk of immune-mediated disease: A case control study. BMC Med. 2012;10:69. doi: 10.1186/1741-7015-10-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Saastamoinen KP, Auvinen MK, Tienari PJ. Month of birth is associated with multiple sclerosis but not with HLA-DR15 in Finland. Mult Scler. 2012;18:563–8. doi: 10.1177/1352458511426814. [DOI] [PubMed] [Google Scholar]
- 7.Nikseresht A, Sharifian M, Hamidian Jahromi A. Month of birth and the incidence of multiple sclerosis in southern Iran. Iran J Med Sci. 2014;39(Suppl):232–3. [PMC free article] [PubMed] [Google Scholar]
- 8.Fiddes B, Wason J, Kemppinen A, Ban M, Compston A, Sawcer S. Confounding underlies the apparent month of birth effect in multiple sclerosis. Ann Neurol. 2013;73:714–20. doi: 10.1002/ana.23925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sá MJ. Month of birth is not a definite risk factor for multiple sclerosis. Arq Neuropsiquiatr. 2014:72–397. doi: 10.1590/0004-282x20140029. [DOI] [PubMed] [Google Scholar]
- 10.Fragoso YD, Adoni T, Almeida SM, Alves-Leon SV, Arruda WO, Barbagelata-Aguero F, et al. Multiple sclerosis in South America: Month of birth in different latitudes does not seem to interfere with the prevalence or progression of the disease. Arq Neuropsiquiatr. 2013;71:573–9. doi: 10.1590/0004-282X20130098. [DOI] [PubMed] [Google Scholar]
- 11.Etemadifar M, Sajjadi S, Nasr Z, Firoozeei TS, Abtahi SH, Akbari M, et al. Epidemiology of multiple sclerosis in Iran: A systematic review. Eur Neurol. 2013;70:356–63. doi: 10.1159/000355140. [DOI] [PubMed] [Google Scholar]
- 12.Etemadifar M, Abtahi SH. Multiple sclerosis in Isfahan, Iran: Past, Present and Future. Int J Prev Med. 2012;3:301–2. [PMC free article] [PubMed] [Google Scholar]
- 13.Etemadifar M, Janghorbani M, Shaygannejad V, Ashtari F. Prevalence of multiple sclerosis in Isfahan, Iran. Neuroepidemiology. 2006;27:39–44. doi: 10.1159/000094235. [DOI] [PubMed] [Google Scholar]
- 14.Etemadifar M, Maghzi AH. Sharp increase in the incidence and prevalence of multiple sclerosis Isfahan, Iran. Mult Scler. 2011;17:1022–7. doi: 10.1177/1352458511401460. [DOI] [PubMed] [Google Scholar]
- 15.Dobson R, Giovannoni G, Ramagopalan S. The month of birth effect in multiple sclerosis: Systematic review, meta-analysis and effect of latitude. J Neurol Neurosurg Psychiatry. 2013;84:427–32. doi: 10.1136/jnnp-2012-303934. [DOI] [PubMed] [Google Scholar]
- 16.Kezuka T. Optic neuritis- Immunological approach to elucidate pathogenesis and develop innovative therapy. Nihon Ganka Gakkai Zasshi. 2013;117:270–92. [PubMed] [Google Scholar]
- 17.Oreja-Guevara C, González-Segura D, Vila C. Spasticity in multiple sclerosis: Results of a patient survey. Int J Neurosci. 2013;123:400–8. doi: 10.3109/00207454.2012.762364. [DOI] [PubMed] [Google Scholar]
- 18.Hecker M, Hartmann C, Kandulski O, Paap BK, Koczan D, Thiesen HJ, et al. Interferon-beta therapy in multiple sclerosis: The short-term and long-term effects on the patients’ individual gene expression in peripheral blood. Mol Neurobiol. 2013;48:737–56. doi: 10.1007/s12035-013-8463-1. [DOI] [PubMed] [Google Scholar]
- 19.Ohji S, Nomura K. The indication of steroid pulse therapy and apheresis therapy for multiple sclerosis. Nihon Rinsho. 2008;66:1127–32. [PubMed] [Google Scholar]
- 20.McDowell TY, Amr S, Langenberg P, Royal W, Bever C, Culpepper WJ, et al. Time of birth, residential solar radiation and age at onset of multiple sclerosis. Neuroepidemiology. 2010;34:238–44. doi: 10.1159/000297749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ramagopalan SV, Link J, Byrnes JK, Dyment DA, Giovannoni G, Hintzen RQ, et al. HLA-DRB1 and month of birth in multiple sclerosis. Neurology. 2009;73:2107–11. doi: 10.1212/WNL.0b013e3181c679f3. [DOI] [PubMed] [Google Scholar]
- 22.Sadovnick AD, Duquette P, Herrera B, Yee IM, Ebers GC. A timing-of-birth effect on multiple sclerosis clinical phenotype. Neurology. 2007;69:60–2. doi: 10.1212/01.wnl.0000265053.22905.64. [DOI] [PubMed] [Google Scholar]