

Abstract
Patient: Male, 89
Final Diagnosis: Right atrial myxoma
Symptoms: Syncope
Medication: None
Clinical Procedure: Echocardiogram • cardiac MRI
Specialty: Cardiology
Objective:
Unusual clinical course
Background:
Right atrial myxoma accounts for 15–20% of cardiac myxomas and syncope is a very rare manifestation. We present the case of an 89-year-old man with right atrial myxoma and syncope, and discuss the role of cardiac magnetic resonance imaging (MRI) in the diagnosis of myxomas.
Case Report:
An 89-year-old man with a history of hypertension, hyperlipidemia, chronic kidney disease stage 4, mild dementia, and benign prostatic hyperplasia presented to the emergency department with an episode of syncope. Physical examination demonstrated normal and regular heart sounds, and normal respiratory rate and oxygen saturation. Echocardiogram described a well-circumscribed echo-dense mass in the right atrial cavity, which was attached to the septum but not obstructing the tricuspid annulus, measuring 1.7×2.2 cm at its widest diameter. Cardiac MRI revealed a mass with dark intensity which enhanced heterogeneously following intravenous administration of gadolinium-chelate, consistent with a myxoma. The location of this myxoma, coupled with the presence of a stalk allowing mobility, provides a clue to how this patient experienced transient obstruction of the tricuspid valve leading to syncope.
Conclusions:
Right heart tumors should be considered in the differential diagnosis of unexplained syncope. Cardiac MRI with gadolinium-chelate administration can help differentiate this tumor from a right-sided atrial thrombus, which can pose a diagnostic challenge.
MeSH Keywords: Cardiac Imaging Techniques, Heart Neoplasms, Myxoma, Syncope, Tricuspid Valve
Background
Myxomas are the most common primary tumor of the heart and right atrial myxoma accounts for 15–20% of cases with this tumor [1]. Most of these are attached to the inter-atrial septum and are mostly asymptomatic but eventually can cause symptoms depending on the size, mobility, and location of the tumor [2,3]. Syncope is a rare manifestation of right atrial myxoma and its initial differentiation from a right atrial thrombus may be difficult. We present the case of an 89-year-old man with syncope who was found to have a right atrial myxoma.
Case Report
An 89-year-old man with a history of hypertension, hyperlipidemia, chronic kidney disease stage 4, mild dementia, and benign prostatic hyperplasia presented to our emergency department with an episode of syncope. He had a past history of positional syncope. Physical examination demonstrated normal and regular heart sounds, and normal respiratory rate and oxygen saturation. The syncope work-up including head computed tomography (CT); carotid Doppler, electroencephalogram, electrocardiogram, and orthostatic blood pressure were negative.
In the clinic, echocardiography described a well-circumscribed echo-dense mass in the right atrial cavity, attached to the septum but not obstructing the tricuspid annulus, measuring 1.7×2.2cm at its widest diameter, consistent with either an atrial thrombus or an atrial myxoma.
Cardiac MRI with gadolinium-chelate administration was conducted to further describe the mass. On cine bright blood steady-state free precession imaging, the mass was noted to be of dark intensity and it enhanced heterogeneously following intravenous administration of gadolinium-chelate, consistent with a myxoma (Figure 1). The freely mobile mass was attached with a thin stalk to the inferior-medial part of the tricuspid annulus near the ostium of the coronary sinus. The mass prolapsed freely into the tricuspid orifice during the cardiac cycle. Following the diagnosis of atrial myxoma, anticoagulation was considered but not started due to the patients’ history of recurrent falls. The patient was subsequently lost to follow-up.
Figure 1.
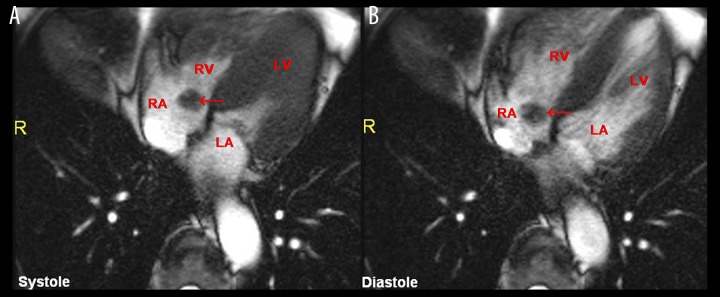
(A) Cardiac MRI showing atrial myxoma during systole. (B) Cardiac MRI showing atrial myxoma during diastole. RA – right atrium; RV – right ventricle; LA – left atrium; LV – left ventricle; arrow – myxoma.
Discussion
The most common causes of syncope in the elderly are orthostatic hypotension and reflex syncope (especially due to carotid sinus syndrome and cardiac arrhythmias) [4] and a cause is often not identified in the emergency room, especially in the elderly. Diagnosis may be complicated by other confounders of syncope (e.g., distinguishing mechanical falls from syncope may be difficult in elderly patients). Other considerations are drug interactions and dehydration [4]. The American Heart Association/American College of Cardiology Foundation Scientific Statement on the Evaluation of Syncope recommends that initial routine evaluation of the patient presenting with syncope should include careful history-taking, physical examination (including orthostatic blood pressure evaluation), and an electrocardiogram [5]. Further evaluation is recommended if a cause is not apparent after initial evaluation, and this includes echocardiography, an exercise test, and myocardial ischemia evaluation.
Right heart tumors should be considered in the differential diagnosis of unexplained syncope. Although right-sided myxomas are rare, they may present with right heart failure secondary to right ventricular outflow tract obstruction, or with syncope secondary to temporary complete obstruction of the tricuspid valve [3]. The main factor predicting obstructive sequelae is the tumor location. The location of this myxoma on the inferior-medial annulus of the tricuspid valve, coupled with the presence of a stalk allowing mobility, suggests why this patient experienced transient obstruction of the tricuspid valve leading to syncope. In a related study evaluating the risk factors for embolism in cardiac myxoma, location of the myxoma and irregular tumor surface were independently associated with increased risk of embolic complications [6]. A diagnostic dilemma may arise in the differentiation of a thrombus from a myxoma. Echocardiography is useful in the initial evaluation of a cardiac mass. Although echocardiogram images could not be retrieved to aid in the pictorial assessment of the tumor location in this report, the cardiac MRI images that were included provided a detailed description of the tumor location and attachment. A particular advantage of cardiac MRI is that it can be used to distinguish a thrombus from a tumor by providing more reliable tissue characterization. It is also better at assessing the relationship of a mass to cardiac structures [7]. Myxomas usually originate from the inter-atrial septum; they can be pedunculated or sessile, and the contours are mostly smooth. Thrombi usually occupy the atrial appendage; they are broad-based and have irregular contours. In general, myxomas, being vascular structures, tend to enhance with contrast administration, while thrombi do not [8].
Conclusions
Right heart tumors should be considered in the differential diagnosis of unexplained syncope. Cardiac MRI with gadolinium-chelate administration can help differentiate this tumor from a right-sided atrial thrombus, which can pose a diagnostic challenge.
References:
- 1.Reynen K. Cardiac myxomas. N Engl J Med. 1995;333(24):1610–17. doi: 10.1056/NEJM199512143332407. [DOI] [PubMed] [Google Scholar]
- 2.Surabhi SK, Fasseas P, Vandecker WA, et al. Right atrial myxoma in a patient presenting with syncope. Tex Heart Inst J. 2001;28(3):228–29. [PMC free article] [PubMed] [Google Scholar]
- 3.Azevedo O, Almeida J, Nolasco T, et al. Massive right atrial myxoma presenting as syncope and exertional dyspnea: Case report. Cardiovasc Ultrasound. 2010;8:23–23. doi: 10.1186/1476-7120-8-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Galizia G, Abete P, Mussi C, et al. Role of early symptoms in assessment of syncope in elderly people: Results from the Italian group for the study of syncope in the elderly. J Am Geriatr Soc. 2009;57(1):18–23. doi: 10.1111/j.1532-5415.2008.02070.x. [DOI] [PubMed] [Google Scholar]
- 5.Strickberger SA, Benson DW, Biaggioni I, et al. AHA/ACCF scientific statement on the evaluation of syncope: From the American Heart Association councils on clinical cardiology, cardiovascular nursing, cardiovascular disease in the young, and stroke, and the quality of care and outcomes research interdisciplinary working group; and the American College of Cardiology Foundation in collaboration with the Heart Rhythm Society. J Am Coll Cardiol. 2006;47(2):473–84. doi: 10.1016/j.jacc.2005.12.019. [DOI] [PubMed] [Google Scholar]
- 6.He DK, Zhang YF, Liang Y, et al. Risk factors for embolism in cardiac myxoma: A retrospective analysis. Med Sci Monit. 2015;21:1146–54. doi: 10.12659/MSM.893855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sparrow PJ, Kurian JB, Jones TR, Sivananthan MU. MR imaging of cardiac tumors 1. Radiographics. 2005;25(5):1255–76. doi: 10.1148/rg.255045721. [DOI] [PubMed] [Google Scholar]
- 8.Grizzard JD, Ang GB. Magnetic resonance imaging of pericardial disease and cardiac masses. Cardiol Clin. 2007;25(1):111–40. doi: 10.1016/j.ccl.2007.02.004. [DOI] [PubMed] [Google Scholar]