

Abstract
Introduction:
In dialysis centers both nephrologists and nurses are faced with the challenge of ensuring reliable and efficient care accordance with the clinical guideline. Hemodialysis adequacy monitoring information system therefore enable the automation of tasks, which ultimately allows doctors and nursing staff more time to dedicate to the individual treatment of patients. Development of the information systems in healthcare has made the use of the Minimum data set inevitable. The purpose of this study was determined MDS and capabilities required in hemodialysis adequacy monitoring information system.
Method and materials:
This is a cross-sectional survey conducted with participation of 320 nephrology specialists in 2015. Data were collected using an electronic questionnaire which was estimated as both reliable and valid. The data were analyzed by SPSS software descriptive statistics and analytical statistics.
Results:
Overall 42 data elements were determined as final set in 4 major categories (patient demographics, medical history, treatment plan and hemodialysis adequacy). The most capabilities required of hemodialysis information system were related to calculate of dialysis adequacy Index (4.80), advice optimal dose of dialysis for each patient (4.63), Easy access to information system without restrictions of time and place (4.61), providing alerts when dialysis adequacy index below the standard (4.55) and Interchange to other information systems in hospitals (4.46) respectively.
Conclusion:
In design and implementation of information systems focus on MDS and identification IS capabilities based on the users’ needs, due to the wide participation users and also the success of the information system. Therefore it is necessary that MDS evaluated carefully with regard to the intended uses of the data. Also information systems based on capabilities the ability to meet the needs of their users.
Keywords: hemodialysis adequacy monitoring, information system, minimum data set, capabilities required, nephrologists
1. INTRODUCTION
There are about 1.8 million patients with end stage renal disease all over the world (1). In Iran, the prevalence and incidence rates of ESRD have been on the increase from 49.9 patients per million of population in 2000 to 63.8 patients per million of population in 2006 (2). Hemodialysis is one of the main forms of renal replacement therapy (3). According to published statistics in 2014, about 23200 Iranian patients with ESRD are received hemodialysis (4). The typical frequency of HD treatments is three times per week and a session lasts on average 4 hours (5).
In dialysis centers both nephrologists and nurses are faced with the challenge of ensuring reliable and efficient care in accordance with the clinical guideline. Therefore, treatment should be carefully. On the other hand dialysis centers have limitations in machines, staff and time that must be legal provisions and economical requirements observed (6-8). Monitoring the adequacy of dialysis as the best solution to achieve a high quality of medical treatments and efficiency of resources is considered (9). Because of the complexity of the process of dialysis and the need for continuous assessment treatment plans, all information of main parameters for each patient has been recorded, processed, stored and retrieved effectively(7-10). The availability of data on both the planned and delivered treatment may lead to a thorough analysis of the plan effectiveness (11). The adequacy of hemodialysis is important determinant of the quality of life and has a direct impact on morbidity and mortality of patients (12).in Iran the adequacy of hemodialysis is so low, for instance Kt/V less than 1.2 and URR less than 65% were found in 56.7%, and 65.2% of the patients, respectively (13). Then basic strategy should be devised to improve it. The use of information systems as a supporting tool to improve reporting, assessment, and decision making processes (7). Hemodialysis adequacy monitoring information system therefore enable the automation of tasks, which ultimately allows doctors and nursing staff to dedicate more time to the individual treatment of patients (6). Development of the information systems in healthcare has made the use of the MDS inevitable (14). Minimum data set defined as: a minimum set of items of information with uniform definitions and categories concerning the specific dimension which meets the information needs of multiple data users in the healthcare system (15-17). Laing stated that the MDS prepared a framework for developing the necessary conditions for comprehensive documentation of the records (18). The results of a study performed by Lai showed that the AIDS MDS improved health through data exchange and was capable of changing the traditional interactions of care givers (19). Primary care specialists believed that the use of the MDS, electronic drug prescription, and electronic drug management enhanced the continuity of care (20).Also it is logical to identify basic IS capabilities that facilitate the fulfillment of this motive, due to the wide participation user in design and implementation information system (21).Aim of this paper is to determine Minimum data set and capabilities required in hemodialysis adequacy monitoring information system.
2. METHODOLOGY
This is a descriptive cross-sectional study conducted in 2015. The studied population consisted of nephrology specialists with at least two years work experience in dialysis centers which were 320 individuals in total. Data were collected through an electronic questionnaire that sends to nephrology specialists’ e-mail. The first part of the questionnaire is dedicated to the respondents’ demographic information including sex, age, work experience and university. The second part consists of 85 data elements in 4 major categories (patient demographics, medical history, treatment plan and hemodialysis adequacy) that experts were asked to review and score the initial set based on their importance by using a five-point Likert scale ranging from 1 to 5 where 1 referred to concept of “lowly important” and 5 indicated the statement of “highly important”. Data elements that were scored more than 3 included in the final minimum data set. In the final part also, capabilities required in hemodialysis adequacy monitoring information system determined. The validity of the instrument was determined based on concepts in the valid scientific texts and comments of experts (including nephrologists, dialysis nurses and health information managements). The reliability assessed through calculating Cronbach’s alpha that value it for the total questionnaire 0.86 obtained. Analysis was performed using SPSS software.
3. RESULTS
Out of 320 distributed questionnaires, 185 ones (57.8%) were collected. 53.3% of respondents were female and their mean age and work experience were 45.7 and 10.2 respectively (Figure1).
Figure 1.
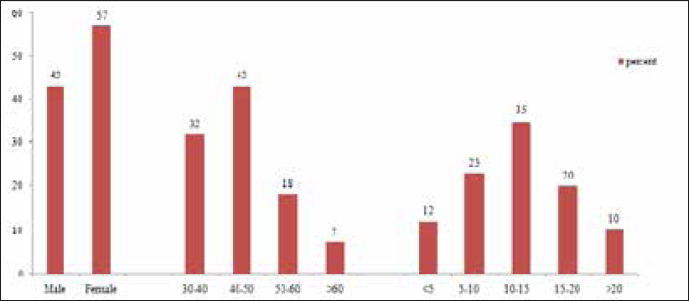
Respondent characteristics (sex, age and work experience)
Overall four classes of data (85 data items) were identified in the hemodialysis system. Data elements scored as highly important or important at least by more than 50 percent of the experts are presented in table 1. Overall 42 data elements were determined as final set (75% <) as follows:
Table 1.
Minimum Data Set for Hemodialysis information system
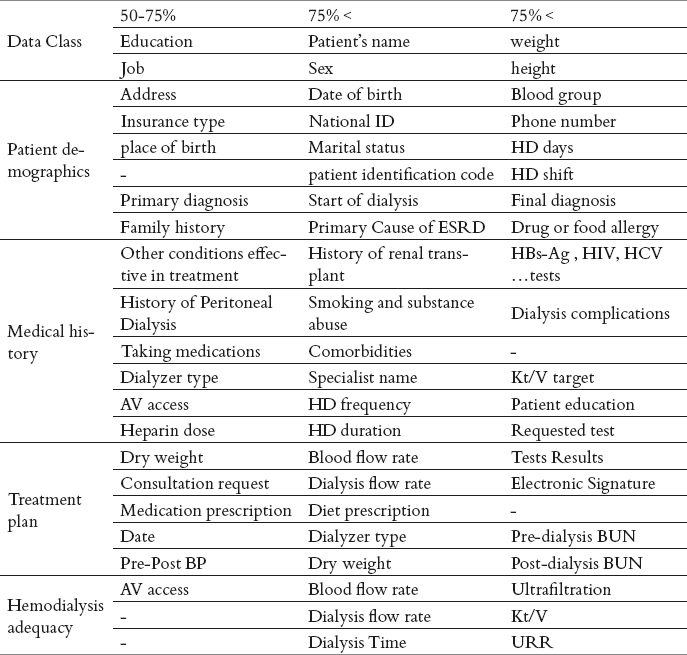
Patient demographics: name, sex, date of birth, national ID, marital status, weight, height, blood group, phone number, HD days and HD shifts.
Medical history: primary cause of ESRD, history of renal transplant, smoking and substance abuse, comorbidities, HBs-Ag, HIV, HCV …tests, drug or food allergy and final diagnosis.
Treatment plan: specialist name, HD frequency, HD duration, blood flow rate, dialysis flow rate, Kt/V target, requested test, tests results, patient education, diet prescription.
Hemodialysis adequacy: dialyzer type, dry weight, blood flow rate, dialysis flow rate, dialysis time, pre-post BUN, ultrafiltration, Kt/V and URR.
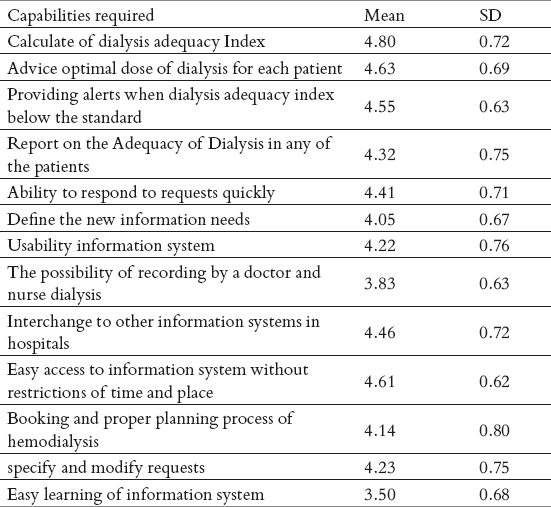
According to the table above, the most capabilities required of hemodialysis information system were related to calculate of dialysis adequacy Index (4.80), advice optimal dose of dialysis for each patient (4.63), Easy access to information system without restrictions of time and place (4.61), providing alerts when dialysis adequacy index below the standard (4.55), Interchange to other information systems in hospitals (4.46) and ability to respond to requests quickly (4.41) respectively.
Table 2.
Capabilities required of hemodialysis information system (range 1-5)
4. DISCUSSION
Sargent in an article entitled “Gathering Data in the Dialysis Unit: What Do You Need? “ suggested a better approach to the use of information systems in the dialysis unit, started with deciding what knowledge is desired. Once this is known, the information that is needed can be determined and finally the data required define and collect (22). In this study, in addition to the MDS to be determined capabilities required in hemodialysis information system.
From the perspective of nephrologists, in their study Ahmadi et al. (2012) the most important information needs in designing electronic health records of dialytic patients documentation included number, blood group, test and test results, type of dialysis, history of surgery and transplantation, cause of kidney failure, discharge recommendations and clinical alerts need to be prioritized (23). Our results showed that final MDS include: name, sex, date of birth, national ID, marital status, weight, height, blood group, phone number, primary cause of ESRD, history of renal transplant, smoking and substance abuse, comorbidities, HBs-Ag, HIV, HCV …tests, HD frequency, HD duration, blood flow rate, dialysis flow rate, Kt/V target, requested test, tests results, patient education, diet prescription, dialyzer type, dry weight, pre-post BUN, ultrafiltration, Kt/V and URR.
In a study, Kalankesh et al (2015) showed that overall six classes of data (46 items) were identified in the selected registry systems for cystic fibrosis: patient demographics, administrative data, survival status, diagnostic procedures, genetic and clinical manifestations, and therapeutics. Thirty two data elements from all six categories of data were approved by the experts as the minimum data set for cystic fibrosis registry system (15). In our research data elements were identified in 4 major categories (85 items): patient demographics, medical history, treatment plan and hemodialysis adequacy. Overall 42 data elements were determined as final set.
Bellazzi et al (2011) in a study for monitoring of hemodialysis treatment that automatically imports data from the hemodialysis monitoring software tools and analyzes the delivered treatment looking at six clinically relevant parameters (blood flow rate, dialysis time, arterial line pressure, venous line pressure, weight loss and dry weight). Failures-to-adhere (FtAs) to the planned treatment are detected and reported to the care-givers (24). in our study also these parameters in MDS of treatment plan and hemodialysis adequacy predicted.
In the study conducted by SUN (2006) interactivity (user interface), personalization (to specify and modify requests) and context-awareness (understand user preferences) as IS capabilities can be help users meet their information needs (21). Our results showed that the most capabilities required of hemodialysis information system were related to calculate of dialysis adequacy Index, advice optimal dose of dialysis for each patient, Easy access to information, Interchange to other information systems in hospitals, Usability information system and ability to respond to requests quickly.
5. CONCLUSION
Data collection is the most important part of information management and the minimum data sets is a standard tool for collecting data that guarantees access to accurate and precise health data.
Designing and performing of MDS in health centers can be considered as the beginning steps of any information system which result in improvement of the quality of care and disease control.
The MDS is a robust mechanism for collecting meaningful and comparable data at the regional and national level. In design and implementation of information, systems focus on MDS and identification IS capabilities based on the users’ needs, due to the wide participation users and also the success of the information system. Therefore it is necessary that MDS evaluated carefully with regard to the intended uses of the data. Also capabilities required information system should be the able to meet the needs of their users.
Acknowledgement
I sincerely appreciate all nephrologists that cordially contributed to this study.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Gotch F. The basic, quantifiable parameter of dialysis prescription is Kt/V urea;treatment time is determined by the ultrafiltration requirement;all three parameters are of equal importance. Blood purification. 2006;25(1):18–26. doi: 10.1159/000096392. [DOI] [PubMed] [Google Scholar]
- 2.Aghighi M, Heidary Rouchi A, Zamyadi M, Mahdavi-Mazdeh M, Rajolani H, Ahrabi S. Dialysis in Iran. Iran J Kidney Dis. 2008;2(1):11–15. [PubMed] [Google Scholar]
- 3.Javed F, Savkin AV, Chan GS, Mackie JD, Lovell NH. Recent advances in the monitoring and control of haemodynamic variables during haemodialysis: a review. Physiological measurement. 2012;33(1):R1. doi: 10.1088/0967-3334/33/1/R1. [DOI] [PubMed] [Google Scholar]
- 4.Mousavi S, Soleimani A, Mousavi M. Epidemiology of end-stage renal disease in Iran: A review. Saudi J Kidney Dis Transpl. 2014;25(3):697–702. doi: 10.4103/1319-2442.132242. [DOI] [PubMed] [Google Scholar]
- 5.Kalantar-Zadeh K, Ikizler TA. Let them eat during dialysis: an overlooked opportunity to improve outcomes in maintenance hemodialysis patients. J Ren Nutr. 2013;23:157–163. doi: 10.1053/j.jrn.2012.11.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bellazzi R, Sacchi L, Caffi E, de Vincenzi A, Nai M, Manicone F, et al. Implementation of an automated system for monitoring adherence to hemodialysis treatment: A report of seven years of experience. International journal of Medical Informatics. 2012;81(5):320–331. doi: 10.1016/j.ijmedinf.2012.01.007. [DOI] [PubMed] [Google Scholar]
- 7.Soetomo RD. A Knowledge-based Hemodialysis Health-Care Information System with Analytical Functions of Temporal Assessments for Monitoring and Treatment Plan of Hemodialysis Patient. 2012 [Google Scholar]
- 8.Lambie SH, Taal MW, Fluck RJ, McIntyre CW. Analysis of factors associated with variability in haemodialysis adequacy. Nephrology Dialysis Transplantation. 2004;19(2):40–46. doi: 10.1093/ndt/gfg570. [DOI] [PubMed] [Google Scholar]
- 9.Azar AT. A novel system for haemodialysis efficiency monitoring. International Journal of Healthcare Technology and Management. 2011;12(2):132–167. [Google Scholar]
- 10.Xie F, Zhang D, Wu J, Zhang Y, Yang Q, Sun X, et al. Design and implementation of the first nationwide, web-based Chinese Renal Data System (CNRDS) BMC medical informatics and decision making. 2012;12(1):11–15. doi: 10.1186/1472-6947-12-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yao ZM, Bai LJ, Guo FS. Design and Implementation of Hemodialysis Intelligent Management System. Applied Mechanics and Materials. 2012;121:1804–1808. [Google Scholar]
- 12.Adequacy H. Work Group. Clinical practice guidelines for hemodialysis adequacy, update 2006. Am J Kidney Dis. 2006;48(1):82–90. doi: 10.1053/j.ajkd.2006.03.051. [DOI] [PubMed] [Google Scholar]
- 13.Amini M, Aghighi M, Masoudkabir F, Zamyadi M, Norouzi S, Rajolani H, et al. Hemodialysis Adequacy and Treatment in Iranian Patients. Iranian journal of kidney diseases. 2011;5(2):103–109. [PubMed] [Google Scholar]
- 14.Cai S, Mukamel DB, Veazie P, Temkin-Greener H. Validation of the Minimum Data Set in identifying hospitalization events and payment source. J Am Med Dir Assoc. 2011;12(1):38–43. doi: 10.1016/j.jamda.2010.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kalankesh LR, Dastgiri S, Rafeey M, Rasouli N, Vahedi L. Minimum Data Set for Cystic Fibrosis Registry: a Case Study in Iran. Acta Iinform Med. 2015;23(1):18–21. doi: 10.5455/aim.2015.23.18-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mac Neela P, Scott PA, Treacy MP, Hyde A. Nursing minimum data sets: a conceptual analysis and review. Nursing inquiry. 2006;13(1):44–51. doi: 10.1111/j.1440-1800.2006.00300.x. [DOI] [PubMed] [Google Scholar]
- 17.Ahmadi M, Mohammadi A, Chraghbaigi R, Fathi T, Shojaee Baghini M. Developing a Minimum Data Set of the Information Management System for Orthopedic Injuries in Iran. Iran Red Crescent Med J. 2014;16(7):e17020. doi: 10.5812/ircmj.17020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Laing K. Use of the SGNA Minimum Data Set in the clinical area. Gastroenterol Nurs. 2005;28(1):59–60. doi: 10.1097/00001610-200501000-00015. [DOI] [PubMed] [Google Scholar]
- 19.Lai TY, Larson EL, Rockoff ML, Bakken S. User acceptance of HIV TIDES-Tailored Interventions for Management of Depressive Symptoms in persons living with HIV/AIDS. J Am Med Inform Assoc. 2008;15(2):217–226. doi: 10.1197/jamia.M2481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tamblyn R, Huang A, Kawasumi Y, Bartlett G, Grad R, Jacques A, et al. The development and evaluation of an integrated electronic prescribing and drug management system for primary care. J Am Med Informatic. 2006;13(2):148–159. doi: 10.1197/jamia.M1887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sun J. Assessing Goodness of Fit in Confirmatory Factor Analysis, Measurement and Evaluation in Counseling and Development. 2005; 37(4):240–256. [Google Scholar]
- 22.Sargent J. Control of dialysis by a single-pool urea model: the National Cooperative Dialysis Study. Kidney international Supplement. 1983;(13):S19. [PubMed] [Google Scholar]
- 23.Ahmadi M, Khoshkam M, Babaei R. Information Needs Study on Electronic Health Records of Dialysis Patients from Nephrologists’ Perspective. JHA. 2012;15(47):13–22. [Google Scholar]
- 24.Bellazzi R, Sacchi L, Caffi E, de Vincenzi A, Nai M, Manicone F, et al. Implementation of an automated system for monitoring adherence to hemodialysis treatment: A report of seven years of experience. International Journal of Medical Informatics. 2012;81(5):320–331. doi: 10.1016/j.ijmedinf.2012.01.007. [DOI] [PubMed] [Google Scholar]