

Abstract
Background/aim
Feedback on clinical reasoning skills during fieldwork education is regarded as vital in occupational therapy students' professional development. The nature of supervisors' feedback however, could be confirmative and/or corrective and corrective feedback could be with or without suggestions on how to improve. The aim of the study was to evaluate the impact of supervisors' feedback on final-year occupational therapy students' clinical reasoning skills through comparing the nature of feedback with the students' subsequent clinical reasoning ability.
Method
A mixed-method approach with a convergent parallel design was used combining the collection and analysis of qualitative and quantitative data. From focus groups and interviews with students, data were collected and analysed qualitatively to determine how the students experienced the feedback they received from their supervisors. By quantitatively comparing the final practical exam grades with the nature of the feedback, their fieldwork End-of-Term grades and average academic performance it became possible to merge the results for comparison and interpretation.
Results
Students' clinical reasoning skills seem to be improved through corrective feedback if accompanied by suggestions on how to improve, irrespective of their average academic performance. Supervisors were inclined to underrate high performing students and overrate lower performing students.
Conclusions
Students who obtained higher grades in the final practical examinations received more corrective feedback with suggestions on how to improve from their supervisors. Confirmative feedback alone may not be sufficient for improving the clinical reasoning skills of students.
Keywords: feedback, fieldwork education, mixed methodology research, physical dysfunction
Introduction
The purpose of undergraduate educational programmes in occupational therapy is to produce competent entry-level therapists who are able to master the challenges of practice (Dancza et al., 2013; Koski, Simon & Dooley, 2013; Richard, 2008). One of the challenges is acquiring sound clinical reasoning skills. Clinical reasoning is a complex thinking and doing process that requires memory, critical, creative and practical reasoning skills (Mattingly & Fleming, 1994; Sternberg, 2002). Students should learn to reason effectively throughout their undergraduate education by means of various teaching methods. According to the European Network of Occupational Therapists in Europe (ENOTHE, 2004), clinical reasoning skills should be acquired in a progressive way during the education programme. Learning should occur at a deeper level of reasoning during final year students' fieldwork education under the supervision of a registered occupational therapist (ENOTHE, 2004; Hills, Ryan, Smith & Warren-Forward, 2012). One way to acquire clinical reasoning skills is by means of quality feedback from supervisors during fieldwork education (Koski et al., 2013; Rodger, Fitzgerald, Davila, Millar & Allison, 2011; Thomas & Arnold, 2011). Bernard and Goodyear (2004, p. 5) are of the opinion that feedback is of prime importance for fieldwork supervision and state that without systematic feedback students may gain ‘no more than an illusion' that they are developing their skills.
Feedback on students' clinical reasoning occurs in a cycle of reciprocal influencing according to Vorster (2011). The cycle is the process whereby supervisors give information to students about their clinical reasoning skills and students have the choice on how to act upon the feedback. Egan (2002) classifies feedback as confirmatory or corrective. Through confirmatory feedback, students are informed whether they are effective in applying clinical reasoning skills, and with corrective feedback whether they are wandering off track, and how to improve their practise. The absence of feedback will not support any corrective action and will therefore have negative implications for their learning and professional development (Vorster, 2011). Also when no feedback is given, students are left to their own devices, which implies that learning, if any, takes place through trial and error, or through students believing they are doing what ought to be done (Chur-Hansen & McLean, 2006).
In a study at three universities in Australia, including 29 occupational therapy students, 41 practice educators and eight practice education staff, the importance of positive (confirmatory) and negative or critical (corrective) feedback was emphasised (Rodger et al., 2011). The student participants regarded critical (corrective) feedback as a crucial component of fieldwork education and appreciated a balance between positive (confirmatory) and critical (corrective) feedback. According to the authors, students felt they could deal with critical or negative (corrective) feedback if it was given in a constructive manner. Similar results were found in a survey by Koski et al. (2013) on effective fieldwork educator behaviours in occupational therapy. Thirty seven students and 85 supervisors from the eastern and western parts of the United States who completed the survey indicated that they valued fieldwork educators who used the evaluation process (summative assessment) to direct students in respect of strengths and opportunities for development. In a study by Ernstzen, Bitzer and Grimmer-Somers (2009) on physiotherapy students' and supervisors' perceptions of fieldwork opportunities, students also preferred mixed feedback. In addition, accurate feedback on their practical skills was considered beneficial by students.
In a four year longitudinal survey on the quality of fieldwork supervision among 108 physiotherapy and occupational therapy students' in Zimbabwe, students rated their supervisors as supportive and encouraging. The majority of supervisors were, however, found to overrate students' performance in the field (M'kumbuzi, Chinhengo & Kagseke, 2009).
At the university where the current study was conducted, it is standard procedure that final year occupational therapy students reflect, whether verbally or in writing, on their experiences of fieldwork education. The students' reflections noted that they experienced the supervisors' written and face-to-face feedback as predominantly critical or negative. Knowing that feedback influences the communication process (Vorster, 2011), this observation raised the question as to how the interpersonal relationship between supervisor and student impacts on the development of students' clinical reasoning in the field. Several authors maintain that it is the interpersonal communication between supervisor and student which underpin successful fieldwork (Chur-Hansen & McLean, 2006; Hummel, 1997). Therefore, supervisors' interpersonal communication messages that are clear and genuine may confirm or challenge a student, whereas dishonest messages “intentionally or unintentionally” will most likely impede the learning process of students (Bernard & Goodyear, 2004, p. 31).
Although a number of international studies on supervisors' interpersonal communication were identified (Bernard & Goodyear, 2004; Duffy, 2013; M'kumbuzi et al., 2009; McKimm, 2009), no published research could be found on the impact of occupational therapy supervisors' interpersonal communication on the clinical reasoning ability of students in the South African context.
A study was therefore undertaken with the aim of determining which interpersonal communication factors in the supervisory relationship play a role in enhancing occupational therapy students' clinical reasoning during their physical fieldwork education. This article reports one part of this study which sought to determine the impact of supervisors' feedback on student's clinical reasoning skills during their interactions with patients with physical dysfunction in hospitals. The specific objectives were:
-
To determine how students' Final Practical Examination (FPE) grades for clinical reasoning compared with:
Their summative assessment grades for clinical reasoning skills as allocated by their supervisors at the end of the physical fieldwork block (End of Term (EoT)).
Their Average Academic Performance (AAP) grades for the occupational therapy modules in final year.
To determine students' experiences of the nature of their supervisors' written and face-to-face feedback and how this feedback influenced their clinical reasoning ability as measured in the FPE.
Method
Design
A mixed-method approach was employed (Creswell, 2014). Qualitative and quantitative methods were integrated in a mixed-method approach with a convergent parallel design (Barg et al., 2006; Creswell, 2013a,b; Wittink, Barg & Gallo, 2006). The way in which the qualitative and quantitative data was integrated is set out in Table 1.
TABLE 1.
Mixed-method design of study
| Phase | Status | Ontology | Epistemology | Methodology |
|---|---|---|---|---|
| Data collection | QUAL | Inter-subjective reality of students | Empathetic interaction with students | Generating data from focus groups and semi-structured interviews |
| QUAN | External reality | Summative assessments by supervisors and examiners | Collecting students' EoT, AAP and FPE grades from archive | |
| Data analysis | QUAL | Inter-subjective reality | Inductive reasoning | Thematic content analysis |
| QUAN | Objective reality | Statistical analysis of quantified data | Pearson's product-moment coefficient | |
| Data interpretation | QUAL QUAN | Combination of subjective and objective reality | Inductive and deductive reasoning | Compare quantitative presentation of qualitative data with students EoT, FPE and AAP grades |
Setting
The study was carried out at a South African university with fourth year undergraduate occupational therapy students. Owing to the number of students (n = 36) in the programme, and limited fieldwork placements, students had to rotate through five fieldwork blocks representing different fields of occupational therapy namely, community rehabilitation, vocational rehabilitation, paediatrics, psychiatry and practices required for patients with physical dysfunction. The five blocks comprised 27 weeks in total and ranged from four to seven weeks per block. The focus in this study was on the students' clinical reasoning skills in the treatment of patients with physical dysfunction (six to seven weeks) as assessed by their supervisors, and the students' experiences of the feedback they received from their supervisors. The supervisors' assessment was summarised and recorded on a Work Competence Report (WCR) which comprises professional knowledge and skills, clinical reasoning, ethical behaviour, interpersonal relationships, professional development and work performance. This summative assessment of students' work competence occurs twice during each block. The first summative assessment was given by the supervisors halfway through the block (mid-term) and the second at the end of the fieldwork block (EoT). The outcome of this summative assessment was conveyed to the students by means of grades allocated for each aspect on the WCR, written comments as well as face-to-face feedback.
Ethics
The study was approved by the Ethics and Research Committee of the Faculty of Health Sciences at the university (134/2006). The chief executive officers of the six hospitals, and the heads of the involved occupational therapy clinical departments were fully informed about the research prior to its start. It was pointed out that data collected from focus groups and semi-structured interviews would be used for the study and that strict confidentiality in respect of the hospital, the supervisors and the students would be upheld. All gave written consent that the study may be conducted at their respective hospitals. Supervisors from each hospital were also visited by the researcher and fully informed about the research prior to the study.
Written consent for participating in the focus groups and semi-structured interviews was provided by each participant. Participants were informed of their right to withdraw from the study at any time, and that all data would be treated confidentially. All participants were assigned a code known to the researcher only to protect their identity.
The head of the occupational therapy department at the university where the study was registered gave consent for each final year student's FPE grade, AAP grades and WCR to be made available for the research study. The archived data were retrieved and captured by the researcher.
Participants
Physical fieldwork education is compulsory for all final year occupational therapy students at the university where the study was conducted. Owing to limited fieldwork placements, only 12 students could complete their physical fieldwork in each block at any time during the year. All final year students (n = 36) were recruited by the researcher on completion of their introduction to their physical fieldwork block, which was scheduled the day before their physical fieldwork block commenced. All agreed to be part of the study.
Data collection
Multiple sources and methods were used to collect data. Quantitative data were captured from students' WCRs (EoT grades) and examination records (FPE and AAP grades). Qualitative data were generated from the focus groups and semi-structured interviews in which the students shared their experiences of receiving written and face-to-face feedback on their clinical reasoning skills from their supervisors.
Quantitative data collection
Student' FPE grades: Towards the end of the academic year final year students are evaluated in a FPE by two examiners (one internal from the university, and one external from another higher educational institution) on their clinical reasoning skills at the same hospital where they completed their fieldwork education for people with physical dysfunction. A marking guideline developed from Du Toit's (2009) Levels of Creative Ability and essay on Initiative in Occupational Therapy is used to arrive at the final grade. The marking guideline consists of grades (in the form of ordinal categorical data and expressed as percentages), that describe different levels of knowledge, skills, insight and interaction. The rubric showing the criteria and descriptors for each marking band is presented in Table 2.
TABLE 2.
UP guideline for allocation of marking grades based on levels of creative ability and initiative in occupational therapy (Du Toit 2009)
| Grading bands |
||||||
|---|---|---|---|---|---|---|
| Criteria | 0–39% | 40–49% | 50–59% | 60–69% | 70–79% | 80–100% |
| Knowledge | Poor basic knowledge | Insufficient knowledge | Sufficient knowledge | Good knowledge | Excellent knowledge | Outstanding knowledge |
| Lack of professional terminology | Incorrect use of terminology | Command of essential terminology | Good command of terminology | Excellent command of terminology | Outstanding command of terminology | |
| Skill | Actions can harm or endanger client | Incorrect process Slow performance & awkward handling | Correct process. Un-systematic. Fair performance with cueing | Correct process Good performance & handling | Skilled performance in terms of speed & handling Can adapt process | Outstanding performance & integration |
| Insight | No insight into result of own actions | Insufficient insight to make correct deductions/adaptations | Basic insight (with cueing) to make some correct deductions | Good insight to make correct deductions | Excellent insight Can reason about implications & interrelations of deductions | Outstanding insight and reasoning |
| Interaction | Does not recognise client needs | Does not meet client needs | Appropriate interaction on clients level | Effective interaction Meets client needs in the session | Excellent interaction Can address needs beyond the session | Outstanding interaction & flexibility |
Students' EoT grades: Each student receives a marking grade for their clinical reasoning skills from their supervisors during their fieldwork placement education. EoT grades are based on the aforementioned marking guideline. As matrix supervision is employed (students are supervised by more than one therapist, and each supervisor has more than one student at a hospital) supervisors meet together when they write each student's WCR. On giving written and face-to-face feedback to each student, individual supervisor's comments are discussed so that students can follow up with the relevant supervisor. EoT grades (indicated on the student's WCR) were retrieved from the university's archive.
Students' AAP grades: Each student's average academic performance grade was calculated and averaged on completion of all occupational therapy modules in the final year. According to the university's guidelines, the contribution of the module on physical dysfunction to the AAP grade comprise of the year grade 50%, written exam grade 25% and practical examination (FPE) 25%. However, as the total grade for the module includes the FPE grade and the intention is to compare the FPE with average academic performance, the 25% contribution of the FPE was excluded from the total grade of this module with the written exam grade weight now taken as 50% of the total in determining the AAP grade.
Qualitative data collection
Focus groups and semi-structured interviews: Information on how the students' experienced the nature of feedback received from supervisors, in both the written WCR and face-to-face meetings, was generated from focus groups and semi-structured interviews. The focus groups were facilitated by the researcher on the first day after the end of the fieldwork block. Focus groups were conducted in English, because all students were proficient in this language. Key open-ended questions as presented below were used to guide the focus groups.
If you reflect on your fieldwork education what comes to mind?
How did you experience the feedback you received?
How would you describe the interpersonal communication between you and your supervisors?
The focus group discussions, lasting from 50 to 70 minutes were recorded. Immediately after a focus group the researcher reflected on the students' shared experiences.
Students who did not participate fully because of their mother tongue (Afrikaans (n = 15)), or whose verbal and non-verbal behaviour were contradictory (n = 7), were invited by means of a text message to participate in semi-structured interviews (Creswell, 2013a,b; Wittink, Barg & Gallo, 2006). All of them agreed. The interviews were carried out during the two weeks following the focus groups. The questions were open-ended and based on the students' experiences expressed in the focus group. The questions in the semi-structured interviews included the following:
In the focus group we discussed your experiences during the physical fieldwork block.
How did you really experience the feedback that was given to you?
Which feedback meant the most to you?
To what extent could you learn from the feedback?
Which feedback did you feel was invalid?
How do you feel about the grades you received at mid-term and end-of-term?
The interviews that lasted for 30–90 minutes were recorded. The notes based on the researcher's reflections on the student's verbal and non-verbal messages were also recorded immediately after the interviews.
Data analysis
Quantitative and qualitative research methods were employed to analyse the data.
Quantitative data analysis
The Pearson's product-moment correlation coefficient (Pearson's r) two-tailed test (Polit & Beck, 2010) was used to determine the correlation between the three forms of student grades. Therefore, FPE grades (allocated for clinical reasoning skills by an internal and an external examiner) were correlated with EoT grades (allocated for clinical reasoning skills by the supervisors at each hospital for physical dysfunction) as well as with students' AAP grades (combined grades for the occupational therapy modules in the final year, excluding the FPE grade in the module for physical dysfunction).
Qualitative data analysis
Owing to equipment failure, data from the third focus group and one semi-structured interview were lost. Data obtained from the remaining two focus groups and 21 semi-structured interviews were transcribed verbatim. These data were subsequently analysed by two coders independently to enhance rigour and trustworthiness. The main themes with associated sub-themes that emerged from the analysis, were used to establish the interpersonal communication factors in the supervisory relationship played a role in enhancing occupational therapy students' clinical reasoning during fieldwork education.
This article focusses on feedback, which emerged as one of the themes of supervisors' interpersonal communication.
The first coder was a lecturer in nursing sciences with expertise in qualitative analysis. She used a bottom-up approach and identified feedback as a theme, which she categorised as being positive or critical/negative. The occupational therapy researcher as second coder employed a top–down approach using ready-made categories, confirmatory or corrective, in terms of feedback,(Egan, 2002), and looked for comments fitting the categories (Terre Blanche, Durrheim & Kelly, 2006).
Comments and observations pertaining to feedback clearly referring to a specific supervisor were categorised as being confirmative, limited confirmative, corrective or limited corrective. If corrective, it was also noted where possible whether the feedback was accompanied by suggestions on how to improve. For each supervisor the number of comments in each category were then counted and aggregated on a percentage (frequency) basis (Creswell, 2014). If for instance, five out of six students described a supervisor as giving confirmative feedback, the supervisor would receive an 83% rating on confirmative feedback.
The average percentage all supervisors at a specific hospital received for either confirmative or corrective feedback was next determined to get an indication of the nature of feedback students at that hospital was generally exposed to.
The Pearson's r-test was subsequently used to measure the relationship between the students' mean FPE grade and their collective experience of the feedback as confirmative or corrective across the six hospital placements.
Results
Characteristics of sample
In all, 33 occupational therapy undergraduate final year students participated in the three focus groups with eleven students in each group. Three students did not participate because of logistical challenges. Of the 33 students 21 students participated in the semi-structured interviews. All were women, aged between 22 and 35 years and from Caucasian (n = 30) and Black African Ethnic (n = 3) groups.
Comparison of FPE grades with EoT grades
The students as a group, without taking hospital placement into account as shown in the last column of Table 3, obtained an average of 62.8% in the FPE and 68.7% at EoT with a negative correlation of −0.032 between the FPE and EoT. Notwithstanding this general indication that students are overrated at EoT the raw data reveals that supervisors underrated the three (9%) top performing students in the FPE, fairly accurately rated the next 12 (36%) students and generally overrated the clinical reasoning skills of the remaining 18 (55%) lower performing students.
TABLE 3.
Student grades in final practical exam, at end-of -term and average academic performance
| Hospital placement | I | II | III | IV | V | VI | Mean | Student group |
|---|---|---|---|---|---|---|---|---|
| Participant numbers | ||||||||
| Supervisors | 5 | 6 | 2 | 2 | 2 | 2 | 3 | 19 |
| Students | 6 | 9 | 4 | 6 | 4 | 4 | 6 | 33 |
| Student grades as a % | ||||||||
| FPE grades | 68.5% | 62.4% | 59.5% | 67.8% | 57.8% | 56.0% | 62.0% | 62.8% |
| EoT grades | 67.3% | 63.1% | 78.1% | 62.1% | 80.6% | 71.9% | 70.5% | 68.7% |
| Deviation: EoT > FPE | −1.2% | 0.6% | 18.6% | −5.7% | 22.9% | 15.9% | ||
| Correlation; FPE:EoT | −0.710 | −0.032 | ||||||
| AAP grades | 65.1% | 63.9% | 69.5% | 63.7% | 63.6% | 60.5% | 64.4% | 64.3% |
| Deviation: FPE > AAP | 3.4% | −1.5% | −10% | 4.2% | −5.9% | −4.5% | ||
| Correlation: FPE:AAP | 0.181 | 0.486 | ||||||
Based on the mean grade for each hospital, as shown in Table 3, the students' FPE grades on reasoning skills ranged between 56.0% and 68.5% (mean 62.0%; denoting sufficient to good knowledge on the marking guide in Table 2). At the EoT the mean grades ranged between 62.1% and 80.6% (mean of the EoT grades for the six hospitals was 70.5%, denoting excellent knowledge or skilled performance according to the marking guide). However, this tendency to overrate was not common to all hospitals as the deviation between the FPE grades and the EoT had a negative direction for hospitals I and IV and was almost absent at hospital II. Consequently, the level of correlation between the FPE and EoT for the six hospital placements was r = −0.710.
Comparison of FPE grades with AAP grades
The students as a group, without taking hospital placement into account, obtained an average AAP of 64.3% for all occupational therapy modules with a correlation between the FPE and AAP of r = 0.486.
Based on the mean grade for each hospital placement, the students' AAP grades ranged between 60.5% and 69.5% with a collective mean of 64.4%, which corresponds to a good knowledge or competent skill level on the marking guide. As shown in Table 3, the deviation between the FPE grades and the AAP grades was negative for four of the hospitals, although hospital II much less so than hospitals III, V and VI. The level of correlation between the FPE and AAP for the six hospital placements was r = 0.181.
Comparison of FPE grades with students' experience of the nature of feedback
The students' experiences of the feedback as confirmative or corrective varied between different hospitals as presented in Table 4.
TABLE 4.
Students' experiences of the nature of feedback
| Hospital placement | I | II | III | IV | V | VI |
|---|---|---|---|---|---|---|
| FPE grades | 68.5% | 62.4% | 59.5% | 67.8% | 57.8% | 56.0% |
| Students' experience | ||||||
| Confirmative feedback | 24.7% | 8.2% | 66.7% | 50.0% | 50.0% | 100% |
| Correlation FPE:Confirmative feedback | −0.624 | |||||
| Corrective feedback | 89.3% | 90.0% | 100% | 100% | 25.0% | 0.0% |
| Correlation FPE:Corrective feedback | 0.744 | |||||
Corrective feedback
Supervisors at four of the hospital placements (I, II, III and IV) were experienced by participants as giving corrective feedback at a level ≥89.3%. Supervisors at three of the hospitals (I, II and IV) were also experienced as giving guidance on how to improve. The correlation between the FPE and corrective feedback for the six hospital placements was r = 0.744.
Students valued a more experienced supervisor than someone who has just qualified, because they felt novice supervisors were hesitant in answering the questions and were unsure on how much feedback to give. Realistic corrective feedback, even if it seemed to be nit-picking, was perceived by students as a good learning opportunity..
I also learned a lot from a therapist if I can see that her therapy works, then I think, wow, that is a good therapist, then I automatically have respect for that therapist and any feedback they are willing to give me I will take and really look at it … (participant x)
Students were clear about their need to become competent occupational therapists. They were of the opinion that not getting sufficient feedback on their clinical reasoning, on what was poor and what needed to be improved on, was crucial for their professional development. On the whole students appreciated constructive meaningful feedback that assisted them in the development of their clinical reasoning skills.
…the feedback is not that they are trying to criticize you … but … if you are doing something wrong … they have to tell you. (participant bb)
… I think the critical feedback one gets… uhm… is also positive … in that a person could learn from it. They gave a lot of criticism … but… in the end … for the first time …I really knew how to do it.(participant r)
Confirmative feedback
The experiences of confirmative feedback ranged between 8.2% and 100% with a negative correlation (r = −0.624) between confirmative feedback and the average FPE grade for the six hospital placements.
The students had mixed feelings about the confirmative feedback they received. On the one hand confirmative feedback and good grades were welcomed, but on the other validity was put to question.
… it is nice to get good marks but I just wondered how reliable were the marks I received … did I get this mark because she liked me? (participant h)
It is possible that the supervisor gave confirmation and good grades because she felt unsure, did not want to upset the student or damage the supervisory relationship (M'kumbuzi et al., 2009; McKimm, 2009).
Some of the students, however, perceived confirmative feedback as an uplifting and encouraging experience.
…right at the end … the therapists told us in the past … students always wanted a lot of supervision and guidance (feedback) and at the end of term they told us we were not like that … we were even working as therapists.(participant c)
An analysis of the relationship between the FPE grades and the aggregated student experience of all supervisor feedback at the specific hospitals show a clear association between the nature of feedback and the student's ultimate performance in clinical reasoning (FPE grade) with the correlation between FPE and confirmative feedback being r = −0.624 and for corrective feedback r = 0.744. This relationship is graphically presented in Figure1 with the difference between FPE and AAP, which could be interpreted as the enhancement of clinical reasoning over and above expected academic performance, included for ease of reference.
FIGURE 1.
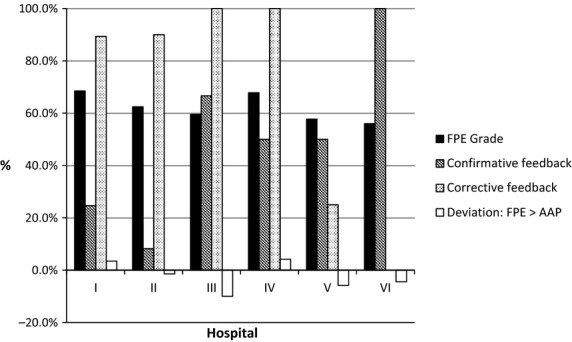
FPE grades compared with feedback according to students (Focus groups &semi-structured interviews).
Discussion
Although the students were allocated to hospital placements (and thus supervisors) based on logistical considerations (i.e. transport), there is always a possibility that the results could be skewed by the academically strong students accidentally ending up with supervisors exhibiting specific traits. The results indicate, however, that this did not seem to have happened as the correlation between AAP and FPE grade per hospital was low (r = 0.181). Furthermore, the average AAP grade per hospital was generally close to the mean overall AAP grade of 64.3%. The exception was Hospital III which seems to have had a higher number of academically strong students with an average AAP grade of almost 70% but which also showed the lowest improvement in clinical reasoning skills as represented by the deviation between FPE and AAP. It can therefore be surmised that general academic prowess does not in itself explain the students' performance in the FPE at the various hospital placements. This is particularly noticeable in the deviation between the average FPE and AAP values found at hospitals III, V and VI.
Supervisors generally rated students high at EoT compared to their achievement in the FPE. The correlation (r = −0.710) seem to indicate an inverse relationship between how the supervisors at the various hospitals rate the students and how they performed in the final practical exam. This is consistent with M'kumbuzi et al.'s (2009) findings. However, supervisors at hospitals I, II and IV tended to be much more realistic in their ratings based on the deviation between EoT and FPE grades.
Supervisors at hospitals I, II, III and IV scored between 89.3% and 100% on corrective feedback. However, reasonable doubt exists whether the feedback at Hospital III was actually constructive/corrective or just critical with no suggestion on how to improve. Supervisors at hospitals V and VI scored only 25% and 0% on corrective feedback. Given the relative high correlation between corrective feedback and the FPE grades (r = 0.744) for the six hospitals, and this despite the anomaly encountered at hospital III, the outcome of the FPE seems to be strongly influenced by supervisors' corrective feedback. This would suggest that supervisors were prepared to facilitate learning at a deeper level of reasoning at hospitals I, II and IV. On the other hand, the low incidence of corrective feedback encountered at hospitals V and VI could be because supervisors were reluctant to deal with students' not meeting the outcomes (Bernard & Goodyear, 2004). However, as evidenced by hospital III, corrective feedback without suggestions on how to improve would also not seem to enhance clinical reasoning among the students.
Students at hospitals I and II received only 24.7% and 8.2% confirmative feedback respectively while students at the other hospitals received 50% or more. In the case of hospital IV, however, the negative deviation (−5.7%) between EoT and FPE would seem to indicate that the confirmative feedback was realistic in the sense that credit was only given where deserved. This is not necessarily the case for hospitals III, V and VI where the deviation between EoT and FPE ranged from 15.9% to 22.9%.
It is further worth noting in the case of hospital IV that the 50% confirmative feedback was accompanied by a very high level of corrective feedback with suggestions on how to improve. This notion is supported by McKimm (2009) who maintains that corrective feedback should be accompanied by suggestions on how to improve. Similar results were found in a randomised controlled trial on medical students' reaction to feedback (Boehler et al., 2006). According to this study students who received specific, constructive feedback on how to improve their performance did significantly better (21.98 vs. 15.87, P < 0.001 on a post-/pre-test basis). Those students that received only compliments (confirmative feedback) showed no improvement although their average satisfaction rating was significantly better than the group that received constructive feedback. This suggests that students who receive confirmative feedback or are left to their own devices, do not know how to improve and so have to learn by themselves, often through trial and error. Furthermore novice supervisors may have been unaware of what students needed to work on (Bernard & Goodyear, 2004). M'kumbuzi et al. (2009) found that supervisors tend to overrate student performance as they fear low grades given to students may reflect their own inadequacies. Attempting to mend mistakes merely by giving confirmative feedback does not appear to enhance clinical reasoning.
Limitations
As the marking guide for the quantitative data collection was not tested, the collected data may be both invalid and unreliable. However, as research on the impact from supervisors' feedback is sparse, the results of this study contribute to needed knowledge. The particular influence of confirmative feedback was not evaluated in depth, which means that conclusions about confirmative feedback must be drawn with caution. A deeper analysis of confirmative feedback would elucidate the validity of the finding that unsubstantiated confirmative feedback has very little impact, but deserved confirmative feedback could contribute to the students, learning experience and motivation. Further research is needed in this respect. Likewise, it may have shown whether corrective feedback incorporating active demonstration of the correct way to execute treatment contribute to the students' learning experience.
Other limitations are the small sample size and the locality and gender of the participants in the sample, which means that the results may not be generalised either within South Africa or internationally, as only female students from one university were included in the study.
Implications
To draw more confident conclusions on the impact of supervisors' rating of students' clinical reasoning skills, the validity, test-retest reliability and inter-rater reliability of the instrument used in this study (marking guide), must be secured.
Feedback, whether confirmative or corrective in nature, and its use as a valuable learning tool, should be clearly understood and applied by supervisors to enable students to maximise their learning. The results indicate that the supervisors included in this study were not fully equipped in all respects of their role in the fieldwork education of students. If this is the case it is strongly recommended that all supervisors receive education on the theoretical underpinning and practical application of constructive and confirmative feedback. The development of a goal-orientated and accredited fieldwork-education programme that integrates the relevant concepts of clinical education with the roles and responsibilities of the supervisor, student and faculty should be researched.
A multisite study to remove any possible institutional bias with participants of both sexes should be carried out in a longitudinal study.
Conclusion
Giving constructive critical feedback on the students' clinical reasoning skills seems to be key to their development as entry-level occupational therapists. Constructive feedback that focuses on students' specific clinical reasoning skills and offers suggestions on how to improve seems tobe more effective than confirmative feedback.
The students' responses indicate that they respected and learnt from supervisors who were experienced as competent in their field of practice, who gave specific feedback, and facilitated their clinical reasoning skills to arrive at optimal solutions for goal achievement.
Acknowledgments
We thank the participants who willingly reflected on their experience and Prof Charl Vorster and Dr Carin Maree for their reflections on the emerging results.
References
- Barg FK, Huss-Ashmore R, Wittink MN, Murray GF, Bogner HR, Gallo JJ. A mixed-methods approach to understanding loneliness and depression in older adults. Journal of Gerontology: Social Sciences. 2006;61B:S329–S339. doi: 10.1093/geronb/61.6.s329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernard JM, Goodyear RK. Fundamentals of clinical supervision. 3rd ed. Boston, MA: Pearson Education; 2004. [Google Scholar]
- Boehler ML, Rogers DA, Swind CJ, Mayforth R, Quin J, Williams RG, Dunnington G. An investigation of medical student reactions to feedback: A randomised control trial. Medical Education. 2006;40:746–749. doi: 10.1111/j.1365-2929.2006.02503.x. [DOI] [PubMed] [Google Scholar]
- Chur-Hansen A, McLean S. On being a supervisor: The importance of feedback and how to give it. Australasian Psychiatry. 2006;1:67–71. doi: 10.1080/j.1440-1665.2006.02248.x. [DOI] [PubMed] [Google Scholar]
- Creswell JW. Research design. Qualitative, quantitative and mixed method approaches. 3rd ed. London: Sage; 2013a. [Google Scholar]
- Creswell JW. Steps in conducting a scholarly mixed methods study. Lincoln: DigitalCommons@University of Nebraska; 2013b. [Google Scholar]
- Creswell JW. Research design. Qualitative, quantitative and mixed method approaches. 4th ed. London: Sage; 2014. [Google Scholar]
- Dancza K, Warren A, Copley J, Rodger S, Moran M, McKay E, Taylor A. Learning experiences on role-emergency placements: An exploration from students' perspectives. Australian Occupational Therapy Journal. 2013;60:427–435. doi: 10.1111/1440-1630.12079. [DOI] [PubMed] [Google Scholar]
- Du Toit V. Pretoria: Vona & Marie du Toit Foundation; 2009. Patient volition and action in occupational therapy. (4th ed.) [Google Scholar]
- Duffy K. Providing constructive feedback to students during mentoring. Nursing Standard. 2013;27:50–56. doi: 10.7748/ns2013.04.27.31.50.e7334. [DOI] [PubMed] [Google Scholar]
- Egan G. The skilled helper: A problem-management and opportunity-development approach to helping. 7th ed. Pacific Grove, CA: Brooks/Cole; 2002. [Google Scholar]
- ENOTHE. Occupational Therapy Education in Europe: PBL Stories & Signposts towards a problem based learning orientated curriculum. Amsterdam: ENOTHE; 2004. [Google Scholar]
- Ernstzen DV, Bitzer E, Grimmer-Somers K. Physiotherapy students' and clinical teachers' perceptions of clinical opportunities: A case study. Medical Teacher. 2009;31:e102–e115. doi: 10.1080/01421590802512870. [DOI] [PubMed] [Google Scholar]
- Hills C, Ryan S, Smith DR, Warren-Forward H. The impact of ‘Generation Y’ occupational therapy students on practice education. Australian Occupational Therapy Journal. 2012;59:156–163. doi: 10.1111/j.1440-1630.2011.00984.x. [DOI] [PubMed] [Google Scholar]
- Hummel J. Effective fieldwork supervision: Occupational therapy students' perspectives. Australian Occupational Therapy Journal. 1997;44:147–157. [Google Scholar]
- Koski KJ, Simon RL, Dooley NR. Valuable occupational therapy fieldwork educator behaviours. Work. 2013;44:307–315. doi: 10.3233/WOR-121507. [DOI] [PubMed] [Google Scholar]
- Mattingly C, Fleming MH. Clinical reasoning. Forms of inquiry in a therapeutic practice. Philadelphia: F. A. Davis Company; 1994. [Google Scholar]
- McKimm J. Giving effective feedback. British Journal of Hospital Medicine. 2009;70:158–161. doi: 10.12968/hmed.2009.70.3.40570. [DOI] [PubMed] [Google Scholar]
- M'kumbuzi VRP, Chinhengo TPT, Kagseke F. Perception of physiotherapy and occupational therapy students' supervision of field attachment in Zimbabwe. Asia Pacific Disability Rehabilitation Journal. 2009;20:112–128. [Google Scholar]
- Polit DF, Beck CT. Essentials of nursing research: Appraising evidence based practice. 7th ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins; 2010. [Google Scholar]
- Richard LF. Exploring connections between theory and practice: Stories from fieldwork supervisors. Occupational Therapy in Mental Health. 2008;24:154–175. [Google Scholar]
- Rodger S, Fitzgerald C, Davila W, Millar F, Allison H. What makes a quality occupational therapy practice placement? Students' and practice educators' perspectives. Australian Occupational Therapy Journal. 2011;58:195–202. doi: 10.1111/j.1440-1630.2010.00903.x. [DOI] [PubMed] [Google Scholar]
- Sternberg RJ. Raising the achievement of all students: Teaching for successful intelligence. Educational Psychology Review. 2002;14:383–393. [Google Scholar]
- Terre Blanche M, Durrheim K. First steps in qualitative data analysis. In: Terre Blanche M, Durrheim K, Painter D, Kelly K, editors. Research in practice: Applied methods for the social sciences. Cape Town: University of Cape Town Press; 2006. pp. 321–344. [Google Scholar]
- Thomas JD, Arnold RM. Giving feedback. Journal of Palliative Medicine. 2011;14:233–239. doi: 10.1089/jpm.2010.0093. [DOI] [PubMed] [Google Scholar]
- Vorster C. IMPACT: The story of interactional therapy. Pretoria: SATORI; 2011. [Google Scholar]
- Wittink MN, Barg FK, Gallo JJ. Unwritten rules of talking to doctors about depression: Integrating qualitative and qualitative methods. Annals of Family Medicine. 2006;4:302–309. doi: 10.1370/afm.558. [DOI] [PMC free article] [PubMed] [Google Scholar]