

Abstract
Background:
Health systems play key roles in identifying tobacco users and providing evidence-based care to help them quit. This treatment includes different methods such as simple medical consultation, medication, and telephone counseling. To assess different quit smoking methods selected by patients in tobacco cessation centers in Iran in order to identify those that are most appropriate for the country health system.
Methods:
In this cross-sectional and descriptive study, a random sample of all quit centers at the country level was used to obtain a representative sample. Patients completed the self-administered questionnaire which contained 10 questions regarding the quality, cost, effect, side effects and the results of quitting methods using a 5-point Likert-type scale. Percentages, frequencies, mean, T-test, and variance analyses were computed for all study variables.
Results:
A total of 1063 smokers returned completed survey questionnaires. The most frequently used methods were Nicotine Replacement Therapy (NRT) and combination therapy (NRT and Counseling) with 228 and 163 individuals reporting these respectively. The least used methods were hypnotism (n = 8) and the quit and win (n = 17). The methods which gained the maximum scores were respectively the combined method, personal and Champix with means of 21.4, 20.4 and 18.4. The minimum scores were for e-cigarettes, hypnotism and education with means of 12.8, 11 and 10.8, respectively. There were significant differences in mean scores based on different cities and different methods.
Conclusions:
According to smokers’ selection the combined therapy, personal methods and Champix are the most effective methods for quit smoking and these methods could be much more considered in the country health system.
Keywords: Cessation, health services, patients, tobacco
INTRODUCTION
Without effective tobacco control measures, it is estimated that by the year 2030, the annual global death toll will reach 8 million.[1,2] With current smoking patterns, approximately 500 million people alive today will eventually be killed by tobacco use.[3] Currently, there are an estimated 1.3 billion smokers in the world.[4] Most smokers indicate interest in quitting, three out of four smokers say they want to quit.[5] One of the core responsibilities of the health system should be to treat tobacco dependence. This treatment includes different methods such as simple medical consultation, medication, and telephone counseling. The cost of these methods differs and would not have the same effect on different smokers.[6] It should be noted that treatments need to be tailored and delivered appropriately for individuals according to their age, gender, interest, needs and also cultural and local conditions.[7] Repeated consultation at each clinical visit would reinforce the necessity for quitting.[8,9] Furthermore, consultation by health interns can significantly increase the quit rates.[10] This intervention is relatively cost-effective because it is a part of available services, which people rarely use. Such interventions are very effective because they are provided by health care providers who are respected by most people and with whom smokers tend to have good interactions.[11,12]
In addition to medical advice and telephone consultation for quitting, an effective method can also include medication. Medication includes various forms of nicotine replacement therapy (NRT) such as patches, gum, lozenges, and nasal spray and also prescription drugs such as bupropion and varenicline.[13]
After 10 years of the first educational intervention for quitting smoking and one or two complementary programs in the Iran health system network, and in some attached centers (including group therapy and free 15 mg nicotine patch) the same interventions are still being implemented with little documentation of effectiveness.[14,15,16,17] Therefore, different treatments including more recent treatments need to be studied and assessed and the most appropriate ones selected and developed at the country health system level. This should include among other factors demands on human resources and availability and cost of medication services. It is important for us to know how these treatments were viewed by patients. In undertaking this assessment, it is important to include patient selection on the methods they have experienced. The aim was to study and assess patients’ selection of different quit smoking methods provided in tobacco cessation services centers in Iran in order to identify those that could be as one of the most appropriate for the country health system.
METHODS
This cross-sectional and descriptive study was conducted in smoking cessation services centers in Iran in 2012–2013. In each Iran's province, there is a university under the supervision of Ministry of Health and Medical Education. Therefore, primary health care services are provided by universities of medical sciences and national tobacco control programs provided by these universities, and there is a person to coordinate these activities in the affiliated centers all across the provinces. There were approximately 50–60 smoking quit centers, which are working under the supervision of health centers in primary health care system, but many of these were not active in presenting tobacco cessation services. 13 active centers in 7 cities were selected (whether public or private) with the goal of obtaining a representative sample size of 1066 subjects by using the following formula:

In a randomly selected day based on first-come, first-serve basis and agreement to join the study, smokers at all active quit centers throughout the country completed the questionnaire. The researchers visited the centers during June 2012 and asked a randomly selected sample of smokers (minimum 10 from each center) to complete an anonymous, self-administered questionnaire during their visit to the center. The contents of the primarily structured questionnaire were designed by the first author based on review of the relevant literature and the authors’ preliminary research.[13,14,15,16,17] Its psychometric properties were evaluated in terms of face and content validity through a panel discussion with seven tobacco control experts in Iran who had experience in tobacco cessation programs. This discussion continued until a convergence of opinions was reached. The reliability coefficient (Cronbach alpha) for the questionnaire was assessed through test-retest on a sample of 15 patients (α = 0.88). The questionnaire also was piloted before distribution.
In tobacco control expert panels, 30 scores were included for assessment. The questionnaire contained 10 questions (3 scores each) regarding the quality, cost, effect, side-effects and the results of quitting methods using a 5-point Liker-type scale from 1 to 3 to have maximum 30 for each. For maximum coverage the centers of seven cities in different geographic regions such as Tehran, Isfahan, Shiraz, Mashhad, Tabriz, Hamedan and Sari were selected (these centers were identified through necessary coordination with the Deputy for Health and Curative Affairs in each province). Prior to distribution of the questionnaire, the purpose and nature of the study were explained to the relevant authorities in each center and also to the randomly selected participants and informed consent was obtained in order to inform the participants regarding the aim of study, feel free to join the study, and other ethical and confidential issues.
All survey responses were entered into a data set and double keyed to ensure accurate data entry. Percentages, frequencies, mean, t-test and variance analysis were computed for all study variables. Analyses were conducted using SPSS 16.00 statistical software (SPSS Inc., Chicago, IL, USA).
RESULTS
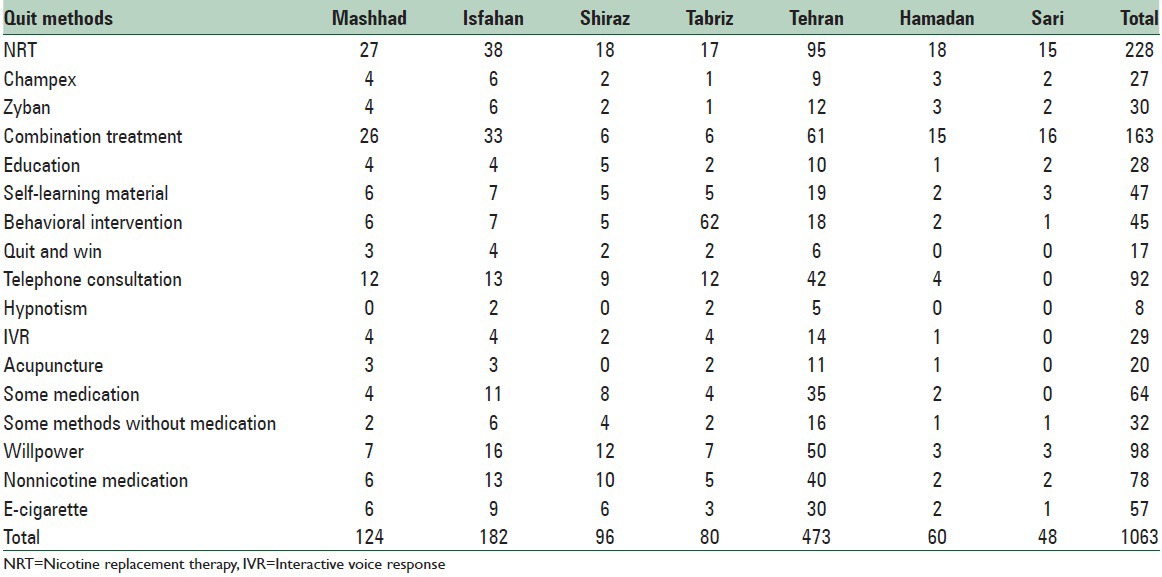
In this study, a total of 1063 out of 1384 smokers returned completed the survey questionnaire (response rate was 77%). Most respondents were from Tehran with 473 cases, using all methods, while in other cities some methods were not accessible or the patients did not use them. For example in Sari city, only 48 cases answered the questionnaire. The most frequently used methods were NRT and combination methods (NRT and counseling) with 228 and 163 cases, respectively. The least used methods were hypnotism (n = 8) and the quit and win method (n = 17) [Table 1].
Table 1.
Frequency distribution of study sample by methods and cities in Iran in 2012-2013
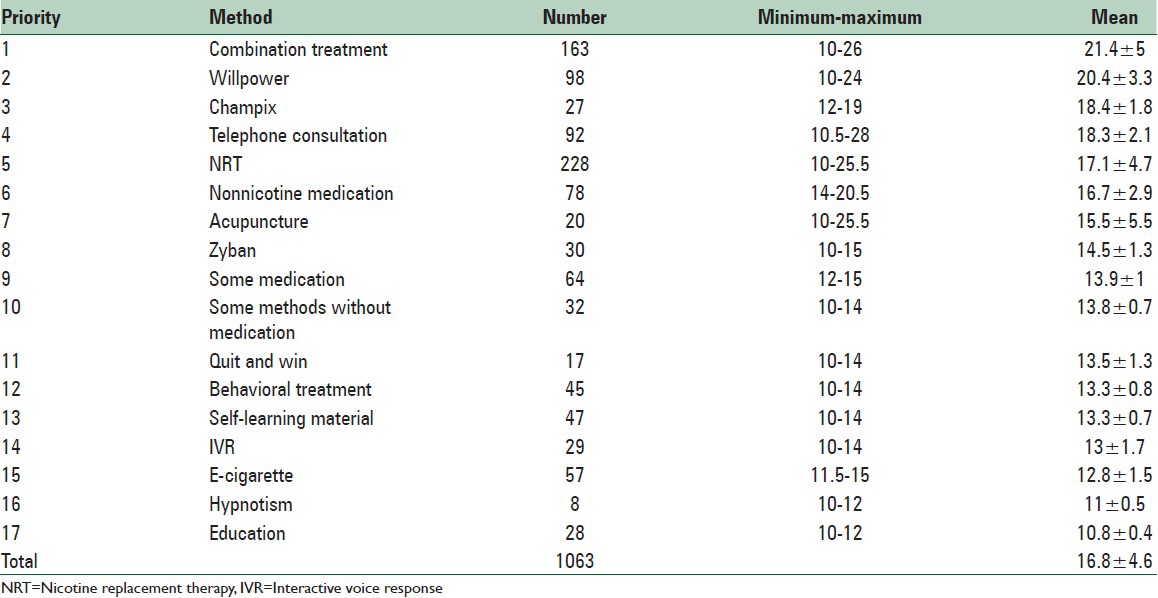
The mean score of all used methods in our study was 16.8 ± 4.6 (minimum 10–maximum 26). A score of 26 was given to combination methods and 10 to different methods. The methods which received the maximum scores were combined methods, willpower and Champix with means of 21.4, 20.4 and 18.4, respectively. The minimum scores were assigned to e-cigarettes, hypnotism and education with means of 12.8, 11 and 10.8, respectively [Table 2].
Table 2.
Prevalence and score obtained for each quit smoking method based on patients' opinion and according to their priority
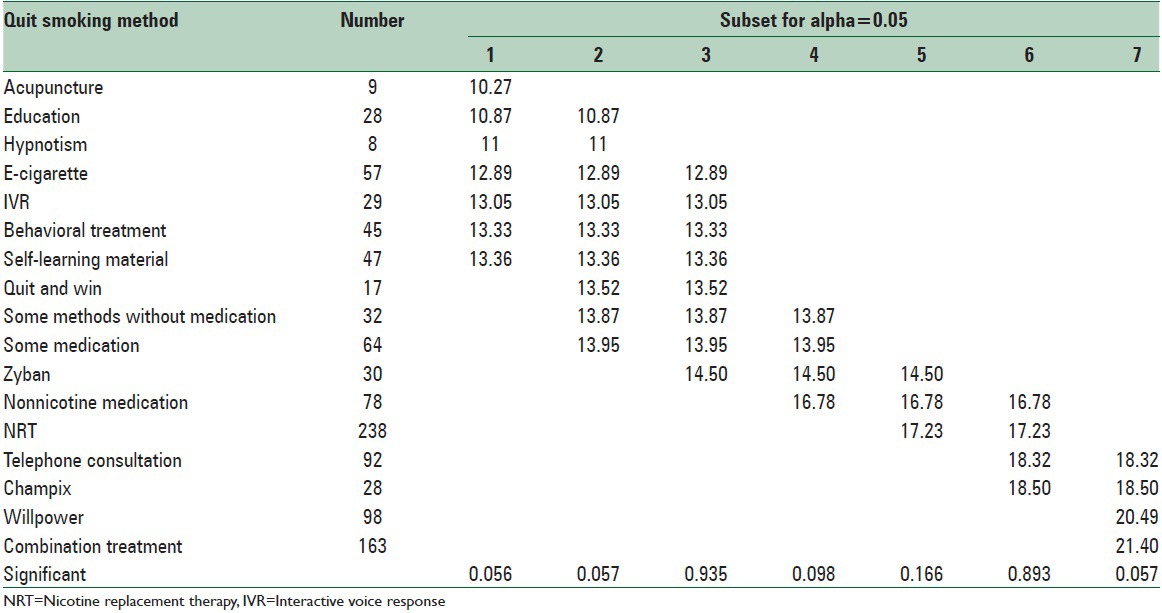
There were significant differences in mean scores based on different cities and in the mean scores of different methods [Table 3]. The cities of Hamadan and Sari gained the maximum scores (P < 0.000) and combined methods, personal, Champix and quitlines gained the maximum scores (P < 0.000). Invariance analysis on mean scores of different methods, there were significant differences among methods, and combined treatment, personal, Champix and telephone consultation gained the maximum scores (P < 0.000) [Table 4].
Table 3.
Analysis of variance of mean scores for patients’ opinions on quit smoking methods in different cities of Iran, 2012
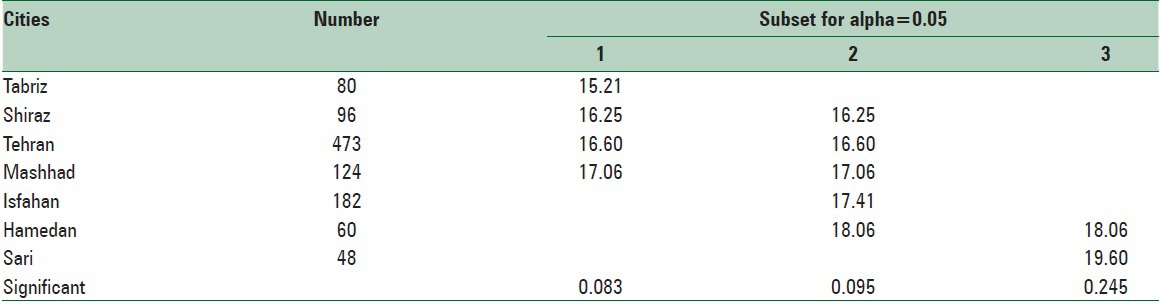
Table 4.
Analysis of variance of mean score provided through patients’ opinion towards different methods of quit smoking in Iran, 2012
There were no significant differences in patients’ mean scores of according to their gender (P = 0.19) [Tables 5 and 6].
Table 5.
Patients mean scores according to their gender in Iran, 2012
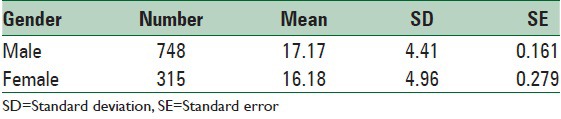
Table 6.
T-test for equality of means score obtained from patients’ opinion regarding different quit methods according to their gender in Iran, 2012

DISCUSSION
In this study, the selection and opinions of the smokers toward different quitting methods revealed that the combination therapy, personal, Champix and telephone consultation were viewed as the most effective methods in the country. It is important to know the patients’ opinions in order to up to date our services at the country level for enhanced success. Among these four preferred methods, the combination therapy treatment was the first priority, and we assume that this could be due to its availability free of charge and also its group therapy approach.[14,15] This method also has been recommended in prior studies.[18,19] For personal methods that were rated as a second priority, we considered that this may be due to the fact that the use of personal methods demonstrates the high motivation of smokers to quit smoking. Other studies have not confirmed this idea,[20] however, and it may be considered as a starting point for further complementary studies. Use of Champix has been implemented once (free of charge) and revealed a good result.[21] Telephone consultation was identified as a fourth priority, and this could also be due to its accessibility at the country level. This result also is consistent with similar studies.[12,22,23]
These seventeen treatment methods for quit smoking can be divided into three groups as follows:
Group with high priority: Combination therapy, willpower, champix, telephone consultation, NRT, nonnicotine medication.
Group with medium priority: Acupuncture, zyban, some medications (such as anti-depression drugs), some methods without medication (for example counseling and watching movies), quit and win, behavioral treatment.
Group with low priority: Learning material, interactive voice response, e-cigarettes, hypnotism, and education.
Consideration should be given to not using the low priority methods.
It was observed that there are significant differences in mean scores for quitting methods among the seven cities [Table 3]. We had assumed that these methods would receive higher scores in Tehran compared to other cities (due to long-term experience and the availability of the centers). However, contrary to our expectations, the highest scores were reported in Sari and Hamadan city. Further research should be done to investigate this result. According to the variance analysis conducted to compare methods (and despite the fact that there were significant differences between the methods); four quit methods, including combination therapy, willpower, and Champix were identified as best. There were no significant differences among the remaining six quit methods [Table 4]. This table indicates that one appropriate method may be selected from among the methods in each group based on present conditions, including patients’ and physicians’ preference and satisfaction.
There also was no significant difference between women and men in this study, in contrast to Gilpin and Pierce's findings.[24] This study demonstrated that patients prefer to use combination therapy individually (not group therapy) and this issue should be considered for the supplementary further study.
The results of this study are important because few studies have assessed real world responses of patients who used different smoking treatment methods. Thus, one potential follow-up from this study could be a training program for health care providers on effective methods to treat smokers. For example, acupuncture has not been proven effective as a tobacco treatment method, yet it was reported as a medium priority treatment by the participants. An important limitation of this study is the cross-sectional nature of the data. This makes it impossible to determine the impact of each method on quitting result. Another important limitation was inability of health policy makers to make necessary final decision for tobacco control program based of the result of this study and future studies should focus on the quality, such as cost-effectiveness, time, and side effects of each cessation method.
This study also reflects the international discussion that has occurred regarding the role of formal treatment relative to self-quitting[21] since participants reported that both willpower and medications like varenicline were most effective for helping them quit smoking. Willpower can be considered an indicator of motivation, and our experience is that those who are most motivated to quit might be the most successful ones. And when that motivation is coupled with an effective medication, the chances of being successful increase even more. Thus, the results of this study reflect the wisdom our patients because they recognize that smoking treatment requires more than just taking a medication, but it also reflects the need to train more healthcare workers to assure they help their patients with the most effective methods.
CONCLUSIONS
Patients’ opinions revealed that combination therapy, willpower, Champix and telephone consultation are the most effective quit methods in the country and that quit centers will have more patients successfully quit smoking using these methods.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Peto R, Lopez AD, Boreham J, Thun M, Heath C Jr, Doll R. Mortality from smoking worldwide. Br Med Bull. 1996;52:12–21. doi: 10.1093/oxfordjournals.bmb.a011519. [DOI] [PubMed] [Google Scholar]
- 3.Levin R, Kinder M. Washington, DC: Center for Global Development; 2004. [Last accessed on 2014 May 22]. Millions saved: proven success in global health? Available from: http://jama.jamanetwork.com/article.aspx?articleid=207156 . [Google Scholar]
- 4. [Last accessed on 2013 Jun 13]. Available from: http://www.apps.who.int/iris/bitstream/10665/85380/1/9789241-eng.pdf?page12 .
- 5.Jones JM. Smoking Habits Stable; Most Would Like to Quit; 18 July, 2006. 2006. Jul 18, [Last accessed on 2007 Dec 06]. Available from: http://www. g a l lup.com/poll/23791/Smoking-Habits-Stable-Most-Would-Like-Quit.aspx .
- 6. [Last accessed on 2013 Jun 13]. Available from: http://www.apps.who.int/iris/bitstream/10665/85380/1/9789241-eng.pdf?page58.60 .
- 7.Feenstra TL, Hamberg-van Reenen HH, Hoogenveen RT, Rutten-van Mölken MP. Cost-effectiveness of face-to-face smoking cessation interventions: A dynamic modeling study. Value Health. 2005;8:178–90. doi: 10.1111/j.1524-4733.2005.04008.x. [DOI] [PubMed] [Google Scholar]
- 8.Solberg LI, Maciosek MV, Edwards NM, Khanchandani HS, Goodman MJ. Repeated tobacco-use screening and intervention in clinical practice: Health impact and cost effectiveness. Am J Prev Med. 2006;31:62–71. doi: 10.1016/j.amepre.2006.03.013. [DOI] [PubMed] [Google Scholar]
- 9.West R, Sohal T. “Catastrophic” pathways to smoking cessation: Findings from national survey. BMJ. 2006;332:458–60. doi: 10.1136/bmj.38723.573866.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fiore MC. Rockville, MD, U.S: Department of Health and Human Services, Press Briefing; 2000. [Last accessed on 2007 Dec 16]. Treating Tobacco Use and Dependence: A Public Health Service Clinical Practice Guideline. Available from: http://www.surgeongeneral.gov/tobacco/mf062700.htm . [Google Scholar]
- 11.Bao Y, Duan N, Fox SA. Is some provider advice on smoking cessation better than no advice? An instrumental variable analysis of the 2001 National Health Interview Survey. Health Serv Res. 2006;41:2114–35. doi: 10.1111/j.1475-6773.2006.00592.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Owen L. Impact of a telephone helpline for smokers who called during a mass media campaign. Tob Control. 2000;9:148–54. doi: 10.1136/tc.9.2.148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pfizer for Professionals. Mechanism of Action of CHANTIX™ (Varenicline) 2007. [Last accessed on 2007 Dec 06]. Available from: https://www.pfizerpro.com/product_info/chantix_dual_action.jsp .
- 14.Masjedi MR, Azaripour A, Heydari G, Hosseini M. Effective factors on smoking cessation among the smokers in the first “Smoking Cessation Clinic” in Iran. Tanaffos J Respir Dis. 2002;1:61–7. [Google Scholar]
- 15.Heydari G, Milani HS, Hosseini M, Masjedi MR. The effect of training and behavioral therapy recommendations on smoking cessation. Tanaffos J Respir Dis. 2003;2:39–44. [Google Scholar]
- 16.Heydari G, Jianfar G, Alvanpour A, Hesami Z, Talischi F, Masjedi MR. Efficacy of telephone quit line for smokers: 12 months follow up results. Tannafos J Respir Dis. 2011;10:42–8. [PMC free article] [PubMed] [Google Scholar]
- 17.Heydari G, Marashian M, Ebn Ahmady A, Masjedi M, Lando HA. Which form of nicotine replacement therapy is more effective for quitting smoking? A study in Tehran, Islamic Republic of Iran. East Mediterr Health J. 2012;18:1005–10. doi: 10.26719/2012.18.10.1005. [DOI] [PubMed] [Google Scholar]
- 18.Lucan SC, Katz DL. Factors associated with smoking cessation counseling at clinical encounters: The Behavioral Risk Factor Surveillance System (BRFSS) 2000. Am J Health Promot. 2006;21:16–23. doi: 10.4278/0890-1171-21.1.16. [DOI] [PubMed] [Google Scholar]
- 19.Centers for Disease Control and Prevention (CDC). Quitting smoking among adults – United States, 2001-2010. MMWR Morb Mortal Wkly Rep. 2011;60:1513–9. [PubMed] [Google Scholar]
- 20.Hass B, Pooley J, Feuring M, Suvarna V, Harrington AE. Health technology assessment and its role in the future development of the Indian healthcare sector. Perspect Clin Res. 2012;3:66–72. doi: 10.4103/2229-3485.96449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Heydari G, Talischi F, Tafti SF, Masjedi MR. Quitting smoking with varenicline: Parallel, randomised efficacy trial in Iran. Int J Tuberc Lung Dis. 2012;16:268–72. doi: 10.5588/ijtld.11.0183. [DOI] [PubMed] [Google Scholar]
- 22.Hu P, Chang C. Taiwan Smokers’ Helpline. Paper Presented at: 2011 Asian Pacific Quit Line Workshop; 7-8. June, Goyang, Republic of Korea. 2011 [Google Scholar]
- 23.Yunibhand J. Thailand Report on Quit Line Activities. Paper Presented at: 2011 Asian Pacific Quit Line Workshop; 7-8. June, Goyang, Republic of Korea. 2011 [Google Scholar]
- 24.Gilpin EA, Pierce JP. Demographic differences in patterns in the incidence of smoking cessation: United States 1950-1990. Ann Epidemiol. 2002;12:141–50. doi: 10.1016/s1047-2797(01)00266-6. [DOI] [PubMed] [Google Scholar]