

Abstract
Background
Globally, common psychiatric disorders such as depression and anxiety are among the leading causes of morbidity and mortality. The 12-item General Health Questionnaire (GHQ-12) is a widely used questionnaire for screening or detecting common psychiatric disorders. The purpose of this study was to examine the reliability, construct validity and factor structure of the GHQ-12 in a large sample of African, Asian and South American young adults.
Methods
A cross-sectional study was conducted among 9,077 undergraduate students from Chile, Ethiopia, Peru and Thailand. Students aged 18–35 years were invited to complete a self-administered questionnaire that collected information about lifestyle, demographics, and GHQ-12. In each country, the construct validity and factorial structures of the GHQ-12 questionnaire were tested through exploratory and confirmatory factor analyses (EFA and CFA).
Results
Overall the GHQ-12 items showed good internal consistency across all countries as reflected by the Cronbach's alpha: Chile (0.86), Ethiopia (0.83), Peru (0.85), and Thailand (0.82). Results from EFA showed that the GHQ-12 had a two-factor solution in Chile, Ethiopia and Thailand, although a three-factor solution was found in Peru. These findings were corroborated by CFA. Indicators of goodness of fit, comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean squared residual, were all in acceptable ranges across study sites. The CFI values for Chile, Ethiopia, Peru and Thailand were 0.964, 0.951, 0.949, and 0.931, respectively. The corresponding RMSEA values were 0.051, 0.050, 0.059, and 0.059.
Conclusion
Overall, we documented cross-cultural comparability of the GHQ-12 for assessing common psychiatric disorders such as symptoms of depressive and anxiety disorders among young adults. Although the GHQ-12 is typically used as single-factor questionnaire, the results of our EFA and CFA revealed the multi- dimensionality of the scale. Future studies are needed to further evaluate the specific cut points for assessing each component within the multiple factors.
Keywords: GHQ-12, factor structure, confirmatory factor analysis, exploratory factor analysis, common psychiatric disorders
Introduction
Most adults with common psychiatric disorders report their first symptoms before 24 years of age [1]. Data from the National Comorbidity Survey of US residents shows that approximately 50% of lifetime diagnosable psychiatric disorders begin by age 14, and that the proportion increases to 75% by age 24 years [2]. These data suggest that childhood, adolescence, and young adulthood periods are crucial in the development of psychiatric disorders. The most common psychiatric disorders include anxiety disorders and major depressive disorders [2]. Early adulthood is a time of heightened psychological vulnerability and onset of serious psychiatric disorders with adverse consequences not just during the transitional years but across the life course [3]. This increased recognition has led to the US Preventive Services Task Force's recommendation of screening adolescents for major depression to ensure early diagnosis and treatment [4]. In low-and middle-income countries (LAMICs) common psychiatric disorders are increasingly recognized as important public health problems, particularly among young adults [5]. Effective treatment of psychiatric disorders requires accurate detection and diagnosis [6] which in turn requires access to and systematic use of diagnostic instruments. In the last few decades, several brief questionnaires have been developed to assess common psychiatric disorders. The 12-item General Health Questionnaire (GHQ-12) originally developed in the UK [7] is one of the most widely used screening questionnaires to detect common psychiatric disorders including symptoms of anxiety and depressive disorders [8-11]. Several investigators have assessed the validity of the GHQ-12 among adults [7] including the World Health Organization multi-city study. Although the GQH-12 was originally designed for use in the adult population, numerous studies have used it in adolescent populations and educational settings due to its brevity; its internal consistency and stable factorial and construct validity [12]. However, no study has evaluated its cross-cultural validity and equivalence in young adults, particularly those in LAMICs. Therefore, we examined the reliability, construct validity and factor structure of the GHQ-12 in a large sample of African, Asian and South American young adults.
Methods and Materials
This multi-country survey of young adults was conducted among college students in four countries: Chile, Ethiopia, Peru and Thailand. Methodological details of the surveys and data collection procedures have been previously published [13-16]. In brief, flyers advertising the study were posted around college campuses. Students interested in participating in the study were invited to meet in a large classroom or auditorium where they were informed about the study and the opportunity to participate. Students consenting to participate were invited to complete a self-administered anonymous individual survey.
In total, 9,077 students aged ≥18 years of age from Chile (N=925), Ethiopia (N=2,645), Peru (N=2,538), and Thailand (N=2,969) participated in the study using a common research protocol. In each country, the questionnaires were translated from English into the local national lingua franca, following the World Health Organization (WHO) translation guidelines for assessment instruments which included a forward translation, targeted back-translation, and a review by a bilingual expert group [17]. Prior to the commencement of the study, ethical approvals were obtained from the following institutional review boards: Centro de Rehabilitación Club de Leones Cruz del Sur, Punta Arenas, Chile; Addis Continental Institute of Public Health, Haramaya University and Gondar University, Ethiopia; Dos de Mayo Hospital and Universidad Nacional Mayor de San Marcos in Lima, Peru; Faculty of Medicine Chulalongkorn University, Walailak University, Thailand, and the University of Washington, USA. The Harvard T.H. Chan School of Public Health Office of Human Research Administration, USA, granted approval to use the anonymised datasets for analysis.
Data collection and variables
As noted above, a self-administered questionnaire was used to collect information in this study. Socio-demographic information collected included age, sex, and year in the university. Lifestyle information included smoking, alcohol use, energy drink and caffeinated beverage use, and physical activity. The questionnaire also included the GHQ-12 instrument for assessment of common psychiatric disorders. After the survey administration, trained research nurses collected participants' anthropometric measurements including height, weight, waist and hip circumference, using protocol established by the WHO [18].
The General Health Questionnaire (GHQ-12)
The GHQ-12 has been commonly used worldwide for studies of various clinical and non-clinical populations [7, 8, 10, 19] to assess non-pathological common psychiatric disorders. The GHQ-12 asks respondents to report how they felt during the last four weeks on a range of symptoms including problems with sleep and appetite, subjective experiences of stress, tension, or sadness, mastering of daily problems, decision making and self-esteem. Response choices included: less than usual, no more than usual, more than usual and much more than usual. A score of 0 is given for the first two choices and 1 for the next two. The maximum possible score is 12 with higher scores suggesting higher mental distress. Typically those who score ≥5 on the GHQ-12 scale are considered as having common psychiatric disorders [8, 19].
Other covariates
Covariates collected include age (years), sex (male, female), cigarette smoking history (never, former, current), alcohol consumption (low: < 1 alcoholic beverage a week, moderate: 1–19 alcoholic beverages a week, and high to excessive consumption: ≥20 alcoholic beverages a week); body mass index (BMI) calculated as weight (in kilograms)/height squared (in square meters). BMI was categorized based on the WHO guidelines (underweight: <18.5 kg/m2, normal: 18.5–24.9 kg/m2, overweight: 25.0–29.9 kg/m2, and obese: ≥30 kg/m2) [18].
Statistical analyses
First, we examined the frequency distributions of socio-demographic, lifestyle characteristics of participants by country. These basic characteristics were summarized using means and standard deviations for continuous variables. We used counts and percentages for categorical variables. First, we evaluated reliability of GHQ-12 using internal consistency and item-total correlation indices. We used Cronbach's alpha as a measure of internal consistency and Spearman correlation as a measure of the direction and strength of item-total correlations. Next, we explored the factor structure of the GHQ-12 questionnaire using both exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) approaches. Prior to performing EFA, we assessed the suitability of the data for performing factor analysis. This analysis showed that it was appropriate to proceed with factor analysis (Bartlett's test of sphericity, p-value < 0.001 in all four countries; and the Kaiser-Meyer-Olkin measure of sampling adequacy, ranging from 0.886 to 0.910). We conducted the EFA using principal component analysis with orthogonal rotation. We used the scree plot, presenting eigenvalues associated with each factor, to determine factor structure. Factors with eigenvalues >1 were assumed to be meaningful and were retained for rotation. Rotated factor loadings of >0.4 were considered sufficient, while items with factor loadings ≥0.4 on more than one factor were considered cross-loading. To complement our EFA and to evaluate the model fit, we conducted CFA using maximum likelihood estimation approaches. In order to assess model fit, we calculated the Root Mean Square Error of Approximation (RMSEA) along with 95% confidence interval (95% CI), comparative fit index and Tucker-Lewis index to evaluate model fit. We used the following criteria recommended by Brown [20] to assess goodness of fit: (1) SRMR values ≤0.08; (2) RMSEA values ≤0.06 or below; (3) comparative fit index ≥0.95. Statistical analyses were performed using Stata version 12.0 software (Statacorp, College Station, TX). All p-values are two-sided and set to α=0.05.
Results
A summary of selected socio-demographic and lifestyle characteristics of study participants stratified by country is presented in Table 1. A total of 9,077 college students from four countries aged 18–35 years participated in the study. The majority of participants in Chile (70.5%), Peru (61.2%) and Thailand (66.8%) were females. In Ethiopia, only 22.9% of participants were female students. Heavy alcohol consumption (≥20 drinks/month was reported by 40.5% of students in Peru, 15.5% in Chile, 1.8% in Thailand, and 1.2% in Ethiopia. Current smoking was most prevalent in Chile (47.7%) and least prevalent in Ethiopia (3.1%). Consumption of any caffeinated beverages was reported by the majority of students in Ethiopia (80.1%), Peru (60.7%) and Thailand (58.1). In Chile 54.9% of students reported consumption of any caffeinated beverages.
Table 1. Demographic and lifestyle characteristics of college students by country.
| Chile N=925 | Ethiopia N=2645 | Peru N=2538 | Thailand N=2969 | Cramer's V | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | ||
| Age (years)* | 21.9 ±3.4 | 21.6±1.7 | 20.9±2.6 | 20.3±1.3 | |
| Age (years) | |||||
| 18-19 | 261 (28.3) | 138 (5.2) | 878 (34.6) | 862 (29.0) | 0.23 |
| 20 | 134 (14.5) | 545 (20.6) | 336 (13.2) | 849 (28.6) | |
| 21 | 111 (12.0) | 730 (27.6) | 405 (16.0) | 722 (24.3) | |
| 22 | 109 (11.8) | 487 (18.4) | 306 (12.1) | 386 (13.0) | |
| >23 | 307 (33.3) | 745 (28.2) | 613 (24.1) | 150 (5.0) | |
| Sex | |||||
| Male | 273 (29.5) | 2007 (77.1) | 985 (38.8) | 985 (33.2) | 0.40 |
| Female | 652 (70.5) | 596 (22.9) | 1553 (61.2) | 1984 (66.8) | |
| Body Mass Index (kg/m2)* | 24.9 ±4.4 | 19.2±1.7 | 23.5 ±4.4 | 21.6±3.8 | |
| Body Mass Index (kg/m2) | |||||
| Underweight (<18.5) | 10 (1.2) | 1026 (38.9) | 83 (4.3) | 491 (16.5) | 0.28 |
| Normal (18.5-24.9) | 431 (55.2) | 1576 (59.8) | 1282 (66.8) | 2046 (69.9) | |
| Overweight (25.0-29.9) | 218 (27.9) | 34 (1.3) | 471 (24.6) | 295 (9.9) | |
| Obese (≥30) | 122 (15.6) | 0 (0.0) | 82 (4.3) | 137 (4.6) | |
| Alcohol Consumption | |||||
| <1 drink/month | 407 (43.9) | 2269 (85.8) | 517 (20.4) | 2287 (77.0) | 0.12 |
| 1-19 drinks/month | 375 (40.5) | 343 (13.0) | 992 (39.1) | 630 (21.2) | |
| ≥20 drinks/month | 144 (15.5) | 33 (1.2) | 1029 (40.5) | 52 (1.8) | |
| Cigarette Smoking Status | |||||
| Never | 316 (42.3) | 2548 (96.3) | 1899 (74.8) | 2710 (91.3) | 0.30 |
| Former | 75 (10.0) | 15 (0.6) | 214 (8.4) | 55 (1.8) | |
| Current | 356 (47.7) | 82 (3.1) | 425 (16.8) | 204 (6.9) | |
| Consumption of Caffeinated Beverages | |||||
| No | 365 (45.1) | 525 (19.9) | 997 (39.3) | 1244 (41.9) | 0.30 |
| Yes | 433 (54.9) | 2111 (80.1) | 1541 (60.7) | 1725 (58.1) |
mean ± SD (standard deviation).
Numbers may not add up due to missing data for selected variable
As shown in Table 2, the GHQ-12 items showed good internal consistency across all countries as reflected by the high values of Cronbach's alpha: Chile (0.86), Ethiopia (0.83), Peru (0.85), and Thailand (0.82). The Spearman's correlation coefficients of the 12 questions of the GHQ and the GHQ-12 total score showed similar patterns in Chile and Peru with losing confidence and could not overcome difficulties having corrected item-total correlations greater than 0.70. In Ethiopia all items had corrected-item total correlations between 0.50 and 0.65. In Thailand able to concentrate (0.49) and lost much sleep (0.42) had the lowest corrected item-total correlations.
Table 2. Item-total correlations of GHQ-12 by country.
| Chile | Ethiopia | Peru | Thailand | |||||
|---|---|---|---|---|---|---|---|---|
| GHQ-12 Items | Corrected item-total correlation |
Alpha if item deleted |
Corrected item-total correlation |
Alpha if item deleted |
Corrected item-total correlation |
Alpha if item deleted |
Corrected item-total correlation |
Alpha if item deleted |
| 1. Able to concentrate | 0.63 | 0.73 | 0.56 | 0.73 | 0.60 | 0.73 | 0.49 | 0.73 |
| 2. Lost much sleep | 0.56 | 0.74 | 0.55 | 0.73 | 0.60 | 0.74 | 0.42 | 0.74 |
| 3. Playing useful part | 0.57 | 0.74 | 0.53 | 0.73 | 0.57 | 0.74 | 0.53 | 0.73 |
| 4. Capable of making decisions | 0.61 | 0.74 | 0.64 | 0.72 | 0.61 | 0.73 | 0.57 | 0.73 |
| 5. Under stress | 0.64 | 0.74 | 0.57 | 0.73 | 0.62 | 0.73 | 0.59 | 0.73 |
| 6. Could not overcome difficulties | 0.70 | 0.73 | 0.62 | 0.72 | 0.71 | 0.73 | 0.56 | 0.72 |
| 7. Enjoy day-to-day activities | 0.60 | 0.73 | 0.53 | 0.73 | 0.47 | 0.74 | 0.58 | 0.72 |
| 8. Face up to problems | 0.64 | 0.73 | 0.61 | 0.72 | 0.56 | 0.73 | 0.63 | 0.72 |
| 9. Feeling unhappy and depressed | 0.70 | 0.73 | 0.56 | 0.73 | 0.66 | 0.74 | 0.64 | 0.72 |
| 10. Losing confidence | 0.72 | 0.73 | 0.64 | 0.72 | 0.71 | 0.73 | 0.68 | 0.72 |
| 11. Thinking of self as worthless | 0.66 | 0.73 | 0.61 | 0.72 | 0.70 | 0.73 | 0.65 | 0.72 |
| 12. Feeling reasonably happy | 0.56 | 0.74 | 0.57 | 0.73 | 0.53 | 0.74 | 0.54 | 0.73 |
| Total GHQ-12 score* | 0.86 | 0.83 | 0.85 | 0.82 | ||||
Overall Cronbach's alpha
Through examination of eigenvalues, factor loadings and the scree plot for GHQ-12 items, a two-factor model was extracted for Chile, Ethiopia and Thailand (Table 3). However, a three-factor model provided a better fit for the data from Peru. In Ethiopia and Thailand the first factor (anxiety and depression) consisted of items 1, 2, 3, 4, 5 and 6; and the second factor (social dysfunction and depression) consisted of items 7, 8, 9, 10, 11, and 12. In Thailand, item 5 (felt constantly under pressure) cross-loaded on both factors. In Chile, the first factor (anxiety) included items 1, 4, 7, and 8. The rest of the items (2, 3, 5, 6, 9, 10, 11, and 12) loaded on the second factor (depression and social dysfunction) while item 6 (felt could not overcome difficulties) and item 10 (losing confidence) cross-loaded on both factors. In Peru the first factor (anxiety and depression) included similar items as in Ethiopia and Thailand (items 1, 2, 3, 4, 5, and 6). The second factor (social dysfunction) included items 9, 10, 11, and 12 while the third factor (depression) included items 7 and 8. Item 6 (felt could not overcome difficulties) cross-loaded on the first two factors.
Table 3. Exploratory Factor Analyses (EFA) for GHQ-12 by country.
| Chile | Ethiopia | Peru | Thailand | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 1 | Factor 2 | Factor 1 | Factor 2 | Factor 3 | Factor 1 | Factor 2 | |
| GHQ-12 Items | |||||||||
| 1. Able to concentrate | 0.25 | 0.64 | 0.18 | 0.62 | 0.65 | 0.11 | 0.25 | 0.11 | 0.63 |
| 2. Lost much sleep | 0.56 | 0.21 | 0.06 | 0.72 | 0.68 | 0.25 | 0.03 | 0.02 | 0.66 |
| 3. Playing useful part | 0.65 | 0.16 | 0.12 | 0.63 | 0.64 | 0.35 | -0.08 | 0.18 | 0.65 |
| 4. Capable of making decisions | 0.21 | 0.66 | 0.36 | 0.56 | 0.66 | 0.09 | 0.27 | 0.35 | 0.48 |
| 5. Under stress | 0.69 | 0.21 | 0.29 | 0.51 | 0.60 | 0.28 | 0.15 | 0.41 | 0.46 |
| 6. Could not overcome difficulties | 0.54 | 0.46 | 0.26 | 0.63 | 0.59 | 0.41 | 0.19 | 0.34 | 0.52 |
| 7. Enjoy day-to-day activities | 0.12 | 0.75 | 0.68 | 0.04 | 0.08 | 0.09 | 0.78 | 0.63 | 0.06 |
| 8. Face up to problems | 0.16 | 0.77 | 0.72 | 0.13 | 0.15 | 0.21 | 0.72 | 0.72 | 0.06 |
| 9. Feeling unhappy and depressed | 0.59 | 0.39 | 0.52 | 0.26 | 0.17 | 0.61 | 0.40 | 0.71 | 0.14 |
| 10. Losing confidence | 0.59 | 0.42 | 0.64 | 0.28 | 0.20 | 0.72 | 0.33 | 0.75 | 0.17 |
| 11. Thinking of self as worthless | 0.76 | 0.16 | 0.64 | 0.23 | 0.24 | 0.75 | 0.20 | 0.63 | 0.27 |
| 12. Feeling reasonably happy | 0.71 | 0.08 | 0.59 | 0.22 | 0.17 | 0.77 | -0.12 | 0.54 | 0.23 |
As shown in Figure 1, results from CFA corroborated the EFA findings showing a three-factor solution in Peru and a two-factor solution in Chile, Ethiopia and Thailand. Indicators of goodness of fit, comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean squared residual were all in acceptable ranges across study sites (Table 4). The CFI values for Chile, Ethiopia, Peru and Thailand were 0.964, 0.951, 0.949, and 0.931, respectively. The corresponding RMSEA values were 0.051, 0.050, 0.059, and 0.059. In Ethiopia enjoying day-to-day activities and facing problems were associated with an approximate correlation of 0.26. We re-examined the model, allowing for these two items to be correlated with each other, which improved the fit (CFI=0.951 and RMSEA=0.050). In Chile thinking of self as worthless and feeling reasonably happy were correlated with an approximate correlation of 0.34. We re-examined the model, allowing for these two items to be correlated with each other, which improved the fit (CFI=0.964 and RMSEA=0.051).
Figure 1. Confirmatory Factor Analysis (CFA) for GHQ-12 by country.
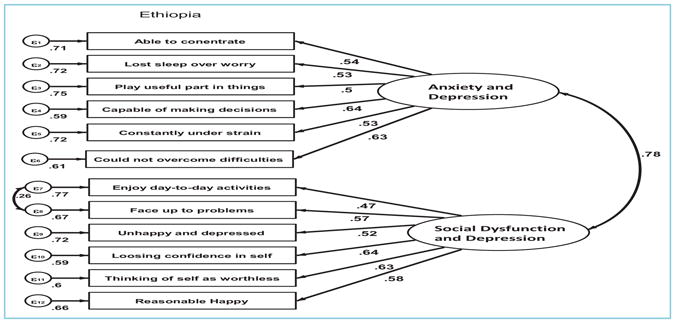
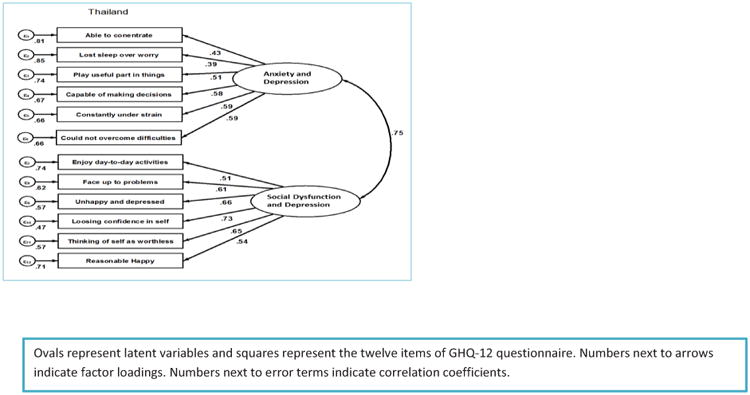
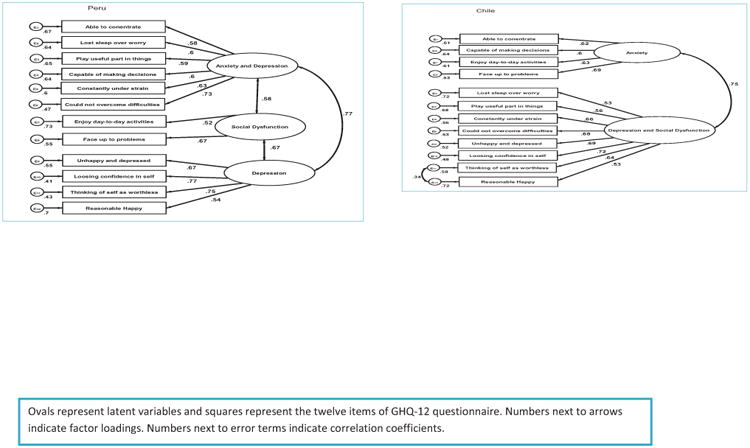
Table 4. Goodness-of-fit indexes for GHQ-12 by county.
| Chile | Ethiopia | Peru | Thailand | |
|---|---|---|---|---|
| RMSEA | 0.051 | 0.050 | 0.059 | 0.059 |
| SRMR | 0.032 | 0.029 | 0.032 | 0.035 |
| CFI | 0.964 | 0.951 | 0.949 | 0.931 |
| TLI | 0.955 | 0.938 | 0.934 | 0.914 |
RMSEA: Root mean squared error of approximation; SRMR: Standardized root mean squared residual; CFI: Comparative fit index; TLI: Tucker-Lewis index
Discussion
We evaluated the reliability, construct validity, and factor structure of the GHQ-12 in a large diverse sample of young adults. Overall our study results showed cross-cultural measurement equivalence and adequate psychometric properties regarding reliability and construct validity of GHQ-12 in four countries. Our findings are consistent with prior studies that reported good reliability [11, 12, 21] and multi- dimensionality [12, 21, 22] of the GHQ-12 questionnaire.
Although the total score of GHQ-12 is typically used to identify common psychiatric disorders, it was originally designed to identify two classes of phenomena: (i) inability to carry out one's normal healthy functions and (ii) emergence of new phenomena that are distressing [12, 23]. The results of our EFA and CFA revealed two-factor models in Chile, Ethiopia and Thailand consistent with findings of prior studies [12, 21, 22] and the original design of the questionnaire [12, 23]. The WHO multi-city study of psychological disorders in general medical practice was the first large-scale attempt at evaluating the factor structure of the GHQ-12. Using EFA procedures, the investigators noted the stability of the factor structure of the GHQ-12 with two factors extracted in 10 cities (Ankara, Bangalore, Berlin, Groningen, Manchester, Nagasaki, Paris, Santiago de Chile and Seattle) and three factors in 5 cities (Athens, Ibadan, Rio de Janeiro, Shanghai, and Verona) [12]. Subsequently several investigators have documented a two-factor model for GHQ-12. For instance, in their study of 18-year-old males in Italy Politi et al found that two factors defined by 7 items related to anxiety and depression (items 2,5,6,9,10,11 and 12) and 6-items related to social dysfunction (items 1,3,4,7,8 and 12). One item (item 12-feeling reasonably happy) cross-loaded on the two factors [21]. In their study of young adults (age 18-25) in Iran Montazeri et al found two-factors where the first factor represented psychological distress (including items 1,3,4,7,8,10 and 11) while the second factor represented social dysfunction (with items 2,5,6,7,9 and 12) [22]. These observations were further reinforced by other investigators who reported a two-factor model of the GHQ-12 [24, 25]. Our observation of a better fit with a three-factor model among Peruvians, is similar to what was proposed by Graetz [26]. The authors proposed a three-factor structure consisting of anxiety and depression (items, 2, 5, 6, and 9), anhedonia and social dysfunction (items 1, 3, 4, 7, 8, and 12) and loss of confidence or self-esteem (items 10 and 11) [26]. Similarly, Pardon et al, in their study of adolescents in Spain, reported a three-factor structure for the GHQ-12 [11]. Overall, our study results showing two dominant factors depression/anxiety and social dysfunction across the four countries (with the possibility of a third factor in Peru) suggest strong construct validity and stability of the GHQ-12 when used in multi-national settings.
Strengths of the current study include a relatively large sample size and diverse group of participants. Nevertheless, some limitations may have an impact on the interpretation of our results. Criterion validity utilizing diagnostic gold standard and test-retest reliability using repeated measures were not assessed. However, the criterion validity of GHQ-12 has been previously shown to be appropriate when compared with clinician administered diagnostic methods [7]. In addition, our study was restricted to young men and women enrolled in colleges or university. Hence, readers should exercise caution when generalizing results from the present study to general populations with lower levels of educational attainment.
In conclusion, this was the first large-scale cross-cultural study of GHQ-12 in young adults. Despite some variations in factor structure, social, geographic, racial and ethnic differences of populations studied to date, our study and those of others confirm the utility of the GHQ-12 in assessing common psychiatric disorders such as symptoms of anxiety and depressive disorders. Future studies are needed to further evaluate the specific cut points for assessing each component within the multiple factors. Our results may help inform future research seeking to identify risk factors associated with anxiety and depressive disorders in young adults in LAMICS. They may also facilitate the design and deployment of intervention programs targeted to preventing anxiety and depressive disorders.
Highlights.
This was the first large-scale cross-cultural study of general health questionnaire (GHQ-12) validation in young adults
The study showed cross-cultural measurement equivalence and adequate psychometric properties regarding reliability and construct validity of GHQ-12 in four countries.
Our results may help inform future research seeking to identify risk factors associated with common psychiatric disorders in young adults in low- and middle income countries.
Acknowledgments
This work was supported by an award from the National Institutes of Health, National Institute of Minority Health and Health Disparities (T37-MD001449). The authors wish to thank the participating universities for supporting the conduct of this study
Footnotes
Competing Interests: None to declare
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Patton GC, Coffey C, Romaniuk H, Mackinnon A, Carlin JB, Degenhardt L, Olsson CA, Moran P. The prognosis of common mental disorders in adolescents: a 14-year prospective cohort study. Lancet. 2014;383(9926):1404–1411. doi: 10.1016/S0140-6736(13)62116-9. [DOI] [PubMed] [Google Scholar]
- 2.Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593–602. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- 3.IOM. Investing in the Health and Well-Being of Young Adults. Washington, DC: The National Academies Press; 2015. [PubMed] [Google Scholar]
- 4.Thombs BD, Roseman M, Kloda LA. Depression screening and mental health outcomes in children and adolescents: a systematic review protocol. Syst Rev. 2012;1:58. doi: 10.1186/2046-4053-1-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Evans DL, Charney DS. Mood disorders and medical illness: a major public health problem. Biological Psychiatry. 2003;54(3):177–180. doi: 10.1016/s0006-3223(03)00639-5. [DOI] [PubMed] [Google Scholar]
- 6.Liu SI, Yeh ZT, Huang HC, Sun FJ, Tjung JJ, Hwang LC, Shih YH, Yeh AW. Validation of Patient Health Questionnaire for depression screening among primary care patients in Taiwan. Compr Psychiatry. 2011;52(1):96–101. doi: 10.1016/j.comppsych.2010.04.013. [DOI] [PubMed] [Google Scholar]
- 7.Goldberg DP, Gater R, Sartorius N, Ustun TB, Piccinelli M, Gureje O, Rutter C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med. 1997;27:6. doi: 10.1017/s0033291796004242. [DOI] [PubMed] [Google Scholar]
- 8.Patel V, Araya R, Chowdhary N, King M, Kirkwood B, Nayak S, Simon G, Weiss HA. Detecting common mental disorders in primary care in India: a comparison of five screening questionnaires. Psychological Medicine. 2008;38(2):221–228. doi: 10.1017/S0033291707002334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Araya R, Wynn R, Lewis G. Comparison of two self administered psychiatric questionnaires (GHQ-12 and SRQ-20) in primary care in Chile. Social Psychiatry and Psychiatric Epidemiology. 1992;27(4):168–173. doi: 10.1007/BF00789001. [DOI] [PubMed] [Google Scholar]
- 10.Abubakar A, Fischer R. The factor structure of the 12-item General Health Questionnaire in a literate Kenyan population. Stress Health. 2012;28(3):248–254. doi: 10.1002/smi.1420. [DOI] [PubMed] [Google Scholar]
- 11.Padron A, Galan I, Durban M, Gandarillas A, Rodriguez-Artalejo F. Confirmatory factor analysis of the General Health Questionnaire (GHQ-12) in Spanish adolescents. Qual Life Res. 2012;21(7):1291–1298. doi: 10.1007/s11136-011-0038-x. [DOI] [PubMed] [Google Scholar]
- 12.Werneke U, Goldberg DP, Yalcin I, Ustun BT. The stability of the factor structure of the General Health Questionnaire. Psychol Med. 2000;30(4):823–829. doi: 10.1017/s0033291799002287. [DOI] [PubMed] [Google Scholar]
- 13.Velez JC, Souza A, Traslavina S, Barbosa C, Wosu A, Andrade A, Frye M, Fitzpatrick AL, Gelaye B, Williams MA. The Epidemiology of sleep quality and consumption of stimulant beverages among Patagonian Chilean college students. Sleep Disord. 2013;2013:910104. doi: 10.1155/2013/910104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lemma S, Patel SV, Tarekegn YA, Tadesse MG, Berhane Y, Gelaye B, Williams MA. The Epidemiology of Sleep Quality, Sleep Patterns, Consumption of Caffeinated Beverages, and Khat Use among Ethiopian College Students. Sleep Disord. 2012;2012:583510. doi: 10.1155/2012/583510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lohsoonthorn V, Khidir H, Casillas G, Lertmaharit S, Tadesse MG, Pensuksan WC, Rattananupong T, Gelaye B, Williams MA. Sleep quality and sleep patterns in relation to consumption of energy drinks, caffeinated beverages, and other stimulants among Thai college students. Sleep Breath. 2013;17(3):1017–1028. doi: 10.1007/s11325-012-0792-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sanchez S, Martinez C, Oriol R, Yanez D, Castaneda B, Sanchez E, Gelaye B, Williams M. Sleep quality, sleep patterns and consumption of energy drinks and other caffeinated beverages among Peruvian college students. Health. 2013;5(8A2):26–35. doi: 10.4236/health.2013.58A2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.WHO: World Health Organization. [Accessed on August 17, 2015];Process of translation and adaptation of instruments. Availabale at: http://www.who.int/substance_abuse/research_tools/translation/en.
- 18.WHO. Report of a WHO Expert Committee. World Health Organizations; Geneva: 1995. Physical status: the use and interpretation of anthropometry. [PubMed] [Google Scholar]
- 19.Fernandes AC, Hayes RD, Patel V. Abuse and other correlates of common mental disorders in youth: a cross-sectional study in Goa, India. Social Psychiatry and Psychiatric Epidemiology. 2013;48(4):515–523. doi: 10.1007/s00127-012-0614-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Brown TA. Confirmatory Factor Analysis for Applied Research. Guilford Press; 2006. [Google Scholar]
- 21.Politi PL, Piccinelli M, Wilkinson G. Reliability, validity and factor structure of the 12-item General Health Questionnaire among young males in Italy. Acta Psychiatr Scand. 1994;90(6):432–437. doi: 10.1111/j.1600-0447.1994.tb01620.x. [DOI] [PubMed] [Google Scholar]
- 22.Montazeri A, Harirchi AM, Shariati M, Garmaroudi G, Ebadi M, Fateh A. The 12-item General Health Questionnaire (GHQ-12): translation and validation study of the Iranian version. Health Qual Life Outcomes. 2003;1:66. doi: 10.1186/1477-7525-1-66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Goldberg DP, Gater R, Sartorius N, Ustun TB, Piccinelli M, Gureje O, Rutter C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychological Medicine. 1997;27(1):191–197. doi: 10.1017/s0033291796004242. [DOI] [PubMed] [Google Scholar]
- 24.Toyabe S, Shioiri T, Kobayashi K, Kuwabara H, Koizumi M, Endo T, Ito M, Honma H, Fukushima N, Someya T, et al. Factor structure of the General Health Questionnaire (GHQ-12) in subjects who had suffered from the 2004 Niigata-Chuetsu Earthquake in Japan: a community-based study. BMC Public Health. 2007;7:175. doi: 10.1186/1471-2458-7-175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Li WH, Chung JO, Chui MM, Chan PS. Factorial structure of the Chinese version of the 12-item General Health Questionnaire in adolescents. J Clin Nurs. 2009;18(23):3253–3261. doi: 10.1111/j.1365-2702.2009.02905.x. [DOI] [PubMed] [Google Scholar]
- 26.Graetz B. Multidimensional properties of the General Health Questionnaire. Soc Psychiatry Psychiatr Epidemiol. 1991;26(3):132–138. doi: 10.1007/BF00782952. [DOI] [PubMed] [Google Scholar]