

Abstract
Background. Influenza and pneumococcal vaccinations are recommended for elderly and high-risk patients; however, rates of adherence are low. We sought to implement influenza and pneumococcal vaccine initiatives in 4 different ambulatory specialty practices, using 3 unique approaches.
Methods. Four specialties with high-risk patient populations were selected for intervention: allergy (asthma), infectious disease (ID) (human immunodeficiency virus), pulmonary (chronic lung disease), and rheumatology (immunocompromised). Allergy and ID focused on influenza vaccination, and pulmonary and rheumatology focused on pneumococcal vaccination. We used 3 strategies for quality improvement: physician reminders, patient letters, and a nurse-driven model. Physicians were provided their performance data on a monthly basis and presented trended data on a quarterly basis at staff meetings.
Results. All 4 specialties developed processes for improving vaccination rates with all showing some increase. Higher rates were achieved with pneumococcal vaccine than influenza. Pneumococcal vaccine rates showed steady improvement from year to year while influenza vaccine rates remained relatively constant. Allergy's influenza rate was 59% in 2011 and 64% in the 2014 flu season. Infectious disease influenza rates moved from 74% in the 2011 flu season to 86% for the 2014 season. Pneumococcal vaccine in pulmonary patients' rate was 52% at the start of intervention in February 2009 and 79% as of January 2015. Rheumatology rates rose from 50% in February 2009 to 87% in January 2015.
Conclusions. Integrated routine workflow and performance data sharing can effectively engage specialists and staff in vaccine adherence improvement. Influenza vaccination may require other approaches to achieve the rates seen with pneumococcal vaccine.
Keywords: improvement, influenza, pneumococcal, quality, vaccines
Quality improvement has become an important aspect of the routine work in healthcare, allowing physicians and staff to understand their current practices, then develop new processes to achieve an end goal. Increasing adherence to guideline-based recommendations on vaccinations has remained a challenge for decades. At our institution, the Department of Medicine has established a Quality Program (DOMQP) to work with all clinical divisions to create clinical quality metrics using billing and electronic medical record (EMR) data and to formulate performance improvement plans [1]. One clear focus of the DOMQP over the past few years has been to improve vaccination rates for influenza and pneumococcal disease across several of our divisions.
Influenza is associated with substantial morbidity and mortality each year in the United States. Since 2010, the Advisory Committee on Immunization Practices has recommended that all persons aged ≥6 months be vaccinated against influenza each year [2]. Likewise, pneumococcal disease is a leading cause of vaccine-preventable illness and death. Thus, vaccination remains a priority for adults older than age 65 years and at-risk patients, such as those with chronic disease, with compromised or altered immune systems resulting from disease, smokers, and nursing home residents [3–5].
Given the clear guideline recommendations supporting the use of influenza and pneumococcal vaccination for specific patient populations, the DOMQP worked with 4 clinical divisions, Allergy, Infectious Diseases, Pulmonary, and Rheumatology, to promote adherence to guidelines for vaccination. We worked to implement 3 improvement strategies—patient reminders, physician reminders, and a nurse-driven model—with the goal of measuring and then increasing vaccination rates. Our process improvement work was guided by 4 key principles: (1) reinforcing patient education and screening, (2) documenting vaccines in a coded section of the EMR for ease of measurement, (3) incorporating nonphysician clinic staff into workflow, and (4) sharing data on vaccination rates routinely to physicians and office staff so that the quality improvement work remained a division priority.
METHODS
Department of Medicine Quality Program Infrastructure
The DOMQP comprises a 1.0 FTE Project Coordinator (K.N.P.), a 0.5 FTE Program Manager (L.E.S.-G.), and a 0.35 FTE Medical Director (S.P.D.), with oversight and direction provided by a Department of Medicine (DOM) Vice Chair (J.C.). There is a 0.10–0.15 FTE Information Systems (IS) resource allocated for quality report development and coding. The purpose of the DOMQP is to work with all divisions within the DOM to measure, report, and improve on quality metrics and projects.
Quality Metric Measurement and Report Development
Through the work of a designated IS person, we leveraged our EMR and automated data retrieval system to develop clinical quality metric reports using billing and EMR data. We worked closely with division leadership to create tailored quality metrics that were unique to the patient population of the divisions and which reflected the specialty care provided. This process took several years, and various quality control checks were performed to ensure data integrity so that the quality metric accurately reflected multiple facets of care provided. Once a master report of patients was created, quality checked, and approved, the data were then used to create additional reports: a summary of the division performance and a provider level summary.
Denominator
A combination of administrative data (diagnosis and billing codes) and EMR clinical data (history of allergy to pneumococcal or influenza vaccination, and medications) was acquired from our hospital's IS. We used these data to determine which patients were eligible for the metrics. Within each division, patients were included in the quality metric if they met visit and diagnosis criteria. The visit criterion was 2 visits in the last 24 months meeting one of the following criteria: (1) at least 1 visit had to have occurred within the first 12 months, and at least 1 visit within the second 12 months; or (2) for patients with visits only during the second 12 months, the first and last visits had to be separated by a minimum of 90 days. These thresholds were developed to ensure that the study population included patients who were regularly seen in the ambulatory practices, as opposed to those seen only at a single consultation visit. The diagnosis criteria for the 4 divisions were as follows: (1) Allergy, patients with asthma; (2) Infectious Diseases, patients with human immunodeficiency virus (HIV); (3) Pulmonary, patients with chronic lung disease; and (4) Rheumatology, patients on immunosuppressive medications. Across all populations, patients who had an allergy or an adverse reaction to vaccination, as documented in a coded field of the EMR, were excluded from the population. These patients were not followed by the metric so the proportion they represent in their respective populations is not known. The total number of patients eligible and the type of patients included in each division are outlined in Table 1.
Table 1.
Patient Populations and Vaccine Strategies for 4 Divisions
| Division | Patient Population | No. of Patients | Vaccine | Vaccine Strategy | No. of Physicians | Percentage Point Increase From Baseline | No. of Patients With Documented Refusal |
|---|---|---|---|---|---|---|---|
| Allergy | Patients with Asthma (Age 13+) | 1142 | Influenza | Nurse-Driven Model | 15 | 5 (Four-Year measurement period) | 85 |
| Infectious Disease* | Adults with HIV (Age 18+) | 659 | Influenza | Screening Sheet and Point of Care Reminder | 19 | 11 (Four-Year measurement period) | 40 |
| Pulmonary | Patients with Chronic Lung Disease (Age 17+) | 2483 | Pneumococcal | Patient Letters in advance of appointment |
27 | 27 (Six-Year measurement period) | 18 |
| Rheumatology | Immunosuppressed Patients (Age 18+) | 2898 | Pneumococcal | Physician Reminders | 35 | 37 (Six-Year measurement period) | 37 |
Abbreviations: HIV, human immunodeficiency virus.
* This division's denominator is determined by the number of established HIV patients they have at the start of the flu season and stays constant throughout.
Numerator for Influenza and Pneumococcal Vaccination
The proportion of patients in the 4 ambulatory divisions who were up-to-date with either vaccination was defined according to the Centers for Disease Control and Prevention (CDC) guidelines. The vaccination status of each patient was determined through documentation in structured data fields of the patient's EMR, in the immunization or health maintenance monitoring fields. This was not just limited to documentation of an administered vaccine but also documentation of a patient decline, receipt of vaccine elsewhere, a deferral, or unavailability of vaccine. Any documented vaccination status would count. For the pneumococcal vaccine, from July 2009–2013, only Pneumovax was counted as meeting the metric. From August 2013 to present, either Pneumovax or Prevnar were counted as meeting the metric, to reflect the updated CDC guidelines. Only patients without any documentation in a coded field were counted as not meeting the metric. Thus, physicians would be given credit for the task of asking a patient to get vaccinated and documenting that the patient declined the vaccine or documenting the vaccine was administered elsewhere (see Figure 1). If the vaccination was documented only in the text of the physician's note, however, this was not included in the outcome—physicians and staff were encouraged to document their actions in a coded section of the EMR from which our IT team could pull the data easily and without the need for manual chart review.
Figure 1.

Vaccination structured fields in electronic medical record (EMR). Example of the module within the EMR for staff and clinicians to document vaccination status as a coded data element to be captured by reporting tools.
Interventions
Nurse Driven Model
Patients' screening for vaccine eligibility, administration and/or documentation handled completely by nursing staff.
Patient Letters
Screening sheet for vaccine sent to patient via postal mail before patients' upcoming visits.
Physician Reminders
Screening sheet combined with vaccination order form to alert physician to have vaccine discussion and order vaccine when appropriate.
Allergy
An influenza vaccine standing order form was made available through the hospital for the division. During flu season, every patient that came to the clinic was asked to complete a screening sheet and offered a flu shot during their visit. Vaccinations were administered and documented by the nursing staff. The improvement strategy was highlighted by DOMQP members at regular faculty meetings and physicians could track the rates of their asthma patients in the EMR.
Infectious Disease
Physicians were re-educated about the appropriateness of flu vaccine among the HIV population. In addition, administrative staff implemented the use of a patient screening sheet which was given to patients at the front desk upon check in to their visit. Patients could then comment on whether they had received a flu vaccine elsewhere or wanted one during that visit. The nursing workflow was changed to incorporate waiting room time as opportunity for vaccine discussion with the patient. If a patient's yearly visit did not fall within the flu season, the nursing/social work team contacted patients via telephone to document in the EMR if they had received a vaccine elsewhere.
Pulmonary
An EMR report was created to automatically generate a list of patients captured in the intervention denominator that were scheduled for a visit in the upcoming 6 weeks. Letters were then sent to patients asking them to bring documentation of, or proof of eligibility for pneumococcal vaccine to their visit. An additional report identified patients in the population on the daily clinic schedules as a second reminder of the importance of the vaccine. Administrative staff implemented a point of care reminder for the physician to have a discussion about pneumococcal vaccination and then document the vaccine status in the appropriate field.
Rheumatology
A checklist was posted on clinic room walls to remind physicians to vaccinate before prescribing immunosuppressive medications. An EMR report was developed from which point-of-care paper reminder forms were generated for patients who had routine clinic visits and were overdue for their pneumococcal vaccine (Figure 2). These reminders were printed and stapled to the billing sheet by administrative staff so that physicians could have a conversation with the patient about vaccination, document prior vaccination in a coded section of the EMR, or order the vaccine to be administered by the nurse on the same day as the visit [6].
Figure 2.

Physician reminder is illustrated. Automatically generated by EMR for patients identified as meeting vaccination criteria. Included in patient chart by front desk staff to provide a physical reminder of vaccination for clinical staff.
Communication Strategy
We worked directly with a clinical champion in each division whose role it was to coordinate the process improvement within the practice. We shared performance data with frontline staff using 2 methods – monthly emails to division leadership (practice manager, division administrator, division chief, and clinical director) and quarterly presentations by the DOMQP at division staff meetings.
The monthly email showed trended data over time, the division performance and individual provider-level data which could be shared with physicians and staff. In some divisions, comparative data on provider-level performance was sent via email in a blinded fashion among all clinical staff. In other divisions, individual provider-level data was shared in an unblinded fashion to spur further increases in performance by providers whose data lagged behind their peers.
During quarterly presentations we described the metric, reviewed performance data, and assessed process improvement efforts within the practices. Staff were encouraged to share any challenges and successes with the entire group in an effort to keep the process streamlined and to address areas where additional process changes might be needed. Questions were answered and the electronic metrics were adjusted over time to make them clinically relevant for clinicians.
RESULTS
During the QI initiative, we saw improvements in both pneumococcal and influenza vaccination rates (Figures 3 and 4). Pneumococcal vaccine rates in pulmonary patients moved from 52% at the start of intervention in February 2009 to 79% as of January 2015. Rheumatology's rate rose from 50% in February 2009 to 87% in January 2015. Allergy influenza rates went from 59% in 2011 to 64% in the 2014 flu season. ID influenza rates saw improvement from 74% in the 2011 flu season to 86% for the 2014 season. For pneumococcal vaccination in Rheumatology, we have previously shown that our intervention had an impact on our vaccination rates through an interrupted time-series analysis [7, 8]. In the Pulmonary practice, there was a small increase in the vaccination rates present before the start of the QI intervention. However, the rate of change (slope) of the pneumococcal vaccination rate appeared to increase more sharply after the patient reminder letter intervention in mid-2011 and then plateaued approximately 80% approximately 2 years later.
Figure 3.
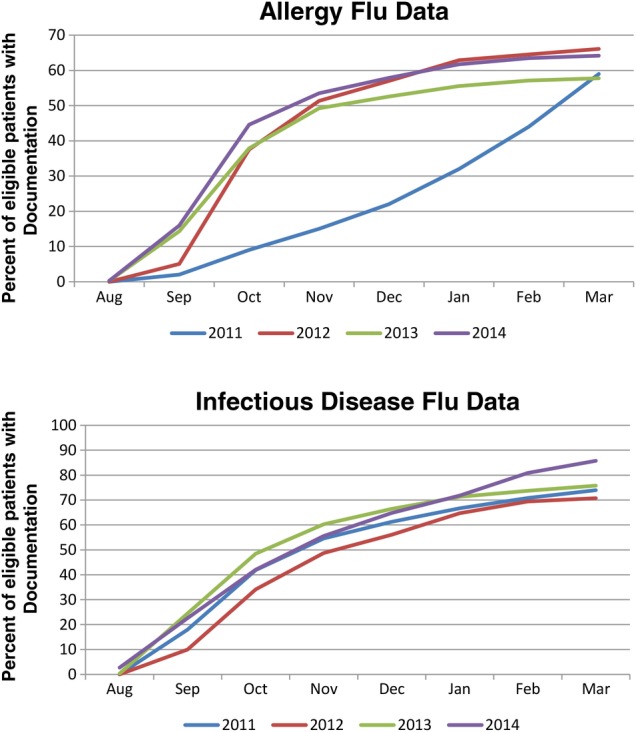
Influenza vaccination rates are shown. (Top) Trended performance data of allergy division asthma patient influenza vaccination rates over 3 flu seasons (2011–2014). (Bottom) Trended performance data of infectious disease division human immunodeficiency virus (HIV) patient influenza vaccination rates over 3 flu seasons (2011–2014). *The interventions in both specialties began in 2011 and remain unchanged.
Figure 4.

Pneumococcal vaccination rates are shown. (Top) Trended performance data of the pulmonary division chronic lung disease pneumococcal vaccine rates from January 2009 through January 2015. Data include new Prevnar 13 documentation rates after it was implemented into workflow in August 2013. (Bottom) Trended performance data of rheumatology division pneumococcal vaccine rates among immunosuppressed rheumatology patients from December 2013 through January 2015. Data include new Prevnar 13 performance rates after it was implemented into workflow in September 2013.
Having metrics and improvement strategies built around the concerns and challenges of clinic staff and their populations led to ease of implementation because staff felt that their view of quality was being reflected in the measurement. Receiving credit for the work of discussion and documentation even when a patient still chose to decline was also helped clinic buy-in because they perceived it as a more accurate data capture of the workflow.
DISCUSSION
The DOMQP provides a unique opportunity for a dedicated quality measurement and improvement team to work closely with frontline specialty physicians and staff to routinely measure and improve quality on adherence to vaccine guidelines. We describe an approach to quality improvement for increasing pneumococcal and influenza vaccination rates, across 4 different divisions -Allergy, Infectious Diseases, Pulmonary, and Rheumatology. We were able to apply 3 distinct performance improvement strategies to yield positive results – physician reminders, patient letters and a nurse-driven model, despite variable number of physicians and unique staffing models in each of the 4 divisions. We learned quality improvement measures are more quickly adopted if the process is customizable and the data is reliable, thus creating tools and reports within the EMR to capture and relay information was paramount. However, it took time and much iteration of our data reports and quality improvement strategies to generate lasting results. For example, we linked our inpatient vaccination administration data with our outpatient vaccination data so that if patient were hospitalized and vaccinated, this would count toward an ambulatory provider meeting their vaccination quality metric.
In light of the Affordable Care Act and the change in the healthcare environment to now monitor and improve patient engagement and well as community health, quality measurement must be captured at 3 different levels: physician, facility and population. In addition, data collection infrastructures should have built-in data output that relays meaningful feedback to frontline staff [9]. We believe that much of our success was due to tailor made reporting and data captures that provides those 3 levels of detail. Team leads were able to discuss and strategize for improvement based on the overall rate of vaccination for the patient populations, rate variation by clinic location and by individual physician.
There are several barriers to ensuring patients are up-to-date with influenza and pneumococcal vaccination in the United States. Physicians may not be knowledgeable about adult vaccination recommendations due to a frequently changing evidence base and may not have practice guidelines readily available or accessible at the point of care. Documentation of vaccinations in the electronic medical record (EMR) may not occur given the increasing burden of clinical documentation for providers and staff. Patient factors include lack of patient awareness of vaccine availability and lack of understanding of the risks of contracting vaccine preventable diseases, particularly in the case of pneumococcal vaccine and its association with invasive pneumococcal disease [10]. Financial hurdles for patients may be cost or insurance coverage, whereas medical practices may face reimbursement issues. Lastly, as ambulatory practices have taken on more complex patients, and the time to care for chronic disease patients has diminished, operational issues within a practice may also limit their ability to vaccinate [11]. We previously reported that developing a routine process for electronic measurement of pneumococcal vaccination rates among immunocompromised rheumatology patients was an important first step in a quality improvement strategy [7]. We subsequently found a statistically significant improvement in pneumococcal vaccination among our immunocompromised rheumatology patients through the use of a point-of-care paper reminder form [8]. Modeling has suggested that programs utilizing standing order forms for both influenza and pneumococcal vaccination can be cost-effective as well [6]. However, the use of a form (neither standing order nor screening sheet) did not lead to an increase of overall performance rates with influenza.
A meta-analysis of approaches to enhance both influenza and pneumococcal vaccination among ambulatory adults found that patient outreach with personal contact and the use of non-physician personnel for vaccination were modestly succesful [12]. Another study of rheumatology outpatients demonstrated that both influenza and pneumococcal vaccination rates rose with the use of a reminder alert within the EMR, particularly within a practice where there was a nurse-driven process [13]. Immunosuppressed patients with inflammatory bowel disease were given a patient questionnaire paired with a nurse-driven vaccination program, which significantly increased both influenza and pneumococcal vaccination rates [14]. Within our clinics both Allergy and ID used a nurse driven model for influenza with varying results. Allergy clinic vaccination efforts seemed to shift the time of vaccination to earlier in the flu season (fall versus spring vaccination) without showing an increase in total documentation. ID showed a significant increase in documentation rates in the last measured season of intervention. There can be a stigma attached to influenza vaccine, possibly due to the fact that there is negative propaganda surrounding flu vaccine with many news outlets reporting that vaccines were ineffective for the strain of influenza that was actually in circulation the year they were administered. Also unlike most vaccines which are one time injections or a series of injections spread years apart flu is a yearly vaccine which may subliminally suggest that it is not of equal value to vaccines such and Pneumovax or Tetanus because immunity does not last as long.
A study among primary care practices in England, determined a few key success factors for increasing influenza vaccination: written performance reports, patient notification and systematic identification of patients eligible for vaccine [15]. Which raises the question: what is the best way to notify? An academic center conducted a randomized controlled trial of text messaging pregnant woman reminding them of the need for influenza vaccination, however this was not an effective approach [16]. Many other types of interventions have been attempted, with variable degrees of success. Some studies suggest that educational efforts generally do not show consistent or sustained impact while others have found that patient education is paramount in dispelling misconceptions about flu vaccination and that having an actual conversation with a physician has led to more vaccination than just merely offering vaccine in the ambulatory clinic setting. Most patients get their information on flu vaccine from media or casual conversations with family and friends. The latter of which are often misinformed or based on some sort of cultural bias [17–19]. Another contributing factor to influenza vaccination is the flu season itself. The flu season as defined by the CDC goes a lot longer than most people perceive the flu season to be. Our data shows that most vaccination occurs during the back-to-school rush of September and continues through January [20]. There is a decline in vaccination during February and March. Perhaps this is the manifestation of another misconception; where people associate the flu with the onset of colder temperatures and see no need for vaccination as Spring draws closer.
Our vaccination quality improvement efforts did have some limitations. Firstly, to prioritize an initiative, there must be continuous communication with divisions and engagement with busy frontline clinicians and staff. At a tertiary care academic referral center, there are multiple competing priorities organizationally. Thus we found that it was a challenge to maintain a high-priority on our vaccination efforts over time.
A second limitation is that since our data was solely electronic, and not based on manual chart review of the EMR, we may have had incomplete data on vaccination for patients who received care outside of our hospital and healthcare network. It was critical that our physicians and staff had discussions with patients about whether they had received the vaccine at a practice outside of our hospital and disconnected from our EMR. Only data elements correctly entered into the EMR could be gathered for analysis and reporting. This issue was particularly relevant for the influenza vaccination. Our rates of improvement for pneumococcal vaccination exceeded our influenza vaccination – we suspect that this is due to the wide availability of influenza vaccine at local chain pharmacies and other locations, thus having no documentation in the electronic health record used by our clinics. This lack of documentation of the influenza vaccines received outside of our institution may result in reports showing falsely lower rates of vaccination than actually exist in our populations. Inversely, the relative lack of ability to receive pneumococcal vaccines in the community ensures that patients utilize ambulatory office visits with their providers for this need. This limitation of the EMR and our healthcare setting is not unique and remains a challenge for outpatient practices that are not part of a true integrated health delivery system.
As the scientific evidence base continues to evolve, incorporating new guidelines into clinical practice will be important. For example, the CDC now recommends both the 13 valent pneumococcal conjugate vaccine (PCV13 Prevnar) and the 23-valent pneumococcal polysaccharide vaccine (PPSV23 Pneumovax) for immunosuppressed high-risk populations [9]. Interventions are now being put in place to ensure that those patients already vaccinated with PPSV23 now receive PCV13 and patients new to vaccination get a PCV13 and a follow appointment scheduled for PPSSV23 at the appropriate interval. In Pulmonary the patients targeted for PCV13 are those with interstitial lung disease, transplant patients and those over 65. In Rheumatology all patients within the Pneumovax denominator are targeted as they are all immunosuppressed. Our preliminary data shows that within our rheumatology practices, the PCV13 vaccination rate reached 53% within 17-months (September 2013–January 2015) (Figure 4).
CONCLUSIONS
In summary, the DOMQP was able to electronically measure and improve rates for influenza and pneumococcal vaccine across 4 different divisions using differing workflow strategies. Prior studies have focused on primary care and pediatrics, with less of a focus on medical specialties. We believe that for certain specialists who care for populations of chronic disease patients, such as HIV, asthma, chronic lung disease and immunosuppressed autoimmune conditions, taking ownership of adherence to current CDC guidelines for vaccinations is essential to improving the quality of care these patients receive. While the guidelines for influenza have not changed the messaging should. Disseminating clear and accurate information regarding the need for and efficacy of influenza vaccine through media and within clinic settings should be an increased priority [19]. Future studies may evaluate the use of similar quality improvement strategies across other chronic disease populations.
Acknowledgments
Special thanks to the faculty and support staff of the Brigham and Women's Hospital ambulatory specialty practices and the Department of Medicine administrative leadership team for their guidance and support.
Potential conflicts of interest. All authors: No reported conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
References
- 1.Szent-Gyorgyi LE, Coblyn J, Turchin A et al. Building a departmental quality program: a patient-based and provider-led approach. Acad Med 2011; 86:314–20. [DOI] [PubMed] [Google Scholar]
- 2.Centers for Disease Control and Prevention. Influenza (Flu); 2014. Available at: http://www.cdc.gov/flu/. Accessed April 1, 2015.
- 3.Centers for Disease Control and Prevention. Vaccines and Immunizations: Pneumococcal Vaccine; 2014. Available at: http://www.cdc.gov/vaccines/vpd-vac/pneumo/default.htm?s_cid=cs_797. Accessed April 1, 2015.
- 4.Mirsaeidi M, Ebrahimi G, Allen MB, Aliberti S. Pneumococcal vaccine and patients with pulmonary diseases. Am J Med 2014; 127:886.e1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vila-Corcoles A, Ochoa-Gondar O. Pneumococcal vaccination among adults with chronic respiratory diseases: a historical overview. Expert Rev Vaccines 2012; 11:221–36. [DOI] [PubMed] [Google Scholar]
- 6.Lin CJ, Zimmerman RK, Smith KJ. Cost-effectiveness of pneumococcal and influenza vaccination standing order programs. Am J Manag Care 2013; 19:e30–7. [PMC free article] [PubMed] [Google Scholar]
- 7.Desai SP, Turchin A, Szent-Gyorgyi LE et al. Routinely measuring and reporting pneumococcal vaccination among immunosuppressed rheumatology outpatients: the first step in improving quality. Rheumatology (Oxford) 2011; 50:366–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Desai SP, Lu B, Szent-Gyorgyi LE et al. Increasing pneumococcal vaccination for immunosuppressed patients: a cluster quality improvement trial. Arthritis Rheum 2013; 65:39–47. [DOI] [PubMed] [Google Scholar]
- 9.Conway PH, Mostashari F, Clancy C. The future of quality measurement for improvement and accountability. JAMA 2013; 309:2215–6. [DOI] [PubMed] [Google Scholar]
- 10.Lode H, Ludwig E, Kassianos G. Pneumococcal infection--low awareness as a potential barrier to vaccination: results of a European study. Adv Ther 2013; 30:387–405. [DOI] [PubMed] [Google Scholar]
- 11.Krishnarajah G, Carroll C, Priest J et al. Burden of vaccine-preventable disease in adult Medicaid and commercially insured populations: analysis of claims-based databases, 2006–2010. Hum Vaccin Immunother 2014; 10:2460–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lau D, Hu J, Majumdar SR et al. Interventions to improve influenza and pneumococcal vaccination rates among community-dwelling adults: a systematic review and meta-analysis. Ann Fam Med 2012; 10:538–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ledwich LJ, Harrington TM, Ayoub WT et al. Improved influenza and pneumococcal vaccination in rheumatology patients taking immunosuppressants using an electronic health record best practice alert. Arthritis Rheum 2009; 61:1505–10. [DOI] [PubMed] [Google Scholar]
- 14.Parker S, Chambers White L, Spangler C et al. A quality improvement project significantly increased the vaccination rate for immunosuppressed patients with IBD. Inflamm Bowel Dis 2013; 19:1809–14. [DOI] [PubMed] [Google Scholar]
- 15.Dexter LJ, Teare MD, Dexter M et al. Strategies to increase influenza vaccination rates: outcomes of a nationwide cross-sectional survey of UK general practice. BMJ Open 2012; 2:pii:e000851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Moniz MH, Hasley S, Meyn LA, Beigi RH. Improving influenza vaccination rates in pregnancy through text messaging: a randomized controlled trial. Obstet Gynecol 2013; 121:734–40. [DOI] [PubMed] [Google Scholar]
- 17.Lin L, Jung M, McCloud RF, Viswanath K. Media use and communication inequalities in a public health emergency: a case study of 2009–2010 pandemic influenza A virus subtype H1N1. Public Health Rep 2014; 129(Suppl 4):49–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Buyuktiryaki B, Soyer OU, Erkocoglu M et al. What a pandemic teaches us about vaccination attitudes of parents of children with asthma. Vaccine 2014; 32:2275–80. [DOI] [PubMed] [Google Scholar]
- 19.Frew PM, Painter JE, Hixson B et al. Factors mediating seasonal and influenza A (H1N1) vaccine acceptance among ethnically diverse populations in the urban south. Vaccine 2012; 30:4200–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Poland GA, Johnson DR. Increasing influenza vaccination rates: the need to vaccinate throughout the entire influenza season. Am J Med 2008; 121:S3–10. [DOI] [PubMed] [Google Scholar]