

Abstract
This article aims to cover post surgical trigeminal neuropathy and other conditions related to chronic trigeminal pain not specifically covered elsewhere in this series.
Is estimated to occur in 4–5% of patients overall, considerably less compared with other site surgeries.
Due to the high volume surgery undertaken in this region chronic post surgical pain remains common.
Relatively few clinicians are aware of this condition and as a result it is frequently poorly managed.
Introduction
Chronic orofacial pain syndromes represent a diagnostic challenge for any practitioner. Patients are frequently misdiagnosed or attribute their pain to a prior event such as a dental procedure, ENT problem or facial trauma. Psychological or psychiatric co-morbidities of depression and anxiety are prevalent in this population and compound the diagnostic conundrum. Treatment is less effective than in other pain syndromes, thus it often requires a multidisciplinary approach to address the many facets of this pain syndrome1.
Aetiology of orofacial pain
Facial pain can be associated with pathological conditions or disorders related to somatic and neurological structures2.
There are a wide range of causes of chronic orofacial pain and these have been divided into three broad categories:
musculoligamentous
dentoalveolar and
neurological and vascular1.
The commonest cause of chronic orofacial pain is temporomandibular disorders, principally myofascial in nature.
As mechanisms underlying these pains begin to be identified, more accurate classifications which are mechanism-based may come to be used. A major change has been that burning mouth syndrome probably has a neuropathic cause using the newly defined definitions rather than being a pain due to psychological causes.
Incidence
Chronic orofacial pain accounts for between 20 and 25% of chronic pain conditions2. A 6-month prevalence of facial pain has been reported by between 1% 2 and 2–3%3 of the population. In the study by Locker and Grushka, some pain or discomfort in the jaws, oral mucosa, or face had been experienced by less than 10% in the past 4 weeks4. In 1980, Bonica5 estimated that 5–7 million Americans suffer from chronic pain in the face and mouth, and between 25 and 45% are affected at some time of life. Most population-based studies have shown that women report more facial pain than men2 with rates approximately twice as high among women compared to men6. In clinic populations the rates for women are even higher1. On the other hand, other studies have found no sex difference in the prevalences of orofacial pain. Several studies have also shown variability in the prevalence across age groups. The age distribution of the facial pain population differs from that of the most usual pain conditions. In contrast to chest and back pain, for example, facial pain has been suggested to be less prevalent among older persons than younger ones. Conversely, in 1993 Lipton et al. found the prevalence of facial pain to remain relatively constant across the age groups2, while Riley and Gilbert3, no difference in prevalence was observed between the age groups of 45–64 years and older.
Diagnosis
The International Headache Society (IHS)7 has published diagnostic criteria for primary and secondary headaches as well as facial pain. Criteria have also been published by the International Association for the Study of Pain (IASP)8 and by the American Academy of Orofacial Pain (AAOP)9, and the Research Diagnostic Criteria for Temporomandibular Disorders10 covered elsewhere in this issue11. The impact of trigeminal pain must not be underestimated. Consequences include interruption of daily social functions such as eating, drinking, speaking, kissing, applying makeup, shaving and sleeping12. Burning mouth syndrome has been reported to cause significant psychological impact in 70% of patients. In temporomandibular joint (TMJ) pain, 29% of patients report a high level of disability resulting in unemployment. A recent validated tool, OHIP-14, has been developed for the assessment of disability related to oral function13.
Classification of orofacial pain
The aim of this section is to address the causes of chronic orofacial pain (lasting >3 months). However, the most common causes of acute dental pain are due to trauma or infection of the dental pulp which contains the nerves and vessels supplying the tooth14.
Chronic orofacial pain
The various suggested classifications of chronic orofacial pain do conflict with each other. Several classifications of chronic orofacial pain have been presented but this article will use the fourth classification (groups 1–3) as it presents a pragmatic and clinically useful alternative15.
Group 1
Neurovascular pain (predominantly in the 1st division of trigeminal (V) nerve)
The 1st division innervates the globe of the eye and the skin in the area above the eye and forehead. Migraine, Cluster headaches, Tension-type headaches, Medication overuse headaches and chronic daily headache will be covered separately in this review series.
Short-lasting unilateral neuralgiaform conjunctival irritation and tearing (SUNCT)
This is possibly a variation of the cluster tic syndrome. It is characterized by brief (15–120 seconds) bursts of pain in the eyes, temple, or face. The pain is usually unilateral and is described as burning, stabbing, or electric. It occurs frequently in a 24-hour period (>100 episodes). Neck movements can trigger the pain. SUNCT syndrome is refractory to medical therapy but there is increasing evidence for treatment with lamotrigine16,17.
Temporal arteritis
Temporal arteritis (also known as giant cell arteritis) is characterized by daily headaches of moderate to severe intensity, scalp sensitivity, fatigue, and various non-specific complaints with a general sense of illness. Ninety-five per cent of patients are over 60 years old. The pain is usually unilateral, although in some cases bilateral or occipital pain do occur. Pain may also be felt in the tongue and is a continuous ache with superimposed sharp, shooting head pains. The pain is similar to and may be confused with that of cluster headache (CH), but CH tends to occur in younger patients. The two may also be distinguished on physical exam, when dilated and tortuous scalp arteries are noted. The erythrocyte sedimentation rate (ESR) is markedly elevated in temporal arteritis18. Definitive diagnosis is made by artery biopsy from the region of the pain, although negative biopsy may be caused by the spotty nature of the disease and does rule out the diagnosis. High dose steroid therapy usually precipitates a dramatic decrease in head pain. Failure to respond to steroid therapy with a negative biopsy should call the diagnosis into question. If the diagnosis seems likely based on history and physical examination, steroids should be started immediately to avoid vision loss, which is the most common complication of the disorder, occurring in 30% of untreated cases. The biopsy remains positive for 7–10 days from starting steroid therapy. Steroids may be tapered to an alternate day maintenance schedule when the pain resolves and ESR normalizes. The disease is usually active for 1–2 years, during which time steroids should be continued to prevent vision loss.
Figure 1.
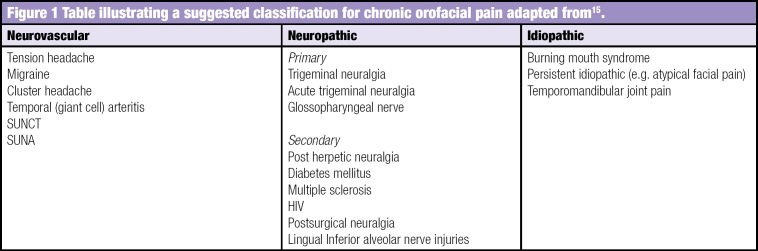
Table illustrating a suggested classification for chronic orofacial pain adapted from15.
Group 2: Neuralgia
This group includes primary neuropathies (trigeminal neuralgia (typical or atypical) and glossopharyngeal neuralgia), and secondary neuropathies including postherpetic neuralgia and post-traumatic V neuralgia, and other peripheral neuropathies affecting the trigeminal system. Nutritional neuropathy, diabetes mellitus, human immunodeficiency virus (HIV), chemotherapy, and multiple sclerosis (MS) are not covered in this review but can present as orofacial pain.
Primary neuropathies
Trigeminal neuralgia (typical or atypical) is covered elsewhere in this issue19.
Glossopharyngeal neuralgia
Glossopharyngeal neuralgia is characterized by pain attacks similar to those in trigeminal neuralgia, but is located unilaterally in the distribution of the glossopharyngeal nerve. Pain is most common in the posterior pharynx, soft palate, base of tongue, ear, mastoid or side of the head. Swallowing, yawning, coughing or phonation may trigger the pain. Management is similar to that for trigeminal neuralgia20.
Secondary neuropathies
Many conditions can cause peripheral sensory neuropathies20 that may present with pain, these include;
Diabetes
Post herpetic neuralgia
Human Immunodeficiency Virus
Chemotherapy
Multiple Sclerosis
Post surgical traumatic neuropathy
Parkinson's disease
Malignancy
Drugs e.g. Growth hormone injections
Nutritional neuropathy
The most common causes of trigeminal neuropathy would include postherpetic neuralgia, post traumatic neuropathy and idiopathic persistent post surgical pain.
Postherpetic neuralgia (PHN)
In patients over 50 years of age there is a 60% incidence of developing postherpetic pain. Herpetic skin eruption is caused by the reactivation of latent varicella zoster virus from the sensory nerve ganglia. The reactivated virus is carried via the axons distally to the skin where it produces a painful rash with crusting vesicles in a dermatomal distribution. The trigeminal nerve is the second most commonly affected after nerves in the thoracic region. Ramsay Hunt syndrome occurs when herpes zoster infection of the geniculate ganglion causes earache and facial palsy. Pain that persists two or more months after the acute eruption is known as postherpetic neuralgia (PHN). The pain is neuropathic in nature, severe, and it is associated with allodynia and hyperalgesia, most commonly affecting the 1st (ophthalmic) distribution of the trigeminal nerve. High doses of antivirals, steroids, and amitriptyline are often used for the acute eruption in otherwise healthy individuals21. Antivirals, NSAIDs, and opioids are often used in immunocompromised patients. More recently, there is evidence that topical 5% lidocaine plasters (Versatis) worn alternatively every 12 hours are very effective22. NICE have provided prescribing guidance for neuropathic pain23.
Post-traumatic trigeminal neuropathy
The most problematic outcome of dental surgical procedures with major medico-legal implications is injury to the trigeminal nerve24. The prevalence of temporarily impaired lingual and inferior alveolar nerve function is thought to range between 0.15–0.54% whereas permanent injury caused by injection of local analgesics is much less frequent at 0.0001–0.01%25,26. Traumatic injuries to the lingual and inferior alveolar nerves may induce a pain syndrome owing to the development of a neuroma. The most commonly injured trigeminal nerve branches, the inferior alveolar nerve (IAN) and lingual nerves are different entities, whereby the lingual nerve sits loosely in soft tissue compared with the IAN that resides in a bony canal. Injury to the third division of the trigeminal may occur due to a variety of different treatment modalities, such as major maxillofacial and minor oral surgery27–31. Peripheral sensory nerve injuries are more likely to be persistent when the injury is severe, if the patient is older, if the time elapsed between the cause of the injury and the review of the patient is of longer duration, and when the injury is more proximal to the cell body.
Subsequent to iatrogenic trigeminal nerve injury, the patient often complains about a reduced quality of life, psychological discomfort, social disabilities and handicap32. Patients often find it hard to cope with such negative outcomes of dental surgery since the patient usually expects significant improvements not only regarding jaw function, but also in relation to dental, facial, and even overall body image after oral rehabilitation33. Altered sensation and pain in the orofacial region may interfere with many daily functions as illustrated in Figure 234.
Figure 2.

Interference of daily functions associated with dental pain
In a recent prospective assessment of 252 patients with iatrogenic trigeminal nerve injuries35 most were caused by third molar surgery but implants and local anaesthesia were significant contributors (Figure 3).
Figure 3.

Factors associated with iatrogenic trigeminal nerve injury
The diagnosis of posttraumatic neuralgia/neuropathy is based upon a history of surgery or trauma temporally correlated with the development of the characteristic neuropathic pain. Age, poor wound closure, infections, foreign material in the wound, haematoma, skull fracture, diabetes mellitus or peripheral neuropathy elsewhere in the body predispose to neuroma development. The pains commonly persist 2 months after the injury and can be permanent. Medical therapy is similar to that used in neuropathic pain conditions depending on the patients' symptoms.
In a recent survey of 252 iatrogenic trigeminal nerve injuries related to dental treatment, 70% of patients presented with pain (Figure 3). This highlights the problems related to postsurgical neuropathy aggravated by the fact that many patients may not have been warned at all about nerve injury or told that they would risk numbness.
Many patients experienced significant daily disability predominantly caused by elicited mechanical or cold allodynia resulting in pain on eating, drinking, kissing sleeping and other essential functions (Figure 4). The inferior alveolar nerve (IAN) supplies general sensation to the lower chin, lip, vermillion gums and teeth unilaterally. The lingual nerve (LN) supplies general sensory to dorsal and ventral aspects of the tongue and lingual gingivae.
Figure 4.

Pain and altered sensation in patients with inferior alveolar nerve injury (IANI)
Current management of these nerve injuries is inadequate. The focus remains on surgical correction or laser therapy with little or no attention to medical or counselling intervention and the patients' psychological, functional or pain related complaints. The fault partly rests with how we assess these patients. Assessment tends to show little regard for the functional or pain evaluation with the main focus on basic mechanosensory evaluation, which is not necessarily reflective of the patients' difficulties. Oral Surgery specialists assessing these injuries should therefore follow guidelines from the World Health Organisation, which suggest that nerve injury outcomes should be assessed in terms of impairment, activity limitations, and participation restrictions36. Guidelines set out by the International Association for the Study of Pain and European Federation of Neurological Societies should also be followed37. Without exception these recommendations are holistic when compared with reports evaluating the management of trigeminal nerve injuries.
Traumatic injuries to peripheral nerves pose complex challenges and treatment of nerve injuries must consider all aspects of the inherent disability. Pain control is of paramount importance and rehabilitation needs to be instituted as first-line treatment. Early intervention is important for optimal physiologic and functional recovery34. Reparative surgery may be indicated when the patient complains of persistent problems related to the nerve injury, however there remains a significant deficiency in evidence base to support this practice. The patients presenting complaints may include functional problems due to the reduced sensation, intolerable changed sensation or pain the latter being predominantly intransigent to surgery39–41 and less often expressed psychological problems relating the iatrogenesis of the injury and chronic pain. Generally for lesions of the peripheral sensory nerves in man, the gold standard is to repair the nerve as soon as possible after injury42. However, the relatively few series of trigeminal nerve repair on human subjects relate mainly to repairs undertaken at more than 6 months after injury.
It is evident from the literature review that there needs to be a cultural change in the choice of intervention, timing and outcome criteria that should be evaluated for interventions for trigeminal nerve injuries. To date, there have been a very limited number of prospective randomised studies to evaluate the effect of treatment delay on, the surgical, medical or counselling outcomes for trigeminal nerve injuries in humans.
Persistent post surgical pain without demonstrable neuropathy
This is defined as pain that is present one year or longer post surgical procedure, that is unexplained by local factors and is best described as neuropathic in nature.
Nonodontogenic dentolalveolar pain is often difficult to diagnose because it is poorly understood20. Even defining and categorizing such persistent pain is challenging. Nonodontogenic pain may represent half of all cases of persistent tooth pain, as shown by a recent systematic review of prospective studies that reported the frequency of nonodontogenic pain in patients who had undergone endodontic procedures. Nonodontogenic pain was defined as dentoalveolar pain present for 6 months or more after endodontic treatment without evidence of dental pathology. Endodontic procedures reviewed were nonsurgical root canal treatment, retreatment, and surgical root canal treatment. 770 articles were retrieved and reviewed, 10 met the inclusion criteria with a total of 3,343 teeth enrolled within the included studies. 1,125 had follow-up information regarding pain status. The authors identified nonodontogenic pain in 3.4% (95% confidence interval, 1.4%-5.5% frequency of occurrence)43.
The prevalence of persistent post surgical pain in the trigeminal system may be low compared with other surgical sites44.
However when one considers the significant frequency of dental surgical procedure undertaken (Figure 5) then significant numbers of individuals may be affected by both post traumatic neuropathy and persistent post surgical pain.
Figure 5.
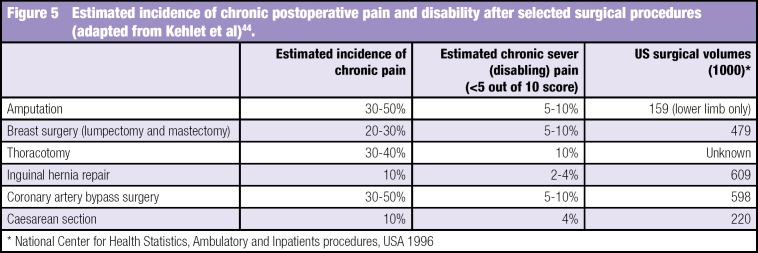
Estimated incidence of chronic postoperative pain and disability after selected surgical procedures (adapted from Kehlet et al)44.
Risk factors for developing persistent post surgical pain include; genetics (deficiency of the enzyme catecholamine-O- methyltransferase), preceding pain (intensity and chronicity), psychosocial factors (i.e. fear, memories, work, physical levels of activity, somatization), age (older = increased risk), gender (female = increased risk) and the surgical procedure and technique (tension due to retraction).
All these persistent post surgical pain conditions may be attributable to post traumatic neuropathy but it is difficult to be conclusive without a demonstrable neuropathic area in relation to the previous surgery. The significant decreased incidence in this condition in the trigeminal region may reflect the lack of central sensitization due to most procedures being undertaken under local anaesthetic45.
Group 3 Idiopathic chronic orofacial pain
This group includes preauricular pain related to the TMJ, burning mouth syndrome (BMS), and persistent idiopathic facial pain.
Temporomandibular joint pain is reviewed separately in this issue11.
Persistent idiopathic facial pain (PIFP)
The term atypical facial pain was first introduced by Frazier and Russell in 1924. It has since been renamed persistent idiopathic facial pain (PIFP). PIFP refers to pain along the territory of the trigeminal nerve that does not fit the classic presentation of other cranial neuralgias16. The duration of pain is usually long, lasting most of the day (if not continuous). Pain is unilateral and without autonomic signs or symptoms. It is described as a severe ache, crushing or burning sensation. Upon examination and workup no abnormality is noted.
Definition
According to the International Association for the Study of Pain (IASP), chronic facial pain refers to symptoms which have been present for at least 6 months. ‘Atypical’ pain is a diagnosis of exclusion after other conditions have been considered and eliminated (i.e. it is idiopathic), and is characterized by chronic, constant pain in the absence of any apparent cause in the face or brain. Many information sources suggest that all ‘unexplained’ facial pains are termed atypical facial pain but this is not the case. Categories of idiopathic facial pain conditions include neuropathic pain due to sensory nerve damage, complex regional pain syndrome (CRPS) from sympathetic nerve damage and atypical facial pain46. Atypical odontalgia, or phantom tooth pain, is a variation of atypical facial pain where intense discomfort is centred around a tooth or group of teeth with no obvious dental or oral disease.
Epidemiology of PIFP
Atypical facial pain is more common in women than in men; most patients attending a facial pain clinic are women aged between 30 and 50 years. Although any area of the face can be involved, the most commonly affected area is the maxillary region. In the majority of patients there is no disease or other cause found. In a few patients the symptoms represent serious disease. In a small number of patients the pain may be one consequence of significant psychological or psychiatric disease46.
Clinical presentation
Atypical facial pain has a very variable presentation. Often it is characterized by continuous, daily pain of variable intensity. Typically, the pain is deep and poorly localized, is described as dull and aching, and does not waken the patient from sleep. At onset the pain may be confined to a limited area on one side of the face, while later it may spread to involve a larger area. Atypical facial pain is a diagnosis of exclusion for pain not meeting the diagnostic criteria of other facial pain syndromes. Mongini et al47 refers to the term atypical facial pain as outdated and includes its description under the category of psychogenic facial pain. Indeed, the description of the pain may be inconsistent because the patient can complain of bilateral pain that often changes locations over weeks to months. The pain is not triggered and is not electrical in quality. Intensity fluctuates but the patient is rarely pain-free. Pain is typically located in the face and seldom spreads to the cranium in contradistinction to tension headache. It is more common in women aged 30–50 years old.
Between 60 and 70% of these patients have significant psychiatric findings, usually depression, somatization or adjustment disorders, therefore psychiatric evaluation is indicated. Treatment is with antidepressants, beginning with low dose amitriptyline at bedtime and increasing the dose until pain and sleep are improved48. Accurate figures are difficult to obtain because of the lack of agreement on classification criteria. Estimated incidence is 1 case per 100 000 population, although this number may be underestimated. PIFP affects both sexes approximately equally, but more women than men seek medical care. The disorder mainly affects adults and is rare in children. PIFP is essentially a diagnosis of exclusion.
Daily or near-daily headaches are a widespread problem in clinical practice. According to population-based data from the United States, Europe, and Asia, chronic daily headache affects a large number (approximately 4–5% of the population) of patients. Importantly, PIFP must be distinguished from various other chronic daily headache syndromes, including hemicrania continua, TMJ syndrome, sidelocked migraine, chronic cluster headache, SUNCT, TN, and many others. A careful history and physical examination, including a dental consultation, laboratory studies, and imaging studies, may be necessary to rule out occult pathology. Underlying pathology such as malignancy, vasculitis, infection, and central or peripheral demyelination may manifest early as neuralgia, and, not until focal neurological deficits, imaging abnormalities, or laboratory abnormalities are discovered, does the diagnosis become evident. Rare cases of referred pain must also be considered.
Atypical odontalgia (AO) is characterized by continuous, dull, aching, or burning pain of moderate intensity in apparently normal teeth or endodontically treated teeth and occasionally in extraction sites. AO is not usually affected by testing the tooth and surrounding tissues with cold, heat or electrical stimuli. The pain remains constant despite repeated dental treatment, even extractions in the region, often rendering patients with persistent pain but whole quadrants stripped of dentition. Moreover, the toothache characteristics frequently remain unchanged for months or years, contributing to the differentiation of AO from pulpal dental pain. Occasionally, the pain may spread to adjacent teeth, especially after extraction of the painful tooth. These patients are defined as having pain in a tooth or tooth region in which no clinical or radiological findings can be detected.
Several studies have been conducted to define this group more clearly. AO patients have more comorbid pain conditions, higher scores for depression and somatization, significant limitation in jaw function, and lower scores on quality of life measures when compared with controls49. When compared to patients with TMD, AO patients were more likely to describe their pain as aching, find rest relieving but cold and heat aggravating. Over 80% relate the onset of their pain to dental treatment. Both groups show worsening of symptoms on chewing, but more patients with TMD have other chronic pain. These patients have somatosensory abnormalities, suggesting that generalized sensitization of the nociceptive mechanism may be occurring. The author believes that the relationship with previous surgical intervention infers that this condition may, in some cases, be partial postsurgical neuropathy of the superior alveolar nerves.
The lack of randomised controlled trials (RCTs) makes evidenced-based care in AO difficult49. One of the major problems with this condition is convincing the patient, and informing their dentist, that there are no dental causes for their pain, so avoiding unnecessary irreversible invasive dental treatment. AO patients are often diagnosed late50 and therefore need a multidisciplinary approach. In her recent review, Baad-Hansen51 presents a sensible progressive approach to managing AO, beginning with topical lidocaine or capsaicin, then tricyclic anti-depressants. Ultimately, the drugs used in neuropathic pain are often gabapentin and pregabalin, tramadol or oxycodone.
Medical care of PIFP
Medical treatment of PIFP is usually less satisfactory than medical treatment for other facial pain syndromes49. Medications used to treat PIFP include antidepressants, anticonvulsants, substance P depletion agents, topical anaesthetics, N-methyl-D-aspartate (NMDA) antagonists, and opioid medications. Of these classes of medications, anticonvulsants and antidepressants appear to be the most effective as the neuropathic component of pain responds well to them. Pharmacotherapeutic knowledge is paramount in the treatment of this refractory pain syndrome.
A multimechanistic approach, using modulation of both ascending and descending pain pathways, is frequently necessary. The goal of therapy is to manage the pain effectively with the fewest adverse medication effects. Anticonvulsants and antidepressants are the mainstays of medication treatment. Alternative therapies such as acupuncture and neuromuscular re-education should be considered as part of a comprehensive treatment plan. Psychological, or occasionally psychiatric, treatment is important in the overall management of a patient with chronic pain. Holistic approach as many has other chronic pain. Available data on alternative treatments are limited.
Surgical care
Details of neurosurgical interventions are beyond the scope of this review. This form of therapy should be considered at a centre well versed in these procedures49.
Consultations
Psychometric testing may be of benefit in the evaluation and treatment of patients with headache and facial pain. Many tests have been applied, but probably the most widely used is the Minnesota multiple personality inventory (MMPI). While especially useful in the evaluation of chronic headache and facial pain patients, a thorough discussion of psychometric testing is beyond the scope of this discussion and is mentioned here only for completeness. Consultation with a dentist may be of benefit. All treatments should be provided in cooperation with the patient's primary care physician.
Conclusion
Chronic orofacial pain continues to present a diagnostic challenge for many practitioners. Patients are frequently misdiagnosed and they can often suffer from psychological/psychiatric symptoms of depression and anxiety. Treatment is less effective than in other pain syndromes and a multidisciplinary approach treatment is desirable.
References
- 1.Hapak L, Gordon A, Locker D, Shandling M, Mock D, Tenenbaum HC. Differentiation between musculoligamentous, dentoalveolar and neurologically based craniofacial pain with a diagnostic questionnaire Journal of Orofacial Pain 1994; 8 (4) 357–638 [PubMed] [Google Scholar]
- 2.Lipton JA, Ship JA, Larach-Robinson D. Estimated prevalence and distribution of reported orofacial pain in the United States. Journal of the American Dental Association 1993; 124 (10) 115–121 [DOI] [PubMed] [Google Scholar]
- 3.Riley JL, 3rd, Gilbert GH. Orofacial pain symptoms: an interaction between age and sex Pain 2001; 90 (3) 245–256 [DOI] [PubMed] [Google Scholar]
- 4.Locker D, Grushka M. The impact of dental and facial pain. Journal of Dental Research 1987; 66 (9) 1414–1417 [DOI] [PubMed] [Google Scholar]
- 5.Bonica JJ. Pain: introduction. Research Publications — Association for Research in Nervous and Mental Disease 1980; 58 1–17. [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention. National Health Interview Survey Orofacial Pain Supplement. National Center for Health Statistics, Atlanta GA, 1989 [Google Scholar]
- 7.Benoliel R, Birman N, Eliav E, Sharav Y. The International Classification of Headache Disorders: accurate diagnosis of orofacial pain? Cephalalgia 2008; 28 (7) 752–762 [DOI] [PubMed] [Google Scholar]
- 8.Türp JC, Hugger A, Nilges P, Hugger S, Siegert J, Busche E, Effenberger S, Schindler HJ on behalf of the German Chapter of the International Association for the Study of Pain (IASP) Recommendations for the standardized evaluation and classification of painful temporomandibular disorders: an update Schmerz 2006; 20 (6) 481–489 [DOI] [PubMed] [Google Scholar]
- 9.Zebenholzer K, Wober C, Vigl M, Wessely P, Wober-Bingol C. Facial pain and the second edition of the international classification of headache disorders. Headache 2006; 46 (2) 259–263 [DOI] [PubMed] [Google Scholar]
- 10.De Boever JA, Nilner M, Orthlieb JD, Steenks MH. Recommendations by the EACD for examination, diagnosis, and management of patients with temporomandibular disorders and orofacial pain by the general dental practitioner. Journal of Orofacial Pain 2008; 22 (3) 268–278 [PubMed] [Google Scholar]
- 11.Durham J. Recent Advancements in Temporomandibular disorders (TMD). Reviews in Pain. 2011; 5 (1) 18–25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kiyak HA, Beach BH, Worthington P, Taylor T, Bolender C, Evans J. Psychological impact of osseointegrated dental implants International Journal of Oral and Maxillofacial Implants 1990; 5 (1) 9–61 [PubMed] [Google Scholar]
- 13.Ravaghi V, Farrahi-Avval N, Locker D, Underwood M. Validation of the Persian Short Version of the Oral Health Impact Profile (OHIP-14) Oral Health & Preventive Dentistry 2010; 8 (3) 229–235 [PubMed] [Google Scholar]
- 14.Renton T. Dental (odontological) pain. Reviews in Pain. 2011; 5 (1) 2–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Woda A, Tubert-Jeannin S, Bouhassira D, et al. Towards a new taxonomy of idiopathic orofacial pain Pain 2005; 116 (3) 396–406 [DOI] [PubMed] [Google Scholar]
- 16.Pareja JA, Kruszewski P, Sjaastad O. SUNCT syndrome. Diagnosis morbi. Shortlasting unilateral neuralgiform headache attacks, with conjunctival injection, tearing and rhinorrhoea. Neurologia Supplement 1997; (5) 66–72 [PubMed] [Google Scholar]
- 17.Balasubramaniam R, Klasser GD, Delcanho R. Trigeminal autonomic cephalalgias: a review and implications for dentistry. Journal of the American Dental Association 2008; 139 (12) 1616–1624 [DOI] [PubMed] [Google Scholar]
- 18.Affolter B, Thalhammer C, Aschwanden M, Glatz K, Tyndall A, Daikeler T. Difficult diagnosis and assessment of disease activity in giant cell arteritis: a report on two patients. Scandinavian Journal of Rheumatology 2009; 38 (5) 1–2 [DOI] [PubMed] [Google Scholar]
- 19.McMillan R. Trigeminal Neuralgia - a debilitating facial pain. Reviews in Pain. 2011; 5 (1) 26–35 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Teixeira MJ, de Siqueira SR, Bor-Seng-Shu E. Glossopharyngeal neuralgia: neurosurgical treatment and differential diagnosis. Acta Neurochirugica (Wien) 2008; 150 (5) 471–475 [DOI] [PubMed] [Google Scholar]
- 21.Benoliel R, Eliav E. Neuropathic orofacial pain. Oral Maxillofacial Surgical Clinics of North America 2008; 20 (2) 237–254, vii. [DOI] [PubMed] [Google Scholar]
- 22.Baron R, Mayoral V, Leijon G, et al. Efficacy and safety of 5% lidocaine (lignocaine) medicated plaster in comparison with pregabalin in patients with postherpetic neuralgia and diabetic polyneuropathy: interim analysis from an open-label, two-stage adaptive, randomized, controlled trial. Clinical Drug Investigation 2009; 29 (4) 231–241 [DOI] [PubMed] [Google Scholar]
- 23.NICE Neuropathic pain. The pharmacological management of neuropathic pain in adults in non-specialist settings. NICE, London: 2010. Available from http://www.nice.org.uk/nicemedia/live/12948/47949/47949.pdf [Accessed 17.01.2011] [Google Scholar]
- 24.Caissie R, Goulet J, Fortin M, Morielli D. Iatrogenic paresthesia in the third division of the trigeminal nerve: 12 years of clinical experience Journal of the Canadian Dental Association 2005; 71 (3)185–190 [PubMed] [Google Scholar]
- 25.Hillerup S. Iatrogenic injury to the inferior alveolar nerve: etiology, signs and symptoms, and observations on recovery. International Journal of Oral and Maxillofacial Surgery 2008; 37 (8) 704–709 [DOI] [PubMed] [Google Scholar]
- 26.Renton T, Thexton A, Crean SJ, Hankins M. Simplifying the assessment of the recovery from surgical injury to the lingual nerve. British Dental Journal 2006; 200 (10) 569–573 [DOI] [PubMed] [Google Scholar]
- 27.Blackburn CW. A method of assessment in cases of lingual nerve injury. British Journal of Oral & Maxillofacial Surgery 1990; 28(4):238–245 [DOI] [PubMed] [Google Scholar]
- 28.Kraut RA, Chahal O. Management of patients with trigeminal nerve injuries after mandibular implant placement. Journal of the American Dental Association 2002; 133 (10) 1351–1354 [DOI] [PubMed] [Google Scholar]
- 29.Wismeijer D, van Mass M, Vermeeren J, Kalk W. Patients' perception of sensory disturbances of the mental nerve before and after implant surgery: a prospective study of 110 patients. British Journal of Oral & Maxillofacial Surgery 1997; 35 (4) 254–259 [DOI] [PubMed] [Google Scholar]
- 30.Hillerup S, Jensen R. Nerve injury caused by mandibular block analgesia International Journal of Oral and Maxillofacial Surgery 2006; 35 (5) 437–443 [DOI] [PubMed] [Google Scholar]
- 31.Grötz KA, Al-Nawas B, de Aguiar EG, Schulz A, Wagner W. Treatment of injuries to the inferior alveolar nerve after endodontic procedures Clinical Oral Investigations 1998; 2 (2) 73–76 [DOI] [PubMed] [Google Scholar]
- 32.Lam NP, Donoff RB, Kaban LB, Dodson TB. Patient satisfaction after trigeminal nerve repair Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 2003; 95 (5) 538–543 [DOI] [PubMed] [Google Scholar]
- 33.Kiyak HA, Beach BH, Worthington P, Taylor T, Bolender C, Evans J. Psychological impact of osseointegrated dental implants International Journal of Oral Maxillofacial Implants 1990; 5 (1) 9–61 [PubMed] [Google Scholar]
- 34.Ziccardi VB, Zuniga JR. Nerve injuries after third molar removal Oral Maxillofacial Surgical Clinics of North America 2007; 19 (1) 105–115 [DOI] [PubMed] [Google Scholar]
- 35.Renton T, Yilmaz Z. A review of 253 post traumatic trigeminal nerve injuries. Journal of Orofacial Pain. In press.
- 36.MacDermid JC. Measurement of health outcomes following tendon and nerve repair Journal of Hand Therapy 2005; 18 (2) 297–312 [DOI] [PubMed] [Google Scholar]
- 37.Cruccu G, Anand P, Attal N, Garcia-Larrea L, Haanpää M, Jørum E, Serra J, Jensen TS. EFNS guidelines on neuropathic pain assessment European Journal of Neurology 2004; 11 (3)153–162 [DOI] [PubMed] [Google Scholar]
- 38.Zuniga JR. Surgical management of trigeminal neuropathic pain. In: Microneurosurgery of the trigeminal nerve. Atlas of Oral Maxillofacial Surgical Clinics of North America 2001; (9) 59–74 [PubMed] [Google Scholar]
- 39.Rutner TW, Ziccardi VB, Janal MN. Long-term outcome assessment for lingual nerve microsurgery. Journal of Oral and Maxillofacial Surgery 2005; 63 (8) 1145–1149 [DOI] [PubMed] [Google Scholar]
- 40.Hillerup S. Iatrogenic injury to oral branches of the trigeminal nerve: records of 449 cases. Clinical Oral Investigations 2007; 11 (2) 133–142 [DOI] [PubMed] [Google Scholar]
- 41.Robinson PP, Loescher AR, Smith KG. A prospective, quantitative study on the clinical outcome of lingual nerve repair. British Journal of Oral & Maxillofacial Surgery 2000; 38 (4) 255–263 [DOI] [PubMed] [Google Scholar]
- 42.Birch R, Bonney G, Dowell J, Hollingdale J. Iatrogenic injuries of peripheral nerves. Journal of Bone and Joint Surgery. British Volume 1991; 73 (2) 280–282 [DOI] [PubMed] [Google Scholar]
- 43.Nixdorf N, Moana-Filho EJ, Law AS, et al. Frequency of Nonodontogenic Pain after Endodontic Therapy: A Systematic Review and Meta-Analysis Journal of Endodontics 2010; 36 (9) 1494–1498 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention The Lancet 2006; 367 (9522) 1618–1625 [DOI] [PubMed] [Google Scholar]
- 45.Woolf C, Mannion RJ. Neuropathic pain: aetiology, symptoms, mechanisms and management The Lancet 1999; 353 (9168) 1959–1964 [DOI] [PubMed] [Google Scholar]
- 46.Evans RW, Agostoni E. Persistent idiopathic facial pain. Headache 2006; 46 (8) 1298–1300 [DOI] [PubMed] [Google Scholar]
- 47.Mongini F, Ferla E, Maccagnani C. MMI profiles in patients with headaches or craniofacial pain: a comparative study. Cephalalgia 1992; 12 (2) 91–98 [DOI] [PubMed] [Google Scholar]
- 48.Abrahamsen R, Baad-Hansen L, Svensson P. (2008) Hypnosis in the management of persistent idiopathic orofacial pain—clinical and psychosocial findings Pain 136 (1–2) 44–52 [DOI] [PubMed] [Google Scholar]
- 49.Baad-Hansen L. Atypical odontalgia—pathophysology and clinical management Journal of Oral Rehabilitation 2008; 35 (1) 1–11 [DOI] [PubMed] [Google Scholar]