

Abstract
Pomalidomide is a distinct oral IMiD® immunomodulatory agent with direct antimyeloma, stromal-support inhibitory, and immunomodulatory effects. The pivotal, multicenter, open-label, randomized phase 3 trial MM-003 compared pomalidomide + low-dose dexamethasone vs high-dose dexamethasone in 455 patients with refractory or relapsed and refractory multiple myeloma after failure of bortezomib and lenalidomide treatment. Initial results demonstrated significantly longer progression-free survival and overall survival with an acceptable tolerability profile for pomalidomide + low-dose dexamethasone vs high-dose dexamethasone. This secondary analysis describes patient outcomes by treatment history and depth of response. Pomalidomide + low-dose dexamethasone significantly prolonged progression-free survival and favored overall survival vs high-dose dexamethasone for all subgroups analyzed, regardless of prior treatments or refractory status. Both univariate and multivariate analyses showed that no variable relating to either the number (≤ or > 3) or type of prior treatment was a significant predictor of progression-free survival or overall survival. No cross-resistance with prior lenalidomide or thalidomide treatment was observed. Patients achieving a minimal response or better to pomalidomide + low-dose dexamethasone treatment experienced a survival benefit, which was even higher in those achieving at least a partial response (17.2 and 19.9 months, respectively, as compared with 7.5 months for patients with less than minimal response). These data suggest that pomalidomide + low-dose dexamethasone should be considered a standard of care in patients with refractory or relapsed and refractory multiple myeloma regardless of prior treatment. ClinicalTrials.gov: NCT01311687; EudraCT: 2010-019820-30.
Introduction
The advent of agents such as lenalidomide (LEN), bortezomib (BORT), and thalidomide (THAL) throughout the treatment continuum of multiple myeloma (MM) has dramatically improved the survival of patients. According to the US Surveillance, Epidemiology, and End Results Program database, 5-year survival rates have increased from 29% during the period from 1990 to 1992 to 40% during the period from 2003 to 2007.1,2 Recent trials incorporating BORT maintenance and LEN continuous therapy have extended first-line progression-free survival (PFS) to nearly 3 years in stem cell transplant–ineligible patients, and beyond 3 years in transplant-eligible patients.3–6
Despite these improvements in frontline patient management, most patients with MM will ultimately relapse and become refractory to previous therapies, leading to poor prognosis. A recent retrospective analysis of patients with advanced refractory or relapsed and refractory MM (RRMM), in whom BORT and immunomodulatory agents have failed, found that alkylating agents such as cyclophosphamide, cyclophosphamide together with corticosteroids or high-dose dexamethasone (HiDEX) were the most common classes of drugs used; corticosteroid monotherapy was also widely used but with limited efficacy.7 Only 24% of patients achieved partial response (PR) or better to any treatment after failure of BORT and an immunomodulatory agent, with a median overall survival (OS) of only 9 months for those who received further treatment and 3 months for those who did not; however, patients were more likely to have been treated with THAL than with LEN.7 Thus, new, effective therapies are needed for the management of patients who have exhausted treatment with BORT, LEN, and THAL.
In the treatment of RRMM, the decision whether to switch agent classes (i.e. from immunomodulatory agent to proteasome inhibitor, or vice versa) or to treat with another agent of the same class remains an open debate. Data on BORT retreatment, LEN therapy following THAL, and carfilzomib use after BORT have been mixed.8–10 In patients with newly diagnosed MM and early RRMM, better depth of response has been associated with improvements in outcome measures, such as survival and duration of response (DOR).11–15 In most of these patients, a deep response (≥ very good partial response (VGPR)) is the treatment goal. However, in patients with RRMM, minimal response (MR) may also be a clinically relevant outcome of treatment.
The distinct oral IMiD® immunomodulatory agent pomalidomide (POM) has been shown to exhibit direct antimyeloma, stromal-support inhibitory, and immunomodulatory effects.16,17 Phase 2 clinical trial results have demonstrated the efficacy and safety of POM with low-dose dexamethasone (LoDEX) in the treatment of patients with RRMM.18–21 POM + LoDEX was compared with HiDEX in patients with RRMM after failure of BORT and LEN in the international, multicenter, open-label, randomized phase 3 trial MM-003.22 POM + LoDEX treatment was found to significantly improve PFS and OS. This benefit was also observed in patients refractory to LEN as their last prior treatment. Consistent with the established tolerability profile of POM + LoDEX,18–21 the most common grade 3/4 adverse events observed for POM + LoDEX were hematologic (neutropenia, anemia, and thrombocytopenia).8–21 The current publication reports efficacy from the MM-003 trial by depth of response, number of prior therapies, and types of prior therapies in the MM-003 trial.
Methods
Study design and patients
MM-003 was an open-label, randomized, phase 3 registration trial conducted in 93 centers in Europe, Russia, Australia, Canada, and the United States. All patients provided written informed consent. The study was approved by institutional review boards or independent ethics committees at all participating centers, and was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonization Guidelines for Good Clinical Practice. This trial is registered with ClinicalTrials.gov (NCT01311687) and EudraCT (2010-019820-30). All authors and the sponsor were involved in data gathering and analysis, review, interpretation, and writing of the report.
Full study results have previously been reported.22 Briefly, patients were aged ≥ 18 years and were required to have had RRMM treated with ≥ 2 prior antimyeloma regimens, been refractory to their last prior treatment, failed prior treatment with BORT and LEN (following ≥ 2 previous consecutive cycles of each, alone or in combination), and received adequate prior alkylator therapy. Failure of BORT or LEN therapy was defined as progressive disease during or within 60 days of completing treatment, progressive disease ≤ 6 months after achieving PR or better, or intolerance without achieving MR or better (BORT only).
455 patients were randomized in a 2:1 ratio to receive 28-day cycles of POM (4 mg/day orally on days 1–21) + LoDEX (40 mg/day orally on days 1, 8, 15, and 22) or HiDEX (40 mg/day orally on days 1–4, 9–12, and 17–20). For both arms, DEX was administered at a dose of 20 mg/day for patients aged ≥ 75 years. Treatment was continued until progression or unacceptable toxicity. Thromboprophylaxis consisting of the physician’s choice of low-dose aspirin or low-molecular-weight heparin (or equivalent) was required for all patients who received POM and those at high risk of developing thrombosis.
Assessments and statistical analysis
The primary endpoint was PFS, with treatment groups compared using a log-rank test. Secondary endpoints included OS, overall response rate (ORR; the proportion of patients achieving a PR or better), time to progression (TTP), DOR, safety, and quality of life. The PFS and ORR presented in this report were based on investigator assessment using International Myeloma Working Group criteria23 or European Group for Blood and Marrow Transplantation criteria24 (for MR only). Reduction in levels of M-protein was also assessed.
The Kaplan-Meier product-limit method was used to estimate PFS, OS, and DOR, which were then compared between treatment groups using log-rank tests stratified by age, disease population, and number of prior antimyeloma therapies. ORR was compared between treatment arms using the Fisher’s exact test. Subgroup analyses for PFS and OS were carried out using unstratified log-rank tests and presented in forest plots. Multivariate analyses were also performed using a Cox model to assess the effect of prior therapies on PFS and OS.
Results
Patient characteristics
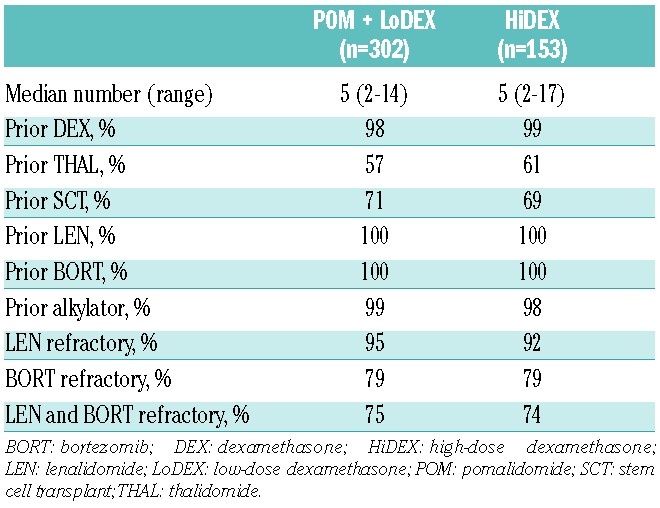
The reported analysis used the most recent data available for MM-003 (cutoff September 1, 2013; median follow-up 15.4 months). Patient disposition is shown in Figure 1. Baseline characteristics were well balanced between treatment arms, as previously described.22 Per protocol, this heavily pretreated patient population (median, 5 lines of prior therapy in both arms) had received prior LEN and BORT (Table 1). Nearly all patients were refractory to LEN (POM + LoDEX arm, 95%; HiDEX arm, 92%), and most were refractory to both LEN and BORT (POM + LoDEX, 75%; HiDEX, 74%).
Figure 1.
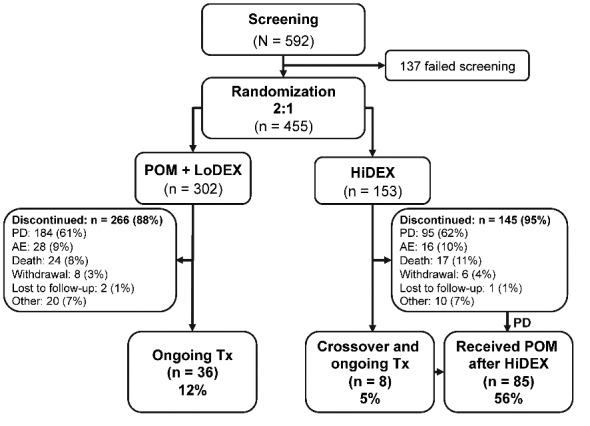
Disposition of MM-003 trial participants as of September 1, 2013. AE: adverse event; HiDEX: high-dose dexamethasone; LoDEX: low-dose dexamethasone; PD: progressive disease; POM: pomalidomide; Tx: treatment.
Table 1.
Prior therapies.
Survival and response (intent-to-treat population)
In the intent-to-treat population, with extended followup, median PFS was significantly longer with POM + LoDEX vs. HiDEX (4.0 vs. 1.9 months; hazard ratio (HR), 0.50; P<0.001). Median OS was significantly longer with POM + LoDEX vs. HiDEX (13.1 vs. 8.1 months; HR, 0.72; P=0.009). This OS advantage was observed despite 85 patients (56%) on the HiDEX arm receiving subsequent POM. A significantly higher ORR (PR or better) was achieved in patients treated with POM + LoDEX vs. HiDEX (32% vs. 11%; P<0.001). 40% of patients receiving POM + LoDEX and 15% of patients receiving HiDEX achieved an MR or better. The median DOR (for patients with a PR or better) was also significantly longer with POM + LoDEX than with HiDEX (7.5 vs. 5.1 months; P=0.031). 82% of patients receiving POM + LoDEX and 61% of patients receiving HiDEX achieved disease control (stable disease or better). In these patients, POM + LoDEX demonstrated a statistically significant improvement in PFS vs. HiDEX (4.9 vs. 2.8 months; P<0.001). Even when patients whose best response was stable disease were analyzed alone, POM + LoDEX still significantly improved PFS vs. HiDEX (3.5 vs. 2.5 months; P=0.034). A number of patients who did not respond within the first 2 to 3 treatment cycles subsequently did achieve a response (or PR). In POM + LoDEX- vs. HiDEX-treated patients, 58 vs. 5, 16 vs. 4, and 20 vs. 5 patients responded within 9 weeks, between 9 and 13 weeks, and after 13 weeks, respectively.
Survival and response based on prior treatment
PFS significantly favored POM + LoDEX vs HiDEX, regardless of number or type of prior therapies, and a similar trend was observed for OS (Figure 2). PFS and OS benefits were maintained in patients who had LEN-refractory disease (PFS: HR, 0.51 (95% CI, 0.41–0.64); OS: HR, 0.70 (95% CI, 0.55–0.90)), even in patients refractory to LEN as their last prior treatment (PFS: HR, 0.41 (95% CI, 0.28–0.62); OS: HR, 0.56 (95% CI, 0.36–0.88)).
Figure 2.
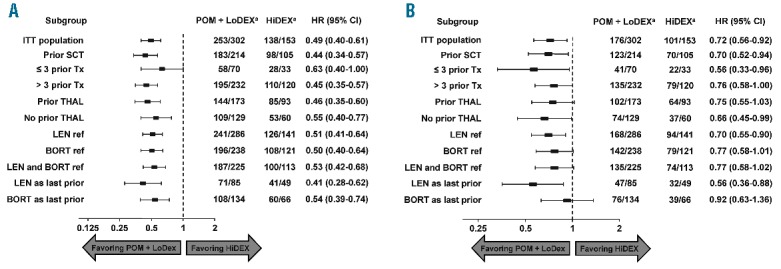
Forest plot of progression-free survival (A) and overall survival (B) based on prior treatment. aNumber of events/number of patients. BORT: bortezomib; HiDEX: high-dose dexamethasone; HR: hazard ratio; ITT: intent-to-treat; LEN: lenalidomide; LoDEX: low-dose dexamethasone; POM: pomalidomide; ref: refractory; SCT: stem cell transplant; THAL: thalidomide; Tx: treatment.
Response rates to POM + LoDEX were similar regardless of number and type of prior therapies (Figure 3). Patients who were refractory to LEN (n=286), BORT (n=238), or both (n=225) had similar ORRs (30% vs. 31% vs. 29%). Response was not significantly different among patients who were refractory to LEN (n=85) or BORT (n=134) as last prior therapy (33% vs. 34%). ORR was similar between patients with (n=173) and without (n=129) prior treatment with THAL (31% vs. 34%) and in the 214 patients with prior stem cell transplant (31%).
Figure 3.
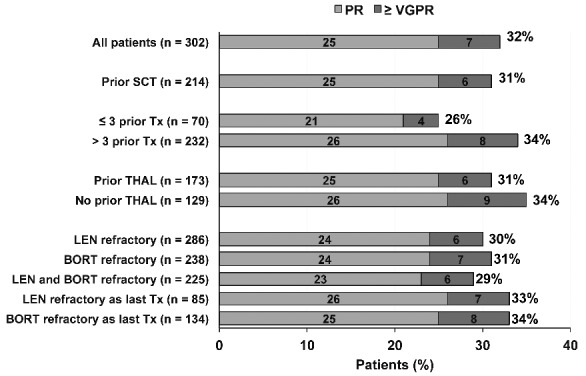
Response (by International Myeloma Working Group criteria) to POM + LoDEX treatment by prior therapy. Percentages may not sum to 100% due to rounding. BORT: bortezomib; LEN: lenalidomide; LoDEX: low-dose dexamethasone; POM: pomalidomide; PR: partial response; SCT: stem cell transplant; THAL: thalidomide; Tx: treatment; VGPR: very good partial response.
TTP for patients treated with POM + LoDEX was significantly longer than that with their last line of therapy, although the difference is unlikely to be clinically meaningful (median, 4.7 vs. 4.4 months; HR, 0.79; P=0.008). In contrast, patients treated with HiDEX progressed significantly more quickly than with their last prior line of therapy (median, 2.1 vs. 4.3 months; HR, 1.76; P<0.001; Figure 4).
Figure 4.
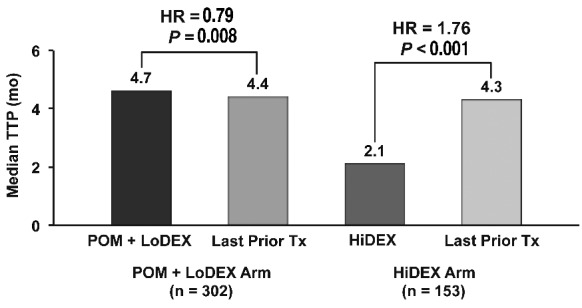
TTP on study compared with last prior therapy. HiDEX: high-dose dexamethasone; HR: hazard ratio; LoDEX: low-dose dexamethasone; POM: pomalidomide; TTP: time to progression; Tx: treatment.
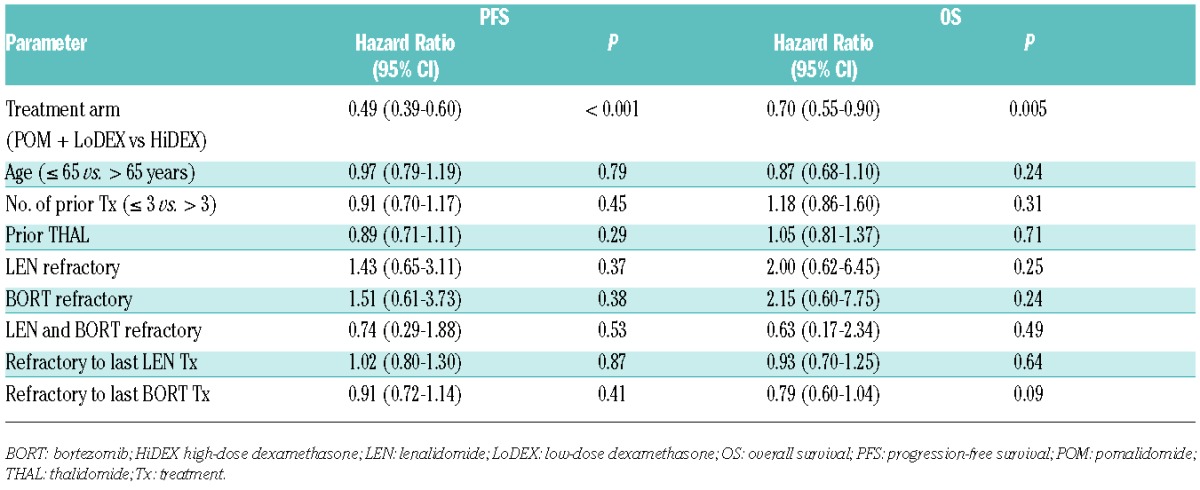
Multivariate analysis found that no variable relating to the number or type of prior treatments was a significant predictor of PFS or OS (Table 2). Factors analyzed included LEN or BORT as last prior therapy and LEN-, BORT -, or double-refractory status.
Table 2.
Multivariate analysis for PFS and OS.
Survival based on depth of response
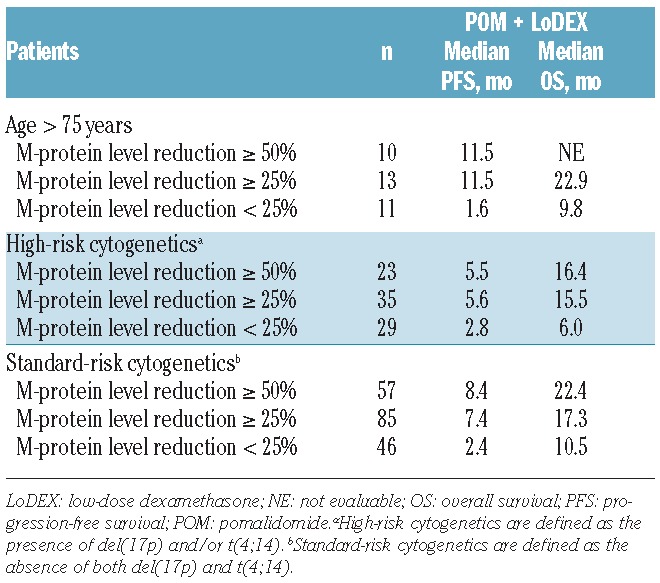
PFS and OS were assessed in patients according to the level of reduction in M-protein levels on POM + LoDEX treatment. Median PFS in POM + LoDEX-treated patients with reductions of < 25%, ≥ 25%, and ≥ 50% was 2.3, 7.4, and 8.4 months, respectively. Median OS in POM + LoDEX-treated patients with reductions of < 25%, ≥ 25%, and ≥ 50% was 7.5, 17.2, and 19.9 months, respectively (Figure 5). The trend associating a greater level of M-protein response with longer PFS and OS was also seen in very elderly patients (> 75 years), and in patients both with and without high-risk cytogenetic factors (Table 3).
Figure 5.
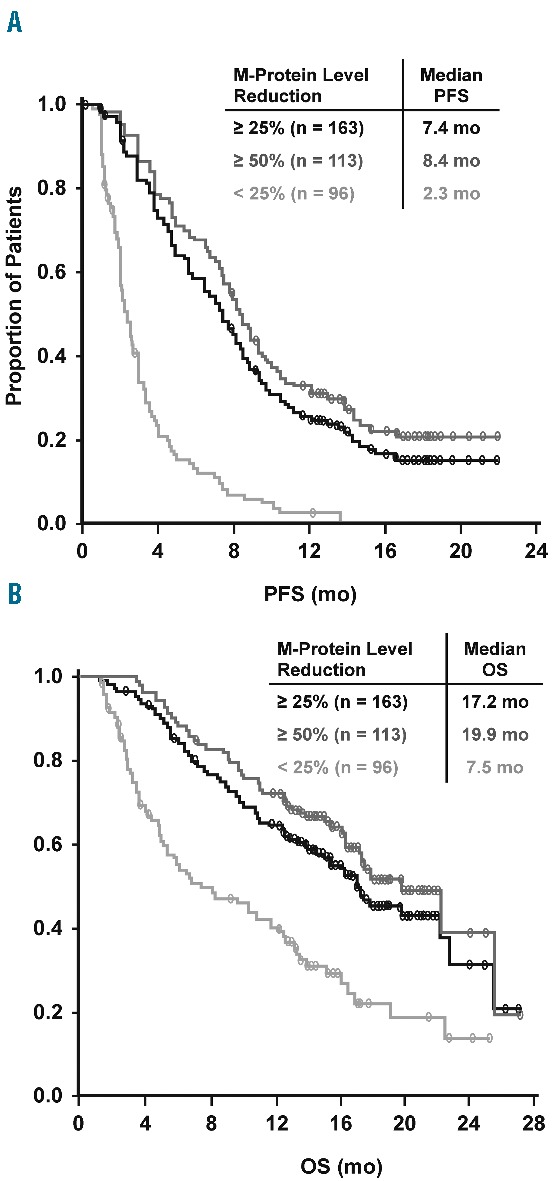
PFS (A) and OS (B) by depth of response measured by degree of M-protein level reduction for patients assigned to POM + LoDEX. LoDEX: low-dose dexamethasone; OS: overall survival; PFS: progression-free survival; POM: pomalidomide.
Table 3.
Survival by depth of response in very elderly (> 75 years) and cytogenetic risk groups.
Discussion
Initial MM-003 results, with a median follow-up of 10 months, demonstrated significantly longer PFS and OS for patients who received POM + LoDEX than for those who received HiDEX.22 Longer follow-up (median, 15.4 months) has confirmed significant PFS (4.0 vs. 1.9 months; P<0.001) and OS (13.1 vs. 8.1 months; P=0.009) benefits for POM + LoDEX vs HiDEX.22 Our subanalysis has shown that these benefits are generally maintained regardless of the number or type of prior therapies, including in patients with ≤ 3 and > 3 prior therapies, with or without prior THAL exposure, with LEN or BORT as last prior therapy, and refractory to LEN, BORT, or both. Multivariate analysis also found no effect of prior treatment on PFS or OS. This analysis demonstrated that approximately one-third of heavily pretreated patients (> 3 prior lines of therapy) will responded to POM + LoDEX. These findings are consistent with results from the phase 2 MM-002 study comparing POM + LoDEX with single-agent POM, in which PFS and OS in POM + LoDEX-treated patients were similar regardless of prior therapies or last prior therapy.18
The current analysis showed that benefits of POM + LoDEX treatment remained consistent regardless of prior treatment, even after repeated agents of the same class. This is a relevant finding in that it fails to support the usual assumption of cross-resistance between drugs of the same class; in fact, at least partial resistance has been suggested when carfilzomib is given immediately following BORT.10 Specifically, the ORR for patients treated with POM + LoDEX after LEN as last prior treatment was 33%, similar to the 32% for the overall POM + LoDEX population, indicating that there is no cross-resistance between POM and prior treatment with an immunomodulatory agent. This is consistent with in vitro data demonstrating antimyeloma effects of POM on LEN-resistant MM cell lines.25,26 These results support the use of immunomodulatory agents in succession, and show that prior LEN treatment should not preclude the use of POM.
Depth of response to POM + LoDEX was associated with a survival benefit for patients achieving a ≥ 25% reduction in M-protein levels. This pattern was consistent in very elderly patients (> 75 years) and those with high-risk cytogenetics, demonstrating that a ≥ 25% reduction in M-protein levels predicts PFS and OS benefits even in these populations with a poor prognosis. The benefit is even more evident for patients achieving a reduction of ≥50% in M-protein levels. Depth of response in other studies has also been found to be associated with longer PFS and/or OS in patients previously exposed to novel agents; these include trials of single-agent carfilzomib,10 POM in combination with cyclophosphamide and prednisone,27 and combination therapy with panobinostat, BORT, and DEX.28
These subanalyses of MM-003 data further support that POM + LoDEX can provide consistent clinical benefits and tolerability to patients with RRMM regardless of prior therapy. This regimen should be considered a standard of care in this patient population.
Acknowledgments
The authors thank the patients who volunteered to participate in this study, staff members at the study sites who cared for them, and representatives of the sponsors who were involved in data gathering and analyses. We also thank Richard Balzer, PhD, and Nicola Hanson, PhD, of MediTech Media for writing assistance, which was funded by Celgene Corporation.
Footnotes
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Brenner H, Gondos A, Pulte D. Recent major improvement in long-term survival of younger patients with multiple myeloma. Blood. 2008;111(5):2521–2526. [DOI] [PubMed] [Google Scholar]
- 2.Pulte D, Gondos A, Brenner H. Improvement in survival of older adults with multiple myeloma: results of an updated period analysis of SEER data. Oncologist. 2011;16(11): 1600–1603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Palumbo A, Bringhen S, Larocca A, et al. Bortezomib-melphalan-prednisone-thalidomide followed by maintenance with bortezomib-thalidomide compared with bortezomib-melphalan-prednisone for initial treatment of multiple myeloma: updated followup and improved survival. J Clin Oncol. 2014;32(7):634–640. [DOI] [PubMed] [Google Scholar]
- 4.Palumbo A, Hajek R, Delforge M, et al. Continuous lenalidomide treatment for newly diagnosed multiple myeloma. N Engl J Med. 2012;366(19):1759–1769. [DOI] [PubMed] [Google Scholar]
- 5.Attal M, Lauwers-Cances V, Marit G, et al. Lenalidomide maintenance after stem-cell transplantation for multiple myeloma. N Engl J Med. 2012;366(19):1782–1791. [DOI] [PubMed] [Google Scholar]
- 6.McCarthy PL, Owzar K, Hofmeister CC, et al. Lenalidomide after stem-cell transplantation for multiple myeloma. N Engl J Med. 2012;366(19):1770–1781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kumar SK, Lee JH, Lahuerta JJ, et al. Risk of progression and survival in multiple myeloma relapsing after therapy with IMiDs and bortezomib: a multicenter International Myeloma Working Group study. Leukemia. 2012;26(1): 149–157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wang M, Dimopoulos MA, Chen C, et al. Lenalidomide plus dexamethasone is more effective than dexamethasone alone in patients with relapsed or refractory multiple myeloma regardless of prior thalidomide exposure. Blood. 2008;112(12):4445–4451. [DOI] [PubMed] [Google Scholar]
- 9.Mateos MV, Richardson PG, Schlag R, et al. Bortezomib plus melphalan and prednisone compared with melphalan and prednisone in previously untreated multiple myeloma: updated follow-up and impact of subsequent therapy in the phase III VISTA trial. J Clin Oncol. 2010;28(13):2259–2266. [DOI] [PubMed] [Google Scholar]
- 10.Siegel DS, Martin T, Wang M, et al. A phase 2 study of single-agent carfilzomib (PX-171-003-A1) in patients with relapsed and refrac tory multiple myeloma. Blood. 2012; 120(14): 2817–2825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Palumbo A, Gay F, Bringhen S, et al. Bortezomib, doxorubicin and dexamethasone in advanced multiple myeloma. Ann Oncol. 2008;19(6):1160–1165. [DOI] [PubMed] [Google Scholar]
- 12.Niesvizky R, Richardson PG, Rajkumar SV, et al. The relationship between quality of response and clinical benefit for patients treated on the bortezomib arm of the international, randomized, phase 3 APEX trial in relapsed multiple myeloma. Br J Haematol. 2008;143(1):46–53. [DOI] [PubMed] [Google Scholar]
- 13.Harousseau JL, Dimopoulos MA, Wang M, et al. Better quality of response to lenalidomide plus dexamethasone is associated with improved clinical outcomes in patients with relapsed or refractory multiple myeloma. Haematologica. 2010; 95(10):1738–1744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kapoor P, Kumar SK, Dispenzieri A, et al. Importance of achieving stringent complete response after autologous stem-cell transplantation in multiple myeloma. J Clin Oncol. 2013;31(36):4529–4535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Morgan GJ, Davies FE, Gregory WM, et al. Cyclophosphamide, thalidomide, and dexamethasone (CTD) as initial therapy for patients with multiple myeloma unsuitable for autologous transplantation. Blood. 2011;118(5):1231–1238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Quach H, Ritchie D, Stewart AK, et al. Mechanism of action of immunomodulatory drugs (IMiDs) in multiple myeloma. Leukemia. 2010;24(1):22–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mark TM, Coleman M, Niesvizky R. Preclinical and clinical results with pomalidomide in the treatment of relapsed/refractory multiple myeloma. Leuk Res. 2014;38(5):517–524. [DOI] [PubMed] [Google Scholar]
- 18.Richardson PG, Siegel DS, Vij R, et al. Pomalidomide alone or in combination with low-dose dexamethasone in relapsed and refractory multiple myeloma: a randomized phase 2 study. Blood. 2014; 123(12):1826–1832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lacy MQ, Kumar SK, LaPlant BL, et al. Pomalidomide plus low-dose dexamethasone (Pom/Dex) in relapsed myeloma: long term follow up and factors predicing outcome in 345 patients [abstract 201]. Blood. 2012;120(21). [Google Scholar]
- 20.Leleu X, Attal M, Arnulf B, et al. Pomalidomide plus low dose dexamethasone is active and well tolerated in bortezomib and lenalidomide-refractory multiple myeloma: Intergroupe Francophone du Myélome 2009–02. Blood. 2013; 121(11):1968–1975. [DOI] [PubMed] [Google Scholar]
- 21.Leleu X, Karlin L, Macro M, et al. Pomalidomide plus low-dose dexamethasone in relapsed or refractory multiple myeloma (RRMM) with deletion (del)17p and/or translocation t(4;14) [abstract 689]. Blood. 2013;122(21). [Google Scholar]
- 22.San Miguel J, Weisel K, Moreau P, et al. Pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone alone for patients with relapsed and refractory multiple myeloma (MM-003): a randomised, open-label, phase 3 trial. Lancet Oncol. 2013;14(11):1055–1066. [DOI] [PubMed] [Google Scholar]
- 23.Durie BGM, Harousseau J, Miguel JS, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006; 20:1467–1473. [DOI] [PubMed] [Google Scholar]
- 24.Bladé J, Samson D, Reece D, et al. Criteria for evaluating disease response and progression in patients with multiple myeloma treated by high-dose therapy and haemopoietic stem cell transplantation. Myeloma Subcommittee of the EBMT. European Group for Blood and Marrow Transplant. Br J Haematol. 1998; 102(5):1115–1123. [DOI] [PubMed] [Google Scholar]
- 25.Ocio EM, Fernández-Lázaro D, San-Segundo L, et al. In vivo murine model of acquired resistance in myeloma reveals differential mechanisms for lenalidomide and pomalidomide in combination with dexamethasone. Leukemia. 2014;29(3):705–714. [DOI] [PubMed] [Google Scholar]
- 26.Lopez-Girona A, Mendy D, Ito T, et al. Cereblon is a direct protein target for immunomodulatory and antiproliferative activities of lenalidomide and pomalidomide. Leukemia. 2012;26(11):2326–2335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Larocca A, Montefusco V, Bringhen S, et al. Pomalidomide, cyclophosphamide, and prednisone for relapsed/refractory multiple myeloma: a multicenter phase 1/2 open-label study. Blood. 2013;122(16):2799–2806. [DOI] [PubMed] [Google Scholar]
- 28.San-Miguel JF, Hungria VT, Yoon SS, et al. Panobinostat plus bortezomib and dexamethasone versus placebo plus bortezomib and dexamethasone in patients with relapsed or relapsed and refractory multiple myeloma: a multicentre, randomised, double-blind phase 3 trial. Lancet Oncol. 2014; 15(11):1195–1206. [DOI] [PubMed] [Google Scholar]