

We read with interest the letter by Bifulco and Malfitano1 that argues that adiposity may be an underlying cause of cancer, and of acute lymphoblastic leukemia (ALL) in particular. Based on our recently published paper “The negative impact of underweight and weight loss on survival of children with acute lymphoblastic leukemia”2 and other studies, the authors suggest that the use of the entity “adiponcosis”, derived from the fusion of “adiposis” and “oncosis”, may be appropriate to support the hypothesis that adiposity increases the risk of ALL.
Although we appreciate existing knowledge that high body mass index may in part enhance cancer risk (either by ‘nature’ or by ‘nurture’),3 this particular issue was not the focus of our study. As stated in a letter by Renehan,4 it is important to differentiate between studies examining the link between excess weight and incidence of cancer and those that examine being overweight and cancer survival. We examined the influence of being underweight on relapse risk and survival in children with ALL, and did not address the influence of weight on ALL risk. Most studies that Bifulco and Malfitano refer to in order to support their hypothesis of “adiponcosis” with respect to “ALL” addressed excess weight as an accelerator of ALL progression, rather than oncogenetic aspects of the question.5–10
Nevertheless, there are many epidemiological studies that now show that excess weight is associated with increased risk for several common cancer types in adults, including breast cancer, cancer of the esophagus and ovaria.3 These studies suggest that hormonal influences have a substantial influence; however, such studies have not yet been performed in children.
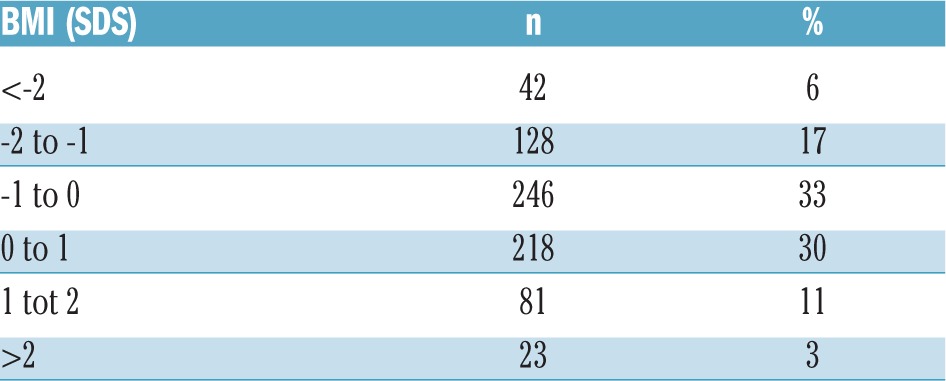
In our Dutch national study,2 including over 700 children, we have now analyzed the prevalence of being overweight and obese and compared this to healthy Dutch peers. The results show that the frequency of being overweight and obese [defined by a body mass index (BMI) of 20–25 kg/m2 and >30 kg/m2, respectively] at diagnosis was 6% and 1%, respectively (Table 1). BMI data standardized for sex and age [BMI standard deviation score (SDS)] were available for 738 patients, of whom 104 (14%) were overweight (11%) and 3% obese (Table 2). By way of comparison, according to the standard normal distribution, 16% of the matched healthy Dutch population has a BMI over 1 SDS and 2% has a BMI over 2 SDS. These results did not show that being overweight and obesity are more prevalent in children with ALL in the diagnostic phase, hence our data do not support the hypothesis that overweight children have an increased risk of developing ALL.
Table 1.
Prevalence of being overweight and obese in children with acute lymphoblastic leukemia at diagnosis by body mass index.
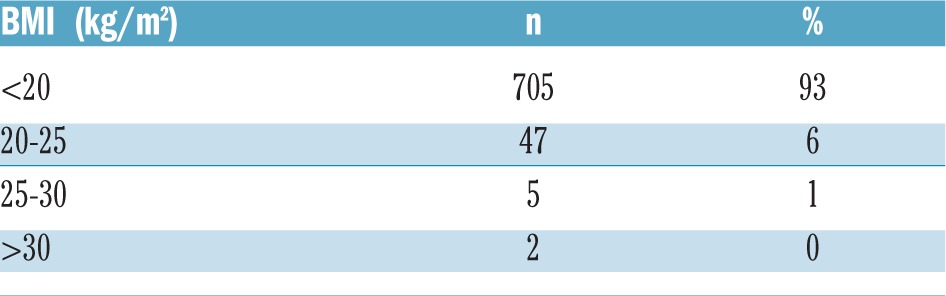
Table 2.
Prevalence of being overweight and obese in children with ALL at diagnosis by body mass index standardized deviation (SDS) category.
Although, epidemiological studies may give further insight into the existence of a link between adiposity and ALL, a direct causal relationship may be hard to show. We feel the suggested potential causative relationship of adiposity and ALL occurence, and consequently the true existence of the entity “adiponcosis” needs to be proven by further in vitro or in vivo research efforts, i.e. by xenograft models. By all means, further research on being overweight as a susceptibility marker for leukemogenesis is an attractive effort, to understand, at least in part, the molecular cause of ALL. It has been shown that obesity induces growth factor overexpression that induces cancer growth, and enhances further cancer growth due to the higher percentage of white adipose tissue (that is orchestrated by enhanced lipid signaling that accelerates the JAK-STAT and NF kappa beta pathway).11 Obesity may further enhance cancer growth by the influence of immune responses, inflammatory responses, insulin resistance and adipokine expression.12 Also, in pediatric solid tumors with overgrowth syndromes, the influence of endogenous growth factor exposure has been shown to facilitate the hyperproliferative processes of oncogenesis. In addition, pharmacokinetic and pharmaco-dynamic issues that are influenced by excess body weight, as discussed by Bifulco and Malfitano,1,13 are certainly important factors that may, in fact, be highly relevant for treatment success in particular.
Bifilico uses BMI as a potential predictive marker for being overweight. We and others have shown that BMI is an inferior method for assessment of true body composition. Methods measuring fat mass, e.g. Dual-X-Ray Absorptiometry (DXA), are preferable as they do not underestimate obesity and differentiate between muscle mass and fat mass.14,15 In a subset of our national cohort,2 body composition was assessed with DXA. We could show that, even in those cases that lost weight during treatment (decrease in BMI), fat percentage increased under dexamethasone treatment, illustrating the value of using measures of body composition instead of BMI.
Finally, one could argue whether the term “adiponcosis” is useful and relevant in clinical practice. We agree with the authors that controlling weight in children between 0–18 years of age is an important effort in current common health care to prevent metabolic syndrome, diabetes mellitus, cardiovascular diseases, impaired gonadal function, pulmonary disease and impaired quality of life.16 Although we could not show that being overweight was a prognostic marker, we agree that life style interventions may be of great benefit for children with ALL. This was further illustrated by the fact that, in our study, even the children with decreasing body mass index over time increased their body fat, but suffered from sarcopenia.2 This shows the value of physical exercise, although we realize that it is a challenge to design such interventions sufficiently that it can be maintained for the full period of ALL treatment.17
In summary, it still remains to be determined whether the definition of “adiponcosis” may survive over time as a clinical relevant entity, but we fully agree that the underlying mechanisms of adiposity as a risk factor for pediatric leukemia needs to be the focus of further attention by the scientific community.
Footnotes
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Bifulco M, Malfitano AM. Comment on “The negative impact of underweight and weight loss on survival of children with acute lymphoblastic leukemia. Acute lymphoblastic leukemia and adiponcosis. Haematologica. 2015;100(3):e118–1199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.den Hoed MA, Pluijm SM, de Groot-Kruseman HA, et al. The negative impact of underweight and weight loss on survival of children with acute lymphoblastic leukemia. Haematologica. 2015; 100(1):62–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Arnold M, Pandeya N, Byrnes G, et al. Global burden of cancer attributable to high body-mass index in 2012: a population-based study. Lancet Oncol. 2015;16(1):36–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Renehan AG. Obesity and cancer: links with survival differ from those with incidence. Ann Oncol. 2015;26(4):821. [DOI] [PubMed] [Google Scholar]
- 5.Yun JP, Behan JW, Heisterkamp N, et al. Diet-induced obesity accelerates acute lymphoblastic leukemia progression in two murine models. Cancer Prev Res (Phila). 2010;3(10):1259–1264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fuemmeler BF, Pendzich MK, Clark K, et al. Diet, physical activity, and body composition changes during the first year of treatment for childhood acute leukemia and lymphoma J Pediatr Hematol Oncol. 2013;35(6):437–443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Esbenshade AJ, Friedman DL, Smith WA, et al. Feasibility and initial effectiveness of home exercise during maintenance therapy for childhood acute lymphoblastic leukemia. Pediatr Phys Ther. 2014;26(3):301–307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Withycombe JS1, Smith LM, Meza JL, et al. Weight change during childhood acute lymphoblastic leukemia induction therapy predicts obesity: A report from the Children’s Oncology Group. Pediatr Blood Cancer. 2015;62(3):434–439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Orgel E, Sposto R, Malvar J, et al. Impact on survival and toxicity by duration of weight extremes during treatment for pediatric acute lymphoblastic leukemia: A report from the Children’s Oncology Group. J Clin Oncol. 2014;32(13):1331–1337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Orgel E, Tucci J, Alhushki W, et al. Obesity is associated with residual leukemia following induction therapy for childhood B-precursor acute lymphoblastic leukemia. Blood. 2014;124(26):3932–3938. [DOI] [PubMed] [Google Scholar]
- 11.Hiu Kiu, Nicholson Sandra E. Biology and significance of the JAK/STAT signalling pathways. Growth Factors. 2012;30(2):88–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Louie SM, Roberts LS, Nomura DK. Mechanisms linking obesity and cancer. Biochim Biophys Acta. 2013;1831(10):1499–508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bifulco M, Pisanti S. “Adiponcosis”: a new term to name the obesity and cancer link. J Clin Endocrinol Metab. 2013;98(12):4664–4665. [DOI] [PubMed] [Google Scholar]
- 14.Blijdorp K, van den Heuvel-Eibrink MM, Pieters R, Boot AM, Delhanty PJ, van der Lely AJ, Neggers SJ. Obesity is underestimated using body mass index and waist-hip ratio in long-term adult survivors of childhood cancer. PLoS One. 2012;7(8):e43269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shah NR, Braverman ER. Measuring Adiposity in Patients: The Utility of Body Mass Index (BMI), Percent Body Fat, and Leptin. PLoS One. 2012;7:e33308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pulgaron ER. Childhood obesity: a review of increased risk for physical and psychological comorbidities. Clin Ther. 2013;35(1):A18–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hartman A, te Winkel ML, van Beek RD, et al. A randomized trial investigating an exercise program to prevent reduction of bone mineral density and impairment of motor performance during treatment for childhood acute lymphoblastic leukemia. Pediatr Blood Cancer. 2009;53(1):64–71. [DOI] [PubMed] [Google Scholar]