

Abstract
Purpose of review
Electric stimulation is a potent means of neuromodulation that has been used to restore hearing and minimize tremor, but its application on tinnitus symptoms has been limited. We examine recent evidence to identify the knowledge gaps in the use of electric stimulation for tinnitus treatment.
Recent findings
Recent studies using electric stimulation to suppress tinnitus in humans are categorized according to their points of attacks. First, non-invasive, direct-current stimulation uses an active electrode in the ear canal, tympanic membrane or temporal scalp. Second, inner ear stimulation uses charge-balanced biphasic stimulation by placing an active electrode on the promontory or round window, or a cochlear implant array in the cochlea. Third, intraneural implants can provide targeted stimulation of specific sites along the auditory pathway. Although these studies demonstrated some success in tinnitus suppression, none established a link between tinnitus suppression efficacy and tinnitus-generating mechanisms.
Summary
Electric stimulation provides a unique opportunity to suppress tinnitus. Challenges include matching electric stimulation sites and patterns to tinnitus locus and type, meeting the oftentimes-contradictory demands between tinnitus suppression and other indications, such as speech understanding, and justifying the costs and risks of electric stimulation for tinnitus symptoms.
Keywords: Tinnitus, Electrical Stimulation, Direct Current, Charge-balanced pulses, Ear Canal, Eardrum, Transcranial Stimulation, Promontory, Round Window, Cochlear Implant, Auditory Brainstem Implant, Auditory Midbrain Implant, Cortical Stimulation, Vagus Nerve Stimulation, Sound Therapy
Introduction
It has been known for more than 200 years that electric stimulation of the auditory system not only evokes the sensation of sound (1), but also suppresses tinnitus (2). At present, electric stimulation via a cochlear implant has proven to be a safe and effective means of restoring hearing to over 400,000 deaf individuals worldwide. However, using electric stimulation to suppress tinnitus has not been thoroughly proven to be either safe or effective, and currently there are no established protocols or Food & Drug Administration (FDA)-approved products.
One reason for this lack of success is that tinnitus is usually treated as an added benefit of electric stimulation of the cochlea to restore hearing in deaf persons (3), rather than as the main indication. With increased awareness and prevalence of tinnitus as a result of presbycusis, noise exposure, or drug side effects, the need is greater than ever to develop safe and effective electric stimulation interventions for patients with debilitating tinnitus. In our opinion, there are no technical hurdles that can or should prevent translating electric stimulation to tinnitus treatment. So what are the problems? Here we examine the points of attack and existing evidence, and identify the opportunities and challenges in electric stimulation for tinnitus therapy.
Points of attack
There are three major points of attack categorized by the position of electrode placement. The first point of attack is electric stimulation, usually direct current (DC), through electrodes non-invasively placed in the external ear canal or tympanic membrane, or on the scalp (Figure 1). The second point of attack is the cochlea (Figure 2). Using a needle or ball electrode minimally-invasively placed in the promontory or round window, an alternating current (AC) with charge-balanced biphasic pulses is delivered to the inner ear. Additionally, a conventional cochlear implant placed in the scala tympani can provide cochlear electric stimulation. The third point of attack is to directly stimulate, usually with surgically-placed surface or penetrating electrodes, the neural elements of the auditory pathway, from the auditory nerve to the cochlear nuclei, inferior colliculus or even auditory cortex (Figure 3).
Figure 1. Direct current (DC) stimulation.
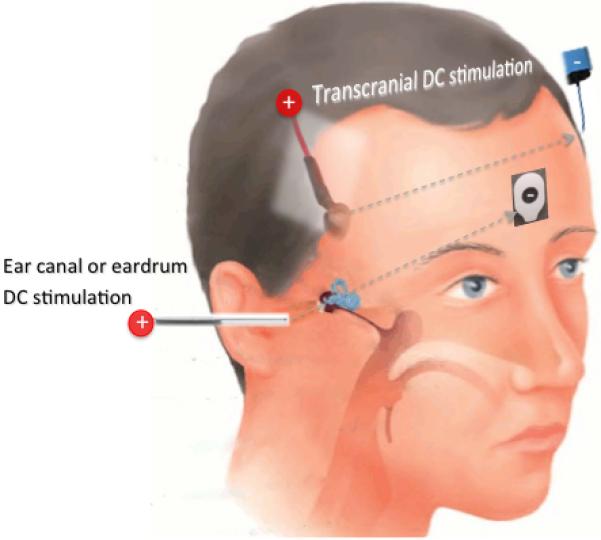
Two examples of DC stimulation are shown. One is ear canal stimulation, in which an active silver electrode (“+”) is placed in the saline-filled ear canal and a passive surface electrode is placed in the forehead. Such configuration would allow the current path (the lower dashed line) to pass the cochlea. Another example is transcranial DC stimulation, in which two surface electrodes are placed in the temporal lobe of each side, allowing current to pass the auditory cortex. The head picture is adapted with permission from: http://www.familydoctor.co.uk/wp-content/uploads/2013/10/tube.jpg
Figure 2. Stimulation of the inner ear.
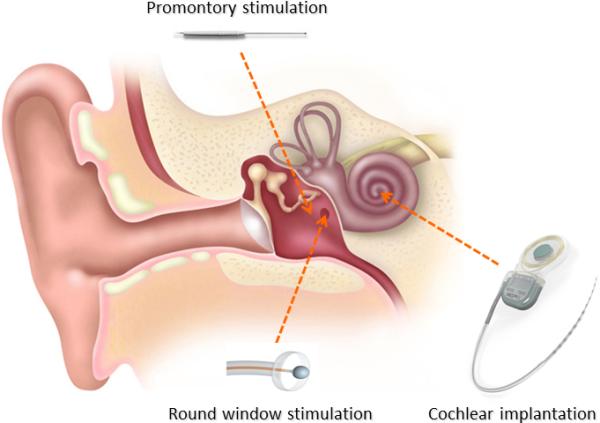
Stimulation of the inner ear includes stimulation of two extra-cochlear sites, promontory or round window and intra-cochlear stimulation via typically a cochlear implant. Promontory and round-window stimulation accesses mostly basal neurons while cochlear implantation can provide more place-specific stimulation from base to apex.
Figure 3. Stimulation of the auditory nerve pathway.
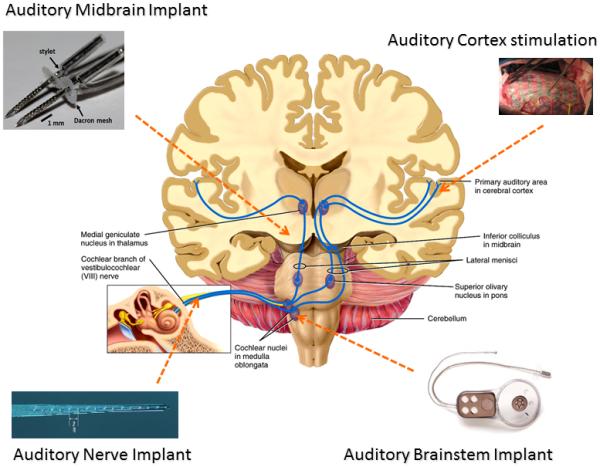
There are many places of attack along the auditory nerve pathway. Using penetrating electrodes to stimulate the auditory nerve trunk has been shown to produce selective activation in animals but not been tried in humans. Stimulation of the auditory brainstem, midbrain or cortex has all been used to suppress tinnitus in humans.
Figure 4 shows the various waveform patterns of electric stimulation, including DC, DC pulses, and charge-balanced biphasic pulses. DC stimulation is generally used in the ear canal and with transcranial stimulation but is typically avoided with inner ear or nerve stimulation due to its promotion of bone growth and long-term toxicity to the neural tissue. DC stimulation can be anodic or cathodic, as well as non-periodic (traces 1 and 2) or periodic (traces 3 and 4). The charge-balanced biphasic pulses (bottom trace) contain no DC and have been proven to be safe for long-term stimulation. For both DC and AC stimulation modes, fine adjustments in current amplitude are required to deliver an optimal level of current that is sufficiently high to produce a tinnitus suppression benefit but not so high as to cause an overly loud sound, pain, or other uncomfortable sensations. The pulse rate (inverse of the period “T”) can also vary from low (e.g., several Hz) to high (e.g., several kHz), or even to be matched to the tinnitus frequency.
Figure 4. Electric stimulation waveforms.
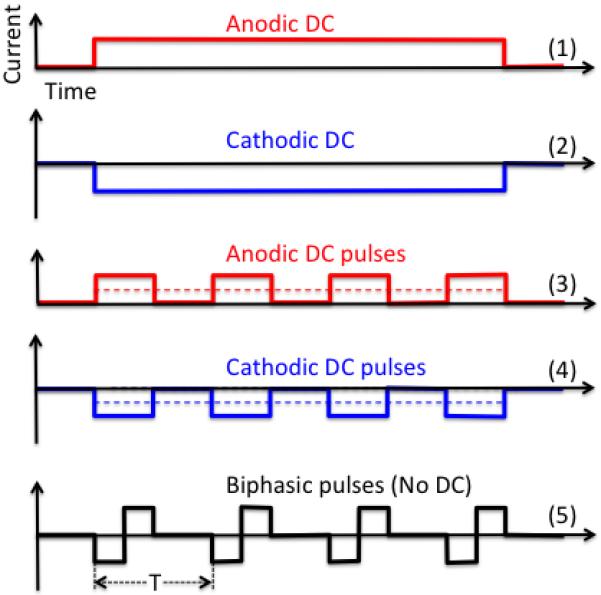
Trace 1 shows anodic direct current stimulation and trace 2 shows cathodic direct current stimulation. Traces 3 and 4 show anodic and cathodic DC pulses, respectively, in which the half duty cycle effectively reduces the DC amplitude to half of the peak amplitude (dashed line). Trace 5 shows charge-balanced, biphasic pulses, which contain no DC and are widely used in nerve stimulation.
Existing Evidence
A PubMed search revealed a total of 251 papers related to electric stimulation and tinnitus, with 100 of them being published in the last 10 years and 48 in the last 5 years (http://www.ncbi.nlm.nih.gov; performed on April 24, 2015). There have been many interesting and encouraging animal studies, but here we only discuss recent selected publications that utilized electric stimulation to treat tinnitus in human subjects.
1. DC stimulation
Mielczarek and Olszewski (4) placed an active silver electrode in an ear canal filled with saline solution and a passive surface electrode on the forehead to deliver pulsatile DC stimulation. The idea for such electrode configuration was that the current would flow directly across the cochlea, which lies between the two electrodes. The treatment involved 15 applications of electric stimulation over approximately 30 days, including 3-4 applications a week with each application lasting 4 minutes. About a third of subjects in the experimental group reported disappearance of tinnitus immediately after electric stimulation, with ~10% of them maintaining the benefit 90 days after stimulation. In contrast, only 5-8% of the subjects in the control group (no electric stimulation) reported disappearance of tinnitus over the same period.
Joos et al. (5) placed an active surface electrode on the skin overlying the temporal lobe and a passive electrode in the contralateral arm to deliver either anodic or cathodic transcranial DC stimulation. In a within-subjects design involving 175 patients, they found a significant tinnitus suppression effect for both anodic and cathodic DC stimulation only at 2 mA amplitude. Because of the lack of a general DC polarity effect, which presumably affects the brain excitatory and inhibitory activities differentially, Joos et al. attributed their observations to overall disruption of abnormal cortical activity in tinnitus patients.
2. Stimulation of the inner ear
Promontory stimulation has been extensively studied for tinnitus suppression for its relatively easy and minimally invasive access. Perez et al. (6) used a transtympanic needle electrode to deliver charge-balanced pulsatile stimulation to the promontory in 10 chronic tinnitus subjects. The Perez study differed from previously-described work in two aspects: they delivered 3 consecutive 30-minute stimulation sessions, every other day, and 7 of their 10 subjects had normal or mild hearing loss (PTA≤40 dB HL at 0.5, 1, 2 and 4 kHz). The within-subjects comparison showed significant tinnitus reduction during or immediately after the multiple treatment sessions, and return to baseline after 4 weeks in 50% of the subjects.
Reconfiguring a Neurelec cochlear implant, Wenzel et al. (7) attached a non-penetrating ball electrode, effectively a single-channel cochlear implant, to the round window in 3 subjects who suffered from single-sided deafness and tinnitus but had essentially normal hearing on the contralateral side. The charge-balanced, low-rate (≤100 Hz), long-term (4 hours per day for 3.5 years) stimulation improved at least one aspect of the tinnitus measures in all patients. Eventually in all 3 subjects, the round window implant was removed and replaced with a conventional cochlear implant, but no direct comparison was reported in tinnitus suppression between the two implants.
To address the site of stimulation question, Punte et al. (8) compared levels of tinnitus suppression achieved by electric stimulation of the 4 most basal electrodes (nearest to the round window) to those of the entire 12 intra-cochlear electrodes in 7 single-sided deafened subjects who also suffered from chronic tinnitus and received a Med-El cochlear implant. They found no tinnitus suppression from basal stimulation but significant suppression from full array stimulation during a 6-month evaluation period. In contrast, a site of stimulation effect was not found, even when electric pitch was matched to tinnitus pitch, in two systematic studies involving a total of 24 tinnitus subjects who had a conventional cochlear implant (9, 10). These two studies found that one or more stimulation patterns could totally abolish tinnitus in most subjects, suggesting that electric stimulation via a cochlear implant is an effective means for tinnitus suppression, but the challenge is to identify and optimize the effective stimuli.
3. Stimulation of the auditory nerve pathway
Similar to the cochlear implant, both the auditory brainstem implant and the deep brain stimulator have been shown to suppress tinnitus as an added benefit to restoring hearing or reducing tremor (11-13). However, chronic (1-6 years), direct stimulation of the auditory cortex by epidural electrodes did not produce any significant tinnitus suppression in a prospective, long-term, well-controlled study involving 9 subjects with severe chronic tinnitus (14). In 4 of the subjects, cortical stimulation reduced tinnitus severity or tinnitus-related symptoms, suggesting either imprecise stimulation of the auditory cortex or insufficiency of cortical stimulation alone.
In a case study involving a subject with traumatically-induced, intractable chronic tinnitus that contained both tonal and noise components on the right side, De Ridder and Vanneste (15) found that cortical stimulation abolished the subject’s tonal tinnitus, while additional spinal cord stimulation at C2 reduced his noise-like tinnitus. Interestingly, the suppressive effect was maintained for at least 5 years, compared with only 3 months by transcranial electrical nerve stimulation. The utility of the multitarget stimulation idea also received support from another interesting case study (16), in which sound therapy paired with vagus nerve stimulation produced a significant benefit in a subject with intractable chronic tinnitus.
Opportunities and Challenges
Recent studies have suggested that electric stimulation can potentially be a potent means for suppressing tinnitus, but significant challenges remain.
1. Mechanism-based treatment
Tinnitus is related to a number of different factors from hearing loss to acoustic trauma and drug side effects. The most significant challenge is to identify the mechanisms underlying tinnitus and its comorbid symptoms on an individual, patient-specific basis. For example, if we can determine that a lack of spontaneous neural activity is the primary etiology in a patient, we can design proper electric stimulation from direct current to high rate stimulation to restore the spontaneous activity (17, 18). Alternatively, if tinnitus etiology is due to highly synchronous, or bursting, or other aberrant cortical activities, then a neural modulator similar to deep brain stimulation can be implanted and programmed to alter these aberrant activities. If the etiology were related to network imbalance, then stimulation of multiple sites would be needed for eradicating the root cause of this type of tinnitus. Finally, if tinnitus is comorbid with hyperacusis, then its effective treatment may require treating hyperacusis first with an entirely different form of electric stimulation.
2. Precise and targeted treatment
In addition to mechanisms-based stimulation, we need to determine whether and how the location of tinnitus (in the ear or inside the head, on one side or both) or the types of tinnitus (tones or noise) requires different types and patterns of electric stimulation. Ear canal or transcranial stimulation is non-invasive but cannot provide targeted stimulation because current flows through paths determined by resistance, and not by distance. The complexity of biological tissues is likely to produce a diffuse pattern of imprecise stimulation. In subjects with high-pitched tinnitus and normal audiograms, promontory or round window stimulation seems to be the most appropriate intervention because its minimally-invasive approach will unlikely affect hearing while likely providing stimulation to the basal turn neurons that over time have detached from the inner hair cells. Conversely, nerve implants, albeit invasive, can provide precise and targeted stimulation to the auditory nerve, brainstem, or cortex. There is no significant technical hurdle from device safety to surgical approach, but the challenge is to decide which type of nerve implant is best suited for an individual tinnitus subject.
3. Optimal and integrated stimulation
Stimulation parameters are also critical to the safety and efficacy. DC stimulation is not desirable because over time it promotes bone growth and is toxic to neural tissues. Charge-balanced stimulation is preferred, but the challenge is to determine optimal parameters in terms of rate, level, mode and pattern of stimulation for specific tinnitus characteristics. Recently, two additional opportunities have emerged. The first is to combine electric stimulation with sound therapy or use multimodal stimulation for improved likelihood of success and efficacy (19, 20). The second is to integrate electric stimulation to optimize both tinnitus suppression and speech recognition in unilaterally or bilaterally deafened subjects (9). The challenge is to meet the oftentimes-contradictory demands in electric stimulation between effective tinnitus suppression and optimal speech recognition.
Conclusion
Electric stimulation has successfully restored partial hearing to 400,000 individuals with severe to profound hearing loss, but neither its safety nor efficacy has been established in tinnitus treatment. Here we examine recent evidence and conclude that the lack of established protocols is due to insufficient understanding of tinnitus generation mechanisms, preventing delivery of precise and targeted electric stimulation to the proper site. The opportunities are ripe with regard to surgical techniques and implantable devices, but the challenges are to identify the appropriate site of electric stimulation and to optimize the stimulation delivery patterns for each and every individual tinnitus subject.
Key points.
Electric stimulation, particularly the charge-balanced AC stimulation, is safe and can potentially suppress tinnitus if both the place and pattern of stimulation are properly matched to the nature of tinnitus.
DC stimulation via ear canal, eardrum or transcranial electrodes is unlikely to provide precise and targeted electric stimulation, thus limiting its utility and potential efficacy.
Promontory or round-window stimulation is appropriate for subjects with high-frequency tinnitus and normal audiograms because its minimally-invasive approach will likely preserve hearing while stimulating the basal turn neurons that might be detached from the inner hair cells.
Cochlear implants are strongly indicated for tinnitus subjects with hearing loss, but the challenge is to balance the needs in using electric stimulation to suppress tinnitus while preserving speech understanding.
Neural implants placed from the auditory nerve to the cortex or even the vagus nerve have the potential to provide the most precise and targeted stimulation, but the challenge is to match the site of stimulation to tinnitus type, while justifying the cost and risks of surgery against the potential benefits of tinnitus suppression.
Acknowledgements
We thank Thomas Lu for help in preparing the illustrations used here. The work was partially supported by the National Institutes of Health (P30-DC008369) and the Thomas and Misako Yuen Family Foundation. FGZ has an equity interest in the Nurotron Biotech and SoundCure, Inc., whose business is related to research discussed here. HRD’s research has been supported by the Institutional Clinical and Translational Sciences Center at the University of California Irvine and the Wareham Family Foundation. HRD has an equity interest in Mind:Set Technologies (beyondtinnitus.com) which has business related to tinnitus. The terms of both FGZ and HRD’s interests have been reviewed and approved by the University of California, Irvine, in accordance with its conflict of interest policies.
References
- 1.Volta A. On the electricity excited by mere contact of conducting substances of different kinds. Royal Soc Philos Trans. 1800;90:403–31. [Google Scholar]
- 2.Althaus J. On tinnitus aurium and its treatment by electricity. Lancet. 1886;128(3283):205–6. [Google Scholar]
- 3.House WF. Cochlear Implants. Annals Otol Rhinol Laryngol. 1976;85(Suppl.27):1–52. [PubMed] [Google Scholar]
- 4.Mielczarek M, Olszewski J. Direct current stimulation of the ear in tinnitus treatment: a double-blind placebo-controlled study. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies. 2014;271(6):1815–22. doi: 10.1007/s00405-013-2849-6. * A unique feature was to set the rate of cathodic DC pulses to matched tinnitus frequency. Another mysterious finding was that subjects in the experimental group had ~5 dB increase in audiometric thresholds at 125 Hz, ~5 dB decrease (improved hearing) between 1000 and 4000 Hz, and no change at high frequencies after stimulation. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Joos K, De Ridder D, Van de Heyning P, Vanneste S. Polarity specific suppression effects of transcranial direct current stimulation for tinnitus. Neural plasticity. 2014;2014:930860. doi: 10.1155/2014/930860. * Different from a bicephalic electrode positioning (see Figure 1) in most previous studies, they placed the reference electrode on the contralateral arm, minimizing its interference. Nevertheless, no difference was observed between anodic and cathodic stimulation. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Perez R, Shaul C, Vardi M, Muhanna N, Kileny PR, Sichel JY. Multiple electrostimulation treatments to the promontory for tinnitus. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2015;36(2):366–72. doi: 10.1097/MAO.0000000000000309. * Significant negative correlation was found between tinnitus duration and suppression efficacy, suggesting the importance of timely application of electric stimulation in effective tinnitus treatment. [DOI] [PubMed] [Google Scholar]
- 7.Wenzel GI, Sarnes P, Warnecke A, Stover T, Jager B, Lesinski-Schiedat A, et al. Non-penetrating round window electrode stimulation for tinnitus therapy followed by cochlear implantation. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies. 2014 doi: 10.1007/s00405-014-3413-8. * The eventual explanation of the Tinnelec implant in all 3 subjects suggested a need for a specially designed cochlear implant that treats tinnitus while providing hybrid or electric hearing in subjects who suffer from unilateral loss or bilateral loss with significant residual acoustic hearing. [DOI] [PubMed] [Google Scholar]
- 8.Punte AK, De Ridder D, Van de Heyning P. On the necessity of full length electrical cochlear stimulation to suppress severe tinnitus in single-sided deafness. Hearing research. 2013;295:24–9. doi: 10.1016/j.heares.2012.08.003. [DOI] [PubMed] [Google Scholar]
- 9.Chang JE, Zeng FG. Tinnitus suppression by electric stimulation of the auditory nerve. Frontiers in systems neuroscience. 2012;6:19. doi: 10.3389/fnsys.2012.00019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Arts RA, George EL, Chenault MN, Stokroos RJ. Optimizing intracochlear electrical stimulation to suppress tinnitus. Ear and hearing. 2015;36(1):125–35. doi: 10.1097/AUD.0000000000000090. * No universal trend was found for optimal stimulation, not even with pitch-matched electric stimulation, suggesting a need for customized programming in using cochlear implants to suppress tinnitus. [DOI] [PubMed] [Google Scholar]
- 11.Soussi T, Otto SR. Effects of electrical brainstem stimulation on tinnitus. Acta oto-laryngologica. 1994;114(2):135–40. doi: 10.3109/00016489409126031. [DOI] [PubMed] [Google Scholar]
- 12.Cheung SW, Larson PS. Tinnitus modulation by deep brain stimulation in locus of caudate neurons (area LC) Neuroscience. 2010;169(4):1768–78. doi: 10.1016/j.neuroscience.2010.06.007. [DOI] [PubMed] [Google Scholar]
- 13.Shi Y, Burchiel KJ, Anderson VC, Martin WH. Deep brain stimulation effects in patients with tinnitus. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2009;141(2):285–7. doi: 10.1016/j.otohns.2009.05.020. [DOI] [PubMed] [Google Scholar]
- 14.Engelhardt J, Dauman R, Arne P, Allard M, Dauman N, Branchard O, et al. Effect of chronic cortical stimulation on chronic severe tinnitus: a prospective randomized double-blind cross-over trial and long-term follow up. Brain stimulation. 2014;7(5):694–700. doi: 10.1016/j.brs.2014.05.008. * The negative result in this long-term study with a relatively large sample size suggested a need for precise and targeted cortical stimulation. [DOI] [PubMed] [Google Scholar]
- 15.De Ridder D, Vanneste S. Multitarget surgical neuromodulation: Combined C2 and auditory cortex implantation for tinnitus. Neuroscience letters. 2015;591:202–6. doi: 10.1016/j.neulet.2015.02.034. * The differential and integrated effects of cortical and spinal cord stimulation on tonal and noise tinnitus suggested a need for combined, multitarget stimulation. [DOI] [PubMed] [Google Scholar]
- 16.De Ridder D, Kilgard M, Engineer N, Vanneste S. Placebo-controlled vagus nerve stimulation paired with tones in a patient with refractory tinnitus: a case report. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2015;36(4):575–80. doi: 10.1097/MAO.0000000000000704. [DOI] [PubMed] [Google Scholar]
- 17.Norena AJ, Mulders WH, Robertson D. Suppression of putative tinnitus-related activity by extra-cochlear electrical stimulation. Journal of neurophysiology. 2015;113(1):132–43. doi: 10.1152/jn.00580.2014. [DOI] [PubMed] [Google Scholar]
- 18.Rubinstein JT, Tyler RS, Johnson A, Brown CJ. Electrical suppression of tinnitus with high-rate pulse trains. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2003;24(3):478–85. doi: 10.1097/00129492-200305000-00021. [DOI] [PubMed] [Google Scholar]
- 19.Teismann H, Wollbrink A, Okamoto H, Schlaug G, Rudack C, Pantev C. Combining transcranial direct current stimulation and tailor-made notched music training to decrease tinnitus-related distress--a pilot study. PloS one. 2014;9(2):e89904. doi: 10.1371/journal.pone.0089904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Markovitz CD, Hogan PS, Wesen KA, Lim HH. Pairing broadband noise with cortical stimulation induces extensive suppression of ascending sensory activity. Journal of neural engineering. 2015;12(2):026006. doi: 10.1088/1741-2560/12/2/026006. [DOI] [PMC free article] [PubMed] [Google Scholar]